


Abstract
Background/Aim: The nuclear factor erytheroid 2–related factor 2-kelch-like ECH-associated protein (NRF2-KEAP1) system and stem cell-like cancer cells are associated with platinum resistance in ovarian cancer. Our objective was to investigate the possible association between platinum resistance, cellular redox-state regulation and stem cell properties in ovarian cancer. Patients and Methods: Thirty-eight patients with epithelial ovarian cancer were included. All patients had undergone primary diagnostic laparoscopy, platinum-based neoadjuvant chemotherapy, and debulking surgery. Tumor samples were analyzed for NRF2, KEAP1, protein deglycase 1 (DJ1/PARK7), cluster of differentiation molecules 44 (CD44) and 117 (CD117) and aldehyde dehydrogenase 1 (ALDH1) by immunohistochemistry. Results: Positive pre-treatment expression of CD44 (p=0.013) and stable/increased post-therapy CD44 expression were associated with platinum resistance (p=0.001). Negative pre-treatment expression of cytoplasmic ALDH1 predicted sensitivity to platinum (p=0.017). Pre-treatment nuclear KEAP1 expression was greater in stage II-III cancer (p=0.0003). After neoadjuvant treatment, all samples were nuclear KEAP1-positive (p=0.025) and increased nuclear KEAP1 expression was associated with higher tumor stage (p=0.0001). Conclusion: CD44 and cytoplasmic ALHD1 could be potential indicators of platinum resistance during neoadjuvant chemotherapy for ovarian cancer.
Ovarian cancer is the leading cause of gynecological cancer-associated deaths. Most patients are diagnosed at an advanced state and the majority experience relapse within two years. Five-year survival at best is only 45% (1). The cornerstone of treatment is surgery and subsequent platinum-based chemotherapy. The use of neoadjuvant chemotherapy to postpone primary surgery has been controversial and the question of the risk of chemoresistance induced by neoadjuvant platinum-based treatment has been raised.
Nuclear factor erythroid 2-related factor 2 (NRF2) is the main sensor of cellular oxidative stress. Under basal conditions it is tethered to its cytoplasmic inhibitor, Kelch-like ECH-associated protein 1 (KEAP1). The disassociation of NRF2 from KEAP1 is triggered by oxidative stress, leading to NRF2 translocation to the nucleus and its binding to antioxidant response elements (AREs) in DNA together with small v-maf avian musculoaponeurotic fibrosarcoma oncogene homolog proteins, resulting in widespread expression of antioxidant proteins (2, 3). KEAP1 is able to remove NRF2 from AREs and stop antioxidant induction in the nucleus (4). Increased NRF2 expression has been detected in several malignancies, including malignant glioma (5) and endometrial cancer (6). There is also evidence (mainly in preclinical models) that NRF2 overexpression or loss of KEAP1 may induce cisplatin/oxaliplatin resistance in ovarian and colorectal cancer (2, 7-9).
Protein deglycase 1 (DJ1/PARK7) is a redox-regulated protein involved in diverse cellular processes such as chemotaxis, cell migration, cell adhesion, angiogenesis, apoptosis, cell–extracellular matrix interactions and immune regulation. DJ1 deactivates reactive oxygen species and protects cells from oxidative stress (10). By inhibiting apoptotic pathways, DJ1 overexpression increases the resistance of neoplastic cells to apoptosis (10).
Malignant tumors have a small proportion of cells that have stem cell-like properties. These cells have unlimited proliferative potential through self-renewal and they can differentiate to generate cells with limited proliferative potential that form the bulk of a tumor (11). Since cancer stem-like cells (CSLCs) are mostly in a dormant state, they can survive chemotherapy (12). In ovarian cancer, the presence of CSLCs is associated with poor survival and chemoresistance (13, 14). High tumorigenicity in xenograft models is taken as the gold standard for the identification of cancer stem cells (CSCs) or CSLCs, but they can also be identified by various cell surface markers such as cluster of differentiation 44 (CD44), aldehyde dehydrogenase 1(ALDH1) and cluster of differentiation 117 (CD117).
CD44 is a transmembrane glycoprotein and a principal receptor for hyaluronic acid, it activates intracellular survival pathways (15). The enzyme ALDH1 protects organisms from harmful aldehydes and cytotoxic drugs, since it catalyzes the oxidation of aldehydes to carboxylic acids (16). CD117, also known as KIT, is a surface marker of embryonic stem cells, hematopoietic stem cells and mesenchymal cells (17). It is a tyrosine kinase receptor for stem cell factor and initiates a broad program of signal transduction, that mediates cell survival, migration and proliferation (11).
The aim of this study was to investigate the possible association between platinum resistance, cellular redox-state regulation and stem cell properties in ovarian cancer.
Patients and Methods
The study involved 38 patients with epithelial ovarian cancer diagnosed and treated at Oulu University Hospital in 2004–2012. All patients had undergone primary diagnostic laparoscopy with tumor biopsies. Platinum-based neoadjuvant chemotherapy was given (minimum of two courses) before the second-look operation. After the second operation, platinum-based chemotherapy was continued for a total of six courses or until remission had been achieved. Pre-chemotherapy tissue samples were collected at the time of diagnostic laparoscopy and postchemotherapy samples at the time of debulking surgery. The samples from both operations were analyzed. In two cases, the preoperative sample was only cytological, and in another two cases, the postoperative sample was insufficient for immunohistochemistry. Thus, it was not possible to perform paired assessment of these samples. Clinical data (age, stage, grade, histology, cancer antigen 12-5 (CA 12-5), recurrence, time of death) were collected from hospital records (Table I). The median follow-up time was 37.5 (17-126) months. Platinum resistance was defined as disease recurrence earlier than 6 months after the last chemotherapy dose, or as cancer progression during the platinum-based chemotherapy, and chemosensitivity as recurrence later than 6 months after the last chemotherapy dose. There were 26 chemoresistant and nine chemosensitive patients in this set of data. In three cases, platinum resistance could not be evaluated as a result of cessation of chemotherapy for patient-related reasons.
Immunohistochemistry. Sections of 3.5 mm were cut from a representative paraffin block and placed on SuperFrostPlus glass slides (Menzel-Gläser, Germany). They were de-paraffinized in xylene and rehydrated in a descending series of ethanolic solutions, incubated in citrate buffer (CD44, ALDH1 and DJ1, pH 6.0; NRF2, KEAP1 and CD117, pH 9.0), boiled in a microwave oven for 17 min and cooled at room temperature before adding the primary antibody. For negative controls, the primary antibodies were replaced with phosphate buffered saline and serum isotype controls (Table II). One sample was cytological and fixed in alcohol.
Patients' characteristics.
Immunoreactivity was assessed by two observers (AL and MPE). The samples were categorized as negative if fewer than 5%, weakly positive if 5-50% and strongly positive if >50% of the malignant cells showed positive immunostaining. Nuclei were considered to be positive if over 5% were immunopositive.
Statistical analyses. IBM SPSS Statistics v. 21.0.0.0 for Windows(IBM Corporation, Armonk, NY, USA) was applied for statistical analysis. The reported p-values are from two-sided chi-square tests and from two-sided McNemar's tests. Survival was analyzed by using the Kaplan–Meier method with the log-rank test. Disease-free survival (DFS) was calculated from the operation date to the confirmed date of relapse and overall survival (OS) to the time of death or the last date in the patient record. Stage was divided in statistical analyses into either stage II-III or IV. Probability values below 0.05 were considered significant.
Ethical considerations. This study was approved by the Local Ethics Committee and the National Supervisory Authority for Welfare and Health (1339/05.01.00.06/2009).
Details of antibodies used.
Results
Pre-treatment antigen expression. Positive immunostaining was detected for CD117 in 10% of pre-treatment samples, CD44 in 67%, and cytoplasmic and nuclear expression of ALDH1 in 39% and 11%, NRF2 in 86% and 42%, KEAP1 in 100% and 86%, DJ1 in 97% and 94%, respectively.
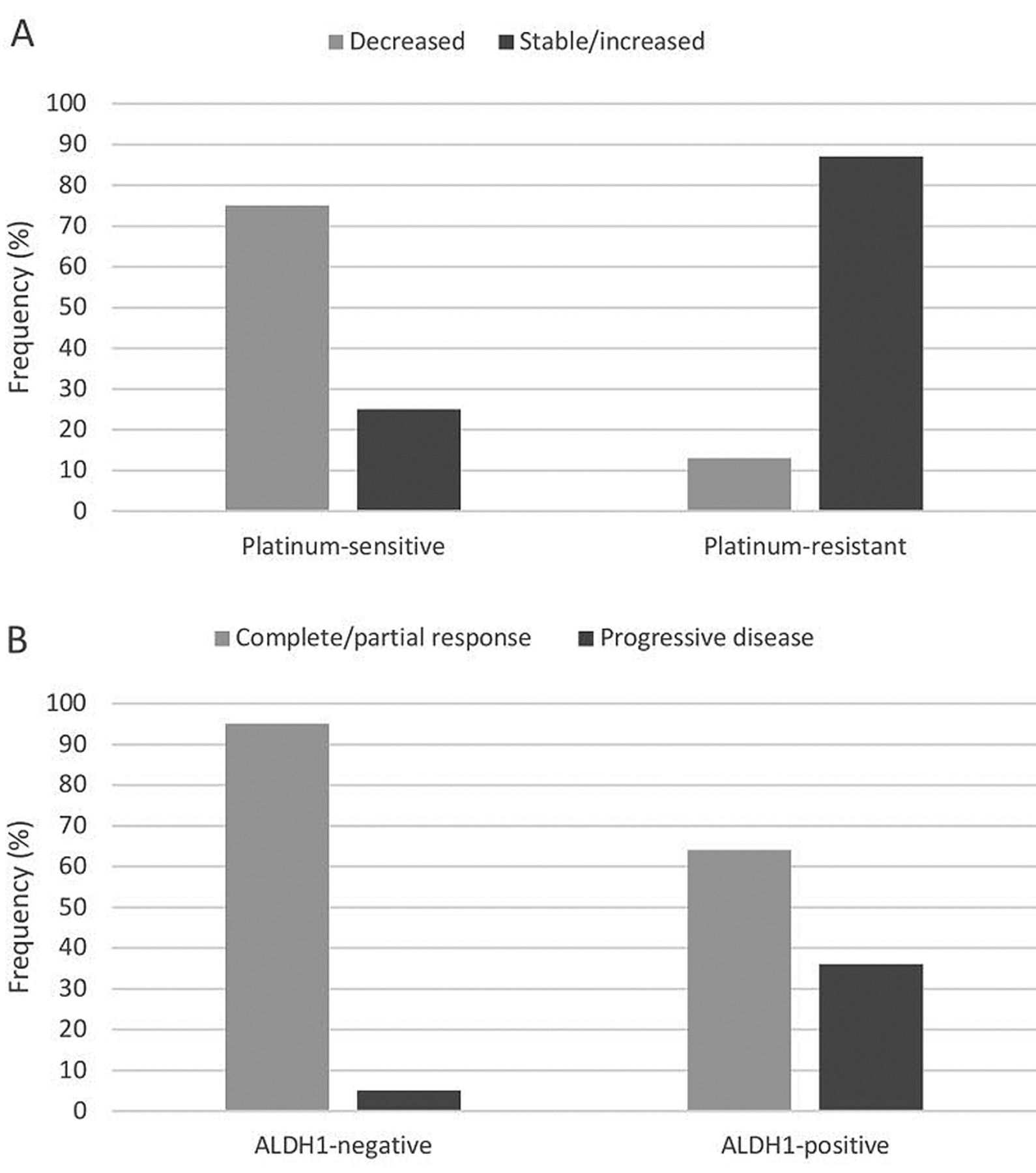
Cancer stem-like cell markers and platinum resistance. Negative pre-treatment CD44 expression correlated with increased platinum sensitivity (p=0.013) whereas positive CD44 expression did not. Increased or stable CD44 expression (compared to lower CD44 expression) after neoadjuvant treatment correlated significantly with platinum resistance (p=0.001). After treatment, CD44 expression had increased in 87% of patients with platinum resistance (Figure 1A). Negative pre-treatment cytoplasmic ALDH1 expression predicted significantly better responses to chemotherapy: only 1 out of 21 (5%) ALDH1-negative tumors did not show a response, while five out of 14 (36%) ALDH1-positive tumors progressed during the course of chemotherapy (p=0.017, Figure 1B). Combined pre-treatment negative CD44 and positive ALDH1 expression predicted platinum resistance (p=0.047), and none of these tumors were platinum-sensitive. Example of the staining patterns is shown in Figure 2. No correlations between CSLC characteristics and changes in OS or DFS were seen. There was no correlation between CD117 expression and platinum sensitivity or clinical parameters of the disease.
Redox-regulating enzymes and neoadjuvant therapy. Before neoadjuvant treatment, 14.7% of samples showed no nuclear KEAP1 expression, whereas after chemotherapy, all samples were nuclear KEAP1-positive (p=0.025, McNemar's test; Figure 3A, Table III). Pre-treatment nuclear KEAP1 staining was significantly greater at stage II-III when compared to stage IV (p=0.0003). The nuclei were KEAP1-positive in all cases (n=26) of stage II-III disease and in 55.5% (n=5) of stage IV cases. Increased nuclear KEAP1 expression post-therapy versus pre-therapy was associated with higher tumor stage (p=0.0001). There was a loss of cytoplasmic NRF2 expression after neoadjuvant therapy (p=0.016, McNemar's test; Figure 3B). Increased nuclear NRF2 expression after neoadjuvant treatment was borderline significantly associated with chemosensitivity (p=0.056). Pre-treatment nuclear ALDH1 positivity was associated with lower pre-treatment cytoplasmic NRF2 expression (p=0.034). Increased cytoplasmic DJ1 expression post-treatment versus pre-treatment was associated with stage IV disease (p=0.035). There were no significant correlations between the redox-regulating enzymes and survival or operability.

A: Percentage of cases showing a change in cluster of differentiation 44 (CD44) expression after neoadjuvant chemotherapy compared to pre-treatment expression of CD44 (p=0.001). B: Percentage of cases showing response to neoadjuvant platinum chemotherapy according to pre-treatment cytoplasmic expression of aldehyde dehydrogenase 1 (ALDH1). ALDH1-negative cases had better response than ALDH1-positive (p=0.017).

Immunohistochemical staining of cluster of differentiation 44 (CD44) and aldehyde dehydrogenase 1 (ALDH1) in ovarian cancer tissue. 100-fold magnification.
Discussion
We herein report that increased or stable CD44 expression after neoadjuvant platinum-based chemotherapy, negative pre-treatment CD44 expression and positive pre-treatment expression of ALDH1 are powerful predictive tools with regards the development of platinum resistance in epithelial ovarian cancer. Several studies have concerned the possible prognostic role of CD44 in epithelial ovarian cancer, but no consensus has been reached with regard to its clinical significance (18, 19) Recently, in ovarian cancer, CD44 was associated with higher tumor grade and stage (20) and metastatic ovarian cancer cells (21). Our results, thus, confirm a connection between increased CD44 expression and chemoresistance in ovarian cancer.
In rectal cancer, up-regulation of ALDH1 predicts poor prognosis but no change in ALDH1 expression between pre- and post-treatment samples was seen (22, 23). ALDH1 expression is associated with poor prognosis in breast (24) and cervical (25) cancer and uterine endometrioid adenocarcinoma (26). In pancreatic adenocarcinoma, ALDH1 expression was found to be greater in patients who received neoadjuvant chemoradiotherapy compared with those not treated with chemoradiation (27). In ovarian carcinoma, ALDH1 expression is associated with CD44 expression, chemoresistance, tumor progression and poor clinical outcome (16, 28-32). Our results, where ALDH1-expressing tumors were those with progressive behavior during chemotherapy, are in line with these findings. On the other hand, pre-treatment ALDH1 has been found to be a favorable prognostic factor in ovarian carcinoma (33). Several studies have revealed that CSLCs in vitro show aggressive growth and chemoresistance (16, 28, 30). However, there are several variables contributing to the function of CSLCs in vivo that make our clinical study valuable. The strength of our study is that we were able to assess both pre- and post-treatment samples from the same patient and evaluate the change of expression of CSLCs after chemotherapy for each individual tumor.
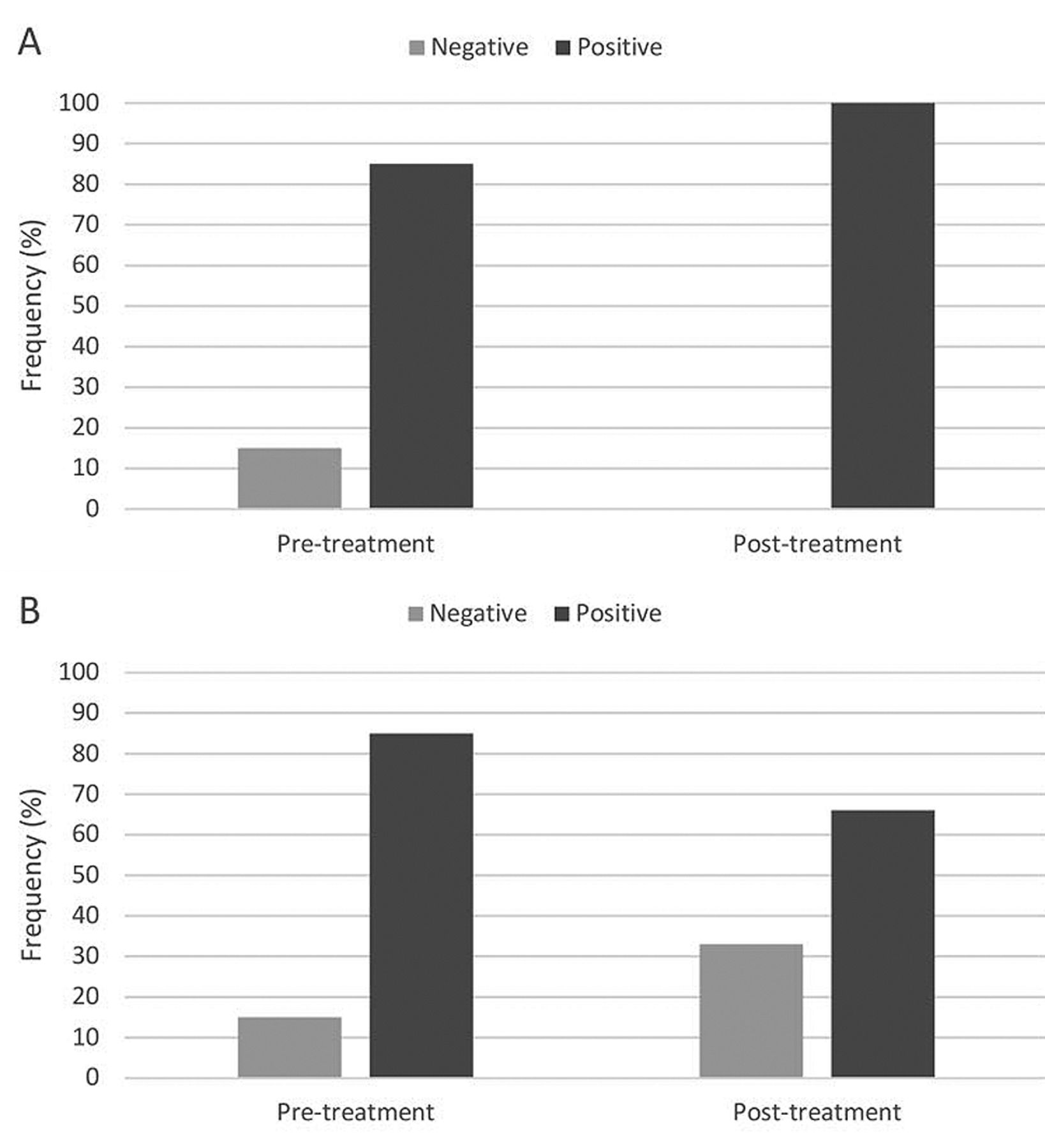
Frequency of expression of kelch-like ECH-associated protein (KEAP1) (A) and cytoplasmic nuclear nuclear factor erytheroid 2-related factor 2 (NRF2) (B) after neoadjuvant treatment compared to pre-treatment values. Differences were significant at p=0.025 and p=0.016, respectively.
Bonneau et al. (12) studied the immunohistochemical expression of CD44, ALDH1 and CD117 in epithelial ovarian cancer before and after chemotherapy (12). In contrast to our results they found that a decrease in CD44 expression after chemotherapy was associated with poor OS. Nevertheless, no correlation was found between CD44 expression and chemoresistance in their clinical material, although in vitro, CD44-positive cells had chemoresistant properties. A reduction in ALDH1 expression was associated with shorter DFS. The authors hypothesized that microscopic residual tumor composites of dormant CSLCs and a large proportion of rapidly dividing bulk cells may explain early recurrence. Our study group was relatively homogeneous and the prognoses of the patients were very poor per se, that may render comparison of progression-free survival and OS difficult. Additionally, for patients with platinum-resistant disease, other non-platinum-based forms of chemotherapy that have resulted in reasonable responses are available, which may also affect survival analysis. There was no correlation between expression of the different CSC markers in our study. It is probable that the cells expressing different CSC markers have their own signaling mechanisms and independent types of function.
Changes in the expression of markers after neoadjuvant treatment compared to pre-treatment values.
Increased DJ1 levels have been observed in association with gastric (34) and pancreatic (35) cancer. In breast cancer, weak DJ1 expression was reported to predict pathological complete remission after neoadjuvant chemotherapy (36). Increased serum and immunohistochemical DJ1 levels were found in endometrial serous cancer (37) and in ovarian cancer, and DJ1 was associated with advanced stage (38). In our study, cytoplasmic expression of DJ1 was particularly increased in post-treatment samples at stage IV. It seems that DJ1-mediated antioxidative defense is especially activated after chemotherapy in advanced-stage ovarian cancer.
The NRF2–KEAP1 system has previously been associated with platinum resistance in ovarian cancer. However, there are no data on the regulation of NRF2–KEAP1 proteins in neoadjuvant study designs. In our study, the increase in nuclear expression of KEAP1 after chemotherapy suggests a role of KEAP1 as an eliminator of nuclear NRF2 as a response to cytotoxic therapy.
Negative pre-treatment CD44 expression and positive ALDH1 expression could be novel potential indicators of the response to platinum-based chemotherapy in ovarian cancer. In our data, 100% of the tumors with this expression pattern were platinum-resistant. CD44 might also be of value in assessment of the development of chemoresistance in cases of persistent ovarian cancer. Further studies are needed to evaluate the expression of CD44 and ALDH1 in neoadjuvant-treated ovarian cancer.
Footnotes
This article is freely accessible online.
Conflicts of Interest
The Authors state that no conflicts of interest exist in regard to this study.
- Received April 13, 2016.
- Revision received May 28, 2016.
- Accepted May 31, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}