


Abstract
Aim: To compare the outcome of 5-fluorouracil (FU)-based hepatic arterial infusion chemotherapy (HAIC) with sorafenib monotherapy in patients with hepatocellular carcinoma (HCC) refractory to transcatheter arterial chemoembolization (TACE). Patients and Methods: In this retrospective cohort study, 123 patients with HCC refractory to TACE, with Child-Pugh A and free of extrahepatic metastasis, were divided into two groups: 65 received HAIC and 58 received sorafenib. Since the size of main tumor and portal vein invasion were significantly different between the HAIC and sorafenib groups, we selected 48 patients from the 65 patients of the HAIC group and 48 from the 58 patients of the sorafenib group. The model used one-to-one matching between the two groups using the case–control method matching method. The clinical characteristics of patients of the case–control HAIC (n=48) and sorafenib groups (n=48) were similar. Overall survival, time to progression and time to treatment failure (TTTF) were compared between the two groups. Results: The median survival time and TTTF were significantly longer in the sorafenib group than in the HAIC group (15 and 12.2 months versus 8 and 4.4 months, respectively; p=0.021 and p=0.002, respectively). Multivariate analysis identified male gender (p=0.008), relative tumor size <50% (p=0.012), α-fetoprotein <400 ng/ml (p=0.005), and treatment with sorafenib (p=0.001) as significant and independent determinants of better overall survival. Conclusion: In patients with HCC refractory to TACE, overall survival was favorable in those treated with sorafenib rather than HAIC.
Several studies have reported on clinical benefits of sorafenib in patients with advanced hepatocellular carcinoma (HCC), including a placebo-controlled randomized phase III study (1) and a phase III study performed in the Asia-Pacific region (2). Sorafenib is currently the only standard therapy in many countries for patients with advanced HCC and extrahepatic metastasis, unresectable HCC, refractory to transcatheter arterial chemoembolization (TACE) and with macroscopic vascular invasion (MVI). Sorafenib is reported to prolong overall survival by 2.3-2.8 months and improve the response rate (RR) by 2.0-3.3%, compared to placebo (1). Sorafenib also has favorable results in patients with disease refractory to TACE compared to hepatic arterial infusion chemotherapy (HAIC) using cisplatin, with a significantly higher disease control rate, longer time to progression and increased overall survival (3).
HAIC is widely used in Asia, especially in Japan. The regimens used in HAIC include cisplatin only, interferon plus 5-fluorouracil (5-FU), or cisplatin plus 5-FU. Several studies have shown the survival benefits of HAIC for advanced HCC without extrahepatic metastasis, with response rates ranging from 20.8 to 52% (4-9). The reported median survival time (MST) in complete and partial responders is about 40 and 17 months, respectively (4-9). In the majority of retrospective studies, survival was significantly better in responders to HAIC than non-responders (5, 6). In HAIC, the response rate to sorafenib is usually high and responders have good overall survival (1, 6). However, the response rate and overall survival are poor in patients with extrahepatic metastasis (10). Furthermore, the survival of patients with Child-Pugh class B cirrhosis is significantly inferior to that of patients with Child-Pugh class A treated with HAIC (9), and the RR and overall survival are poorer in patients with disease refractory to TACE (11).
To our knowledge, there are no studies to have compared the benefits of 5-FU-based-HAIC treatment with sorafenib monotherapy in patients with HCC refractory to TACE. In this retrospective cohort study, we compared the response to HAIC therapy to that of sorafenib monotherapy in patients with TACE-refractory Child-Pugh A HCC, free from extrahepatic metastasis.
Patients and Methods
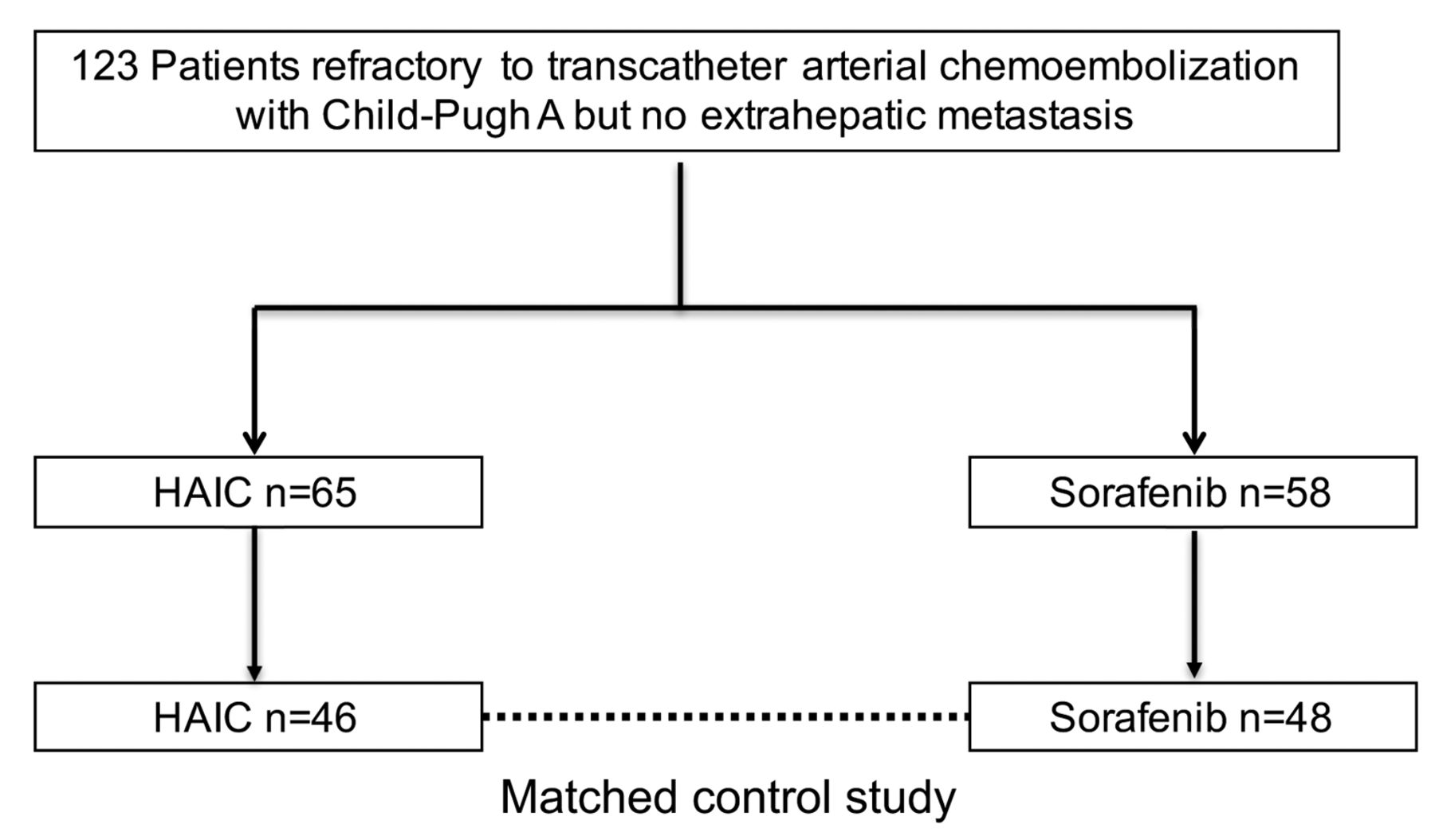
Patients. In this retrospective cohort study, among 325 patients treated by HAIC and 391 patients treated with sorafenib at our and affiliated hospitals, we enrolled only 123 patients with HCC, Child-Pugh A cirrhosis, free from extrahepatic metastasis and refractory to TACE. We excluded patients who were treated with both HAIC and sorafenib during the follow-up period. The study included 65 patients who received HAIC only and 58 who received sorafenib monotherapy.
Refractoriness to TACE was assessed radiologically on baseline computed tomography (CT)/magnetic resonance imaging (MRI) (taken within 3 months of TACE) according to the 2010 JSH Consensus Guidelines (12), and also by changes in tumor markers within 2 months of TACE. For the latter, persistent elevation of α-fetoprotein (AFP) within 2 months after TACE exceeding 20% relative to the baseline (before TACE) was considered non-response.
HAIC. HAIC consisted of repeated arterial infusions of anticancer agents via the injection port. Two drug regimens were used: intra-arterial low-dose cisplatin combined with 5-FU therapy (FP) and intra-arterial 5-FU with subcutaneous interferon (IFN) combination therapy (5-FU+IFN). One course of chemotherapy continued for 2 weeks. 5-FU at 300 mg/kg body weight/day was administered over 24 hours using a mechanical infusion pump from days 1 to 5 of the first and second weeks in both regimens. Cisplatin was injected intra-arterially at 6 mg/kg body weight/day on days 1-5 and 8-12. The IFN used in the 5-FU+IFN regimen was recombinant IFNα-2b or natural IFN-α, administered intramuscularly on days 1, 3, and 5 of each week (total dose, 36 and 60 MU, respectively). A 2- to 4-week rest period of no treatment was allowed after each treatment course (9). A total of 28 patients received FP, while 37 patients received 5FU+IFN.
Sorafenib monotherapy. Treatment with sorafenib was used between June 2009 and December 2015, at a dose of 400 mg twice daily. Treatment interruptions and dose reductions (to 400 mg once daily) were permitted for adverse drug reactions. Patients continued sorafenib monotherapy as long as possible, even when disease progression was noted, until death, or meeting one of the following criteria for cessation of therapy: adverse events that required termination of treatment, deterioration of Eastern Cooperative Oncology Group performance status (ECOG PS) to 4, worsening liver function, or withdrawal of consent. The criterion for liver function for treatment discontinuation was a total bilirubin level >3 mg/dl at 4 weeks after cessation of treatment.
Assessment of response to therapy and safety. The response to treatment was evaluated by the Response Evaluation Criteria in Solid Tumors (RECIST) (13) after completion of each course and at 8 weeks. As part of the assessment, each patient underwent dynamic CT or MRI every 3-4 months. Overall survival was assessed from the date of initiation of therapy until the date of death from any cause.
Safety was assessed by adverse drug reactions, clinical laboratory tests, physical examination, and measurement of vital signs. Adverse drug reactions were defined according to the Common Terminology Criteria for Adverse Events version 4.0 (14).
Statistical analysis. Continuous variables were expressed as the mean, while categorical variables were expressed as absolute and relative frequencies. Univariate analysis was used to investigate the relationship between overall survival of patients refractory to TACE after initiation of therapy and various clinicopathological variables. Overall survival was studied by Kaplan–Meier survival curves with log-rank survival comparisons and 95% confidence interval (CI). A Cox proportional hazards model was used to identify the prognostic factors for overall survival.
Since the size of the main tumor, portal vain invasion (Vp) and des-γ-carboxy prothrombin (DCP) were significantly different between the HAIC and sorafenib groups (see Results), we selected 48 patients from the 65 patients of the HAIC group and 48 from the 58 patients of the sorafenib group. The model used one-to-one matching between the two groups by using the case–control matching method (15).
A p-value less than 0.05 denoted the presence of a statistically significant difference. All statistical analyses were carried out with the Predictive Analytics Software v21.0 (IBM Corp., Armonk, NY, USA).
Results
Patients' clinical characteristics. Table I lists the differences between patients of the HAIC-treated and sorafenib-treated groups. Since the size of main tumor and Vp were significantly different between the two groups, we selected 48 patients from the 65 patients of the HAIC-treated group and 48 from the 58 patients of the sorafenib-treated group (Figure 1). The model used one-to-one match between the two groups by using the case–control method matching method. Table II shows that the clinical characteristics of patients of the case–control HAIC (n=48) and sorafenib groups (n=48) were similar. These patients met the study eligibility criteria and were matched for age, gender, etiology, platelet count, tumor size, Vp, TNM stage, Barcelona Clinic Liver Cancer Staging classification (BCLC), AFP, and DCP.
Characteristics of patients with hepatocellular carcinoma refractory to transcatheter arterial chemoembolization.
Characteristics of patients with hepatocellular carcinoma refractory to transcatheter arterial chemoembolization for the case–control method.
Response to therapy. The proportions of patients with complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD) were 0%,12%, 54% and 27% for the HAIC group, and 2%, 4%, 60%. and 27% for the sorafenib group. The response rate was similar for the HAIC and sorafenib groups (12% and 6%, p=0.4).
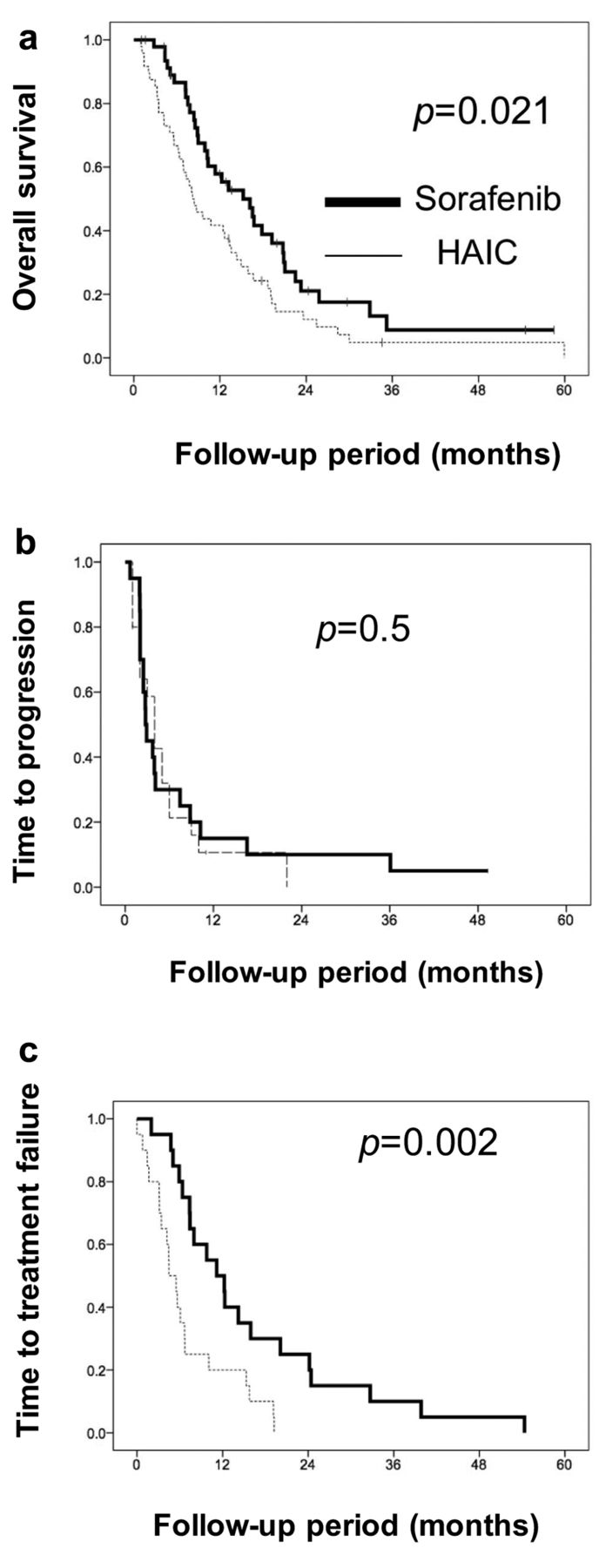
The median survival time was better in the sorafenib group (months) than the HAIC group (15 versus 8 months, p=0.021; Figure 2a). The time to progression was also similar (2.8 months versus 4.0 months, respectively, p=0.5; Figure 2b). The time to treatment failure was longer in the sorafenib group (12.2 versus 4.4 months, respectively, p=0.001; Figure 2c). For the MST of patients treated with HAIC, there was no significant difference between those treated with FP and those treated with 5-FU+IFN.

Flow-chart of patient recruitment.
The MST was longer in patients of the sorafenib group with CR (n=1). The MST of the patients with PR in the sorafenib (n=2) and HAIC (n=6) groups was 33 and 19 months, respectively (p=0.1); while for those with SD, the MST was 18 (n=29) and 12 (n=26) months, respectively (p=0.3). Furthermore, the MST of the patients with PD was 9 (n=13) and 3 (n=13) months, respectively (p=0.001).
Determinants of overall survival. Overall survival correlated significantly with gender (p=0.012), relative tumor size (p=0.049), Vp (p=0.0001), AFP (p=0.005) and treatment type (p=0.001). Multivariate analysis identified male gender (p=0.008) relative tumor size <50% (p=0.012), AFP <400 ng/ml (p=0.005), and treatment with sorafenib (p=0.001) as significant and independent determinants of better overall survival (Table III).
Overall survival according to MVI. In the HAIC group, the MST was not different between Vp0-2 (9 months) and Vp3-4 (7 month; p=0.5, Figure 3a), nor did it differ in the sorafenib group (12 versus 19 months, respectively, p=0.3; Figure 3b).
Adverse events. In the HAIC group, CTCAE grade 3/4 liver failure occurred in two patients (4.0%), hypersensitivity reaction to cisplatin in one patient (2.0%) and infection of the injection port in one (2.2%). In the sorafenib group, CTCAE grade 3/4 worsening of PS occurred in one patient (2.2%) and diarrhea and general fatigue in one patient (2.2%).
Discussion
Sorafenib is standard treatment for HCC refractory to TACE (16). The appearance of extrahepatic metastasis, MVI and enlargement of hepatic tumor are examples of lack of response to TACE. In this study, we selected patients with Child-Pugh A who were free of extrahepatic metastases and refractory to TACE. We also excluded patients who were treated with both HAIC and sorafenib during the follow-up period. In such patients, a switch to sorafenib is recommended rather than continuation of TACE (17). Another study reported that sorafenib is better than HAIC using cisplatin for HCC refractory to TACE (3). To our knowledge, however, there are no studies that compared sorafenib with HAIC using 5-FU for patients who failed se.to respond to TACE. For the above reasons, the present study was designed to compare the response to 5-FU-based HAIC and sorafenib in HCC refractory to TACE in patients with Child-Pugh A cirrhosis, free from extrahepatic metastasis.
Strict comparisons with previous studies is sometimes difficult since such studies included patients whose disease was not refractory to TACE and the patient selection process allowed potential biases. For example, in the study of Ikeda et al., 33% and 45% of patients treated with sorafenib and HAIC, respectively, had Child-Pugh B cirrhosis (3). This is important, since Child-Pugh B cirrhosis is a well-known poor prognostic factor in patients treated with sorafenib. Another limitation of the above study was inclusion of eight out of 66 (12%) patients who were switched from HAIC to sorafenib.
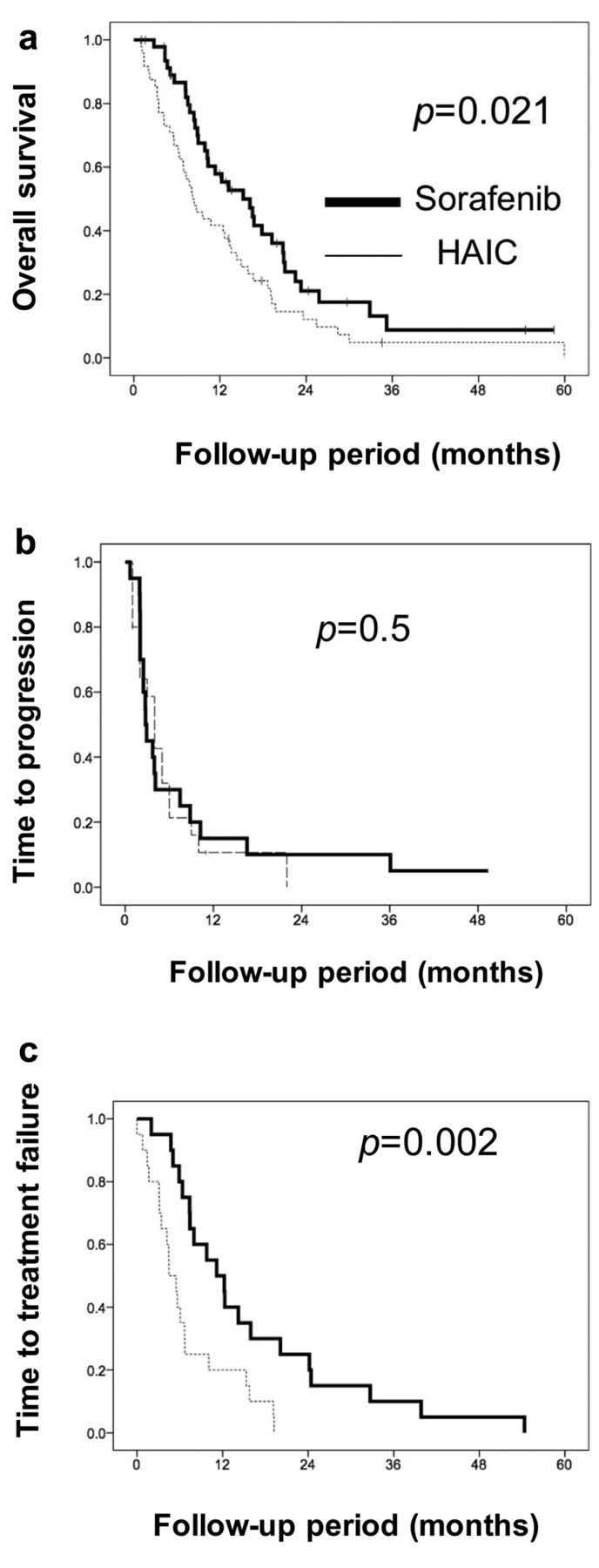
Overall survival (a), time to progression (b), and time to treatment failure (c) for hepatic arterial infusion chemotherapy (HAIC) and sorafenib in patients with hepatocellular carcinoma.

Overall survival after hepatic arterial infusion chemotherapy (HAIC) (a) and sorafenib (b) therapy of hepatocellular carcinoma according to portal vain invasion (Vp). Vp 0, No tumor thrombus; Vp, one tumor thrombus in the second branch of the portal vein; Vp 3, tumor thrombus in the first branch of the portal vein; Vp 4, tumor thrombus in the trunk of the portal vein.
Our results showed that sorafenib provided a better MST (15 months) than HAIC (8 months). The first reason for this is that the time to treatment failure of sorafenib is longer than HAIC: patients who received sorafenib were treated for a longer period than those treated with HAIC. The second reason is the need to withdraw treatment due to stenosis of the hepatic artery by catheter therapy, reduced sensitivity to the drug, deterioration of liver function, or the appearance of collateral arteries.
Results of univariate and multivariate analyses for prognostic factors in patients with hepatocellular carcinoma refractory to transcatheter arterial chemoembolization.
In both groups, the MST was not significantly different between Vp0-2 and Vp3-4. Generally, among patients with MVI, it has been reported that HAIC provides more favorable survival than sorafenib (18). However, in the present study, in which the subject was TACE-refractory patients, the superiority of HAIC to sorafenib was not demonstrated among patients with MVI. This might be due to stenosis of the hepatic artery by catheter therapy, or reduced sensitivity to the drug.
Our study has certain limitations. Firstly, the study included only a small number of patients and was retrospective in nature. However, we selected patients with Child-Pugh A cirrhosis who were free of extrahepatic metastasis and refractory to TACE. We also excluded patients who were treated with both HAIC and sorafenib during the follow-up period, thus allowing us to study selected groups of patients. We believe that the present study provides important information on the management of patients with HCC refractory to TACE.
In conclusion, sorafenib led to favorable overall survival among HCC patients refractory to TACE compared to those treated with HAIC. Further large-scale prospective studies are needed to compare the effects of HAIC with sorafenib.
- Received April 28, 2016.
- Revision received June 9, 2016.
- Accepted June 10, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.