


Abstract
Background/Aim: For advanced paranasal sinus cancer, intra-arterial (I-A) chemotherapy has been applied for improving prognosis and organ preservation. While computed tomographic angiography (CTA) is useful for identifying the tumor-feeding artery, CTA cannot always detect the precise artery. The aim of this study was to assess the feasibility of endoscopic ICG (indocyanine green) fluorescence technique during I-A chemotherapy for recurrent skull-base cancer. Patients and Methods: Seven patients with recurrent skull-base cancer were included in this study. Conventional CTA followed by ICG was administered. Additional information regarding tumor-feeding arteries attained via ICG was evaluated. Results: Out of seven cases, the blood supply to the cancer was detected in three by CTA alone. By adding the endoscopic evaluation, the blood supply to the tumor was confirmed without difficulty in all cases. The information from endoscopic fluorescence imaging was helpful in making decisions concerning the administration of drugs for skull-base cancer. Conclusion: Endoscopic ICG fluorescence imaging combined with I-A chemotherapy compensated for deficiencies of CTA and generated more useful information about the feeders to tumors than was previously available.
- Skull-base cancer
- endoscopic ICG fluorescence imaging
- superselective intra-arterial chemotherapy
- CT angiography
For skull-base cancer such as advanced paranasal sinus cancer, which is resistant to conventional systemic chemotherapy, superselective intra-arterial (I-A) chemotherapy is effective because it increases the concentration of anticancer drugs in the tumor (1-5). To obtain precise information on the blood supply to tumors, we conducted computed tomographic angiography (CTA) for head and neck cancer in 1998 for the first time in the world (6). This procedure can provide accurate and detailed information about the vascular supply to head and neck tumors (7-10). However, it is difficult to confirm the drug distribution areas when the tumor is superficially spread or the patient has undergone dental treatment with metal.
Recent advances in indocyanine green (ICG) fluorescence imaging have enabled visualization of the blood flow in tissues (3, 11-14). In addition, a report using ICG fluorescence technique with I-A chemotherapy has been applied to oral cancer (15).
However, for conducting I-A chemotherapy for skull-base cancer, previously employed ICG techniques such as photodynamic eye (PDE; Hamamatsu Photonics Co. Ltd) use equipment too large to insert into the nasal cavity to obtain useful information concerning feeding arteries. As recent endoscopic ICG fluorescence imaging has enabled the visualization of the blood supply to intra-abdominal organs (15), we applied endoscopic ICG fluorescence technique for the visualization of the blood supply to skull-base tumors. The purpose of this study was to assess the feasibility of the endoscopic ICG fluorescence technique during I-A chemotherapy for recurrent skull-base cancer, especially paranasal sinus cancer.
Patients and Methods
Seven patients with recurrent skull-base cancer who were treated by I-A chemotherapy from April 2014 to March 2016 were included in this study. The patients' characteristics are shown in Table I. CTA was performed after the branch of a possible tumor feeding artery was identified using conventional digital subtraction angiography (DSA). At the same time, 5 mg of ICG was injected and we observed whether the tumoral regions were stained by means of near infrared (NIR) endoscopic camera system (NIR light; KARL STORZ Co. KG, Tuttlingen, Germany). The imaging is generated by a high-end full high-definition camera system (IMAGE 1 SPIES™; KARL STORZ Co. KG) connected to an endoscope with 5.8 mm diameter equipped with a specific filter for optimal detection of the NIR fluorescence and white light. A powerful xenon light source (D-LIGHT P SCB; KARL STORZ Co. KG) provides both visible and NIR excitation light. Switching from the standard light is controlled by the surgeon. In addition, NIR fluorescence imaging offers adjustable visualization modalities such as ICG mode and SPECTRA A mode. Surgeons can select NIR modes according to their specific situation and objective.
Patients' characteristics (TNM classification).

Indocyanine green (ICG) fluorescence endoscope (a) and ICG fluorescence images of skull-base cancer (b). i: White light, ii: ICG mode, iii: SPECTRA A mode. Endoscopic ICG fluorescence images were effective for detection of blood supply to skull-base tumors.
I-A chemotherapy was performed weekly over a 4-week period: 150 mg/m2 of cisplatin was administered superselectively through feeding arteries at 5 mg/min. Sodium thiosulfate at a dose of 200-fold that of cisplatin was injected intravenously concurrently to neutralize the adverse effects of cisplatin.
Patients also received concomitant cetuximab with I-A chemotherapy. An initial loading cetuximab dose of 400 mg/m2 was delivered intravenously over 120 min. Patients then received weekly infusions of 250 mg/m2 of cetuximab with I-A chemotherapy.
We evaluated the diagnostic sensitivity of CTA and endoscopic ICG fluorescence technique. Furthermore, we evaluated which mode was more effective for visualization and confirmation of blood supply, ICG mode or SPECTRA A mode. A SPECTRA A mode image is created by removing the red color from ICG fluorescence imaging. Figure 1 shows ICG fluorescence endoscopic and ICG fluorescence images of skull-base cancer which was biopsied 5 min after ICG injection. Informed consent was obtained from each patient before treatment and the study was approved by the Human Ethics Review Committee of our hospitals (approval number 00861).
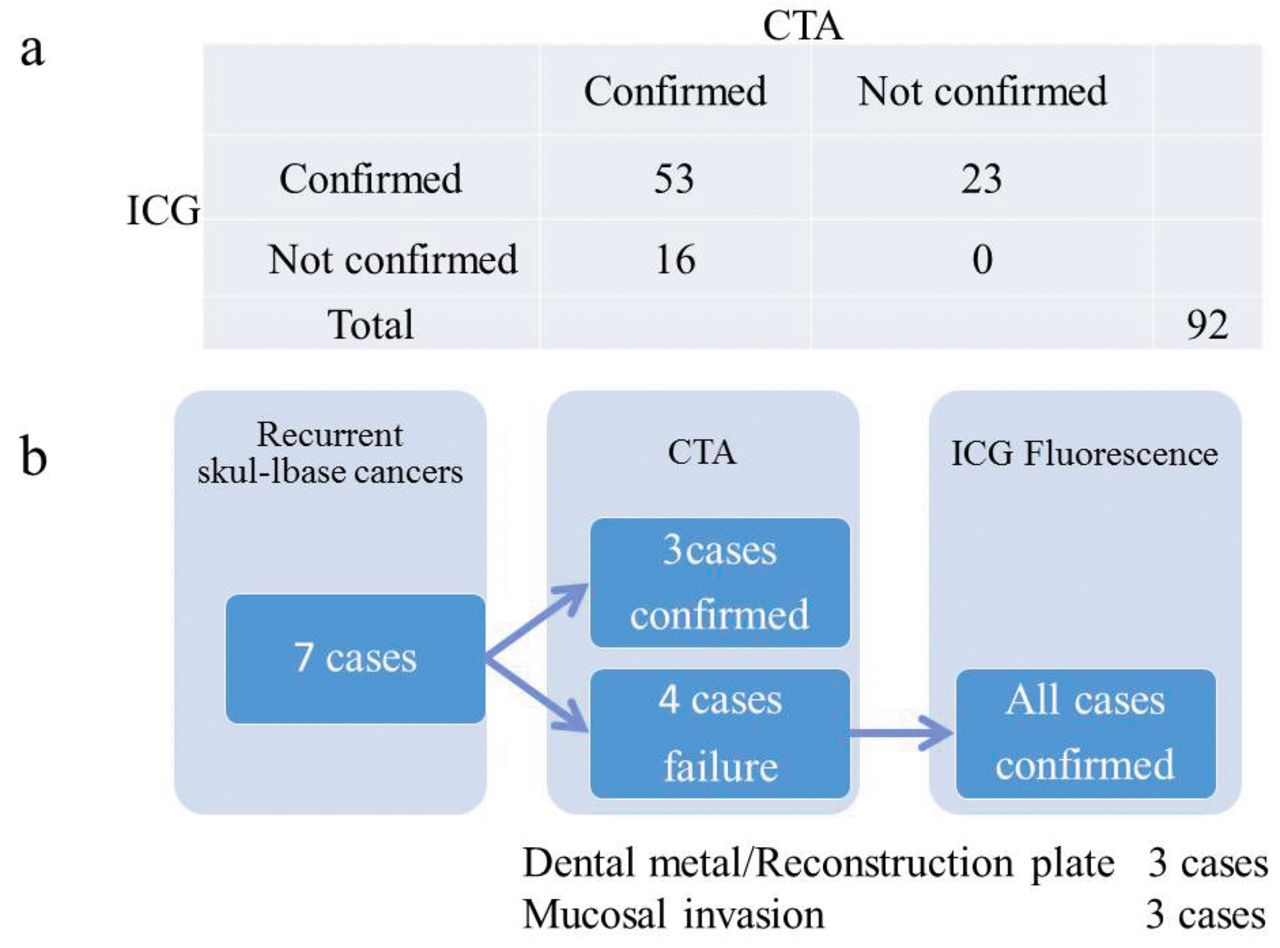
Confirmation rate of tumor-feeding arteries using computed tomographic angiography (CTA) and indocyanine green (ICG) fluorescence imaging. a: The total number of superselectively infused arteries was 92. Of the 92 infused arteries, CTA detected 69 blood supplies to tumors. However, CTA was unable to confirm the remaining 23 as supplying arteries to the skull-base cancer. b: CTA revealed the vascular areas of selected arteries in only three cases. The reasons for the failure in detecting the tumor-feeding arteries included dental metal or reconstruction plates (three cases) and mucosal invasions (three cases).
Results
Seven patients with recurrent skull-base cancer received I-A chemotherapy in order to preserve organs. Superselective I-A chemotherapy was carried out via the femoral artery. There were no significant complications. The total number of I-A chemotherapy courses was 31. The mean number of I-A chemotherapy courses was 4.5 (range=4-6).
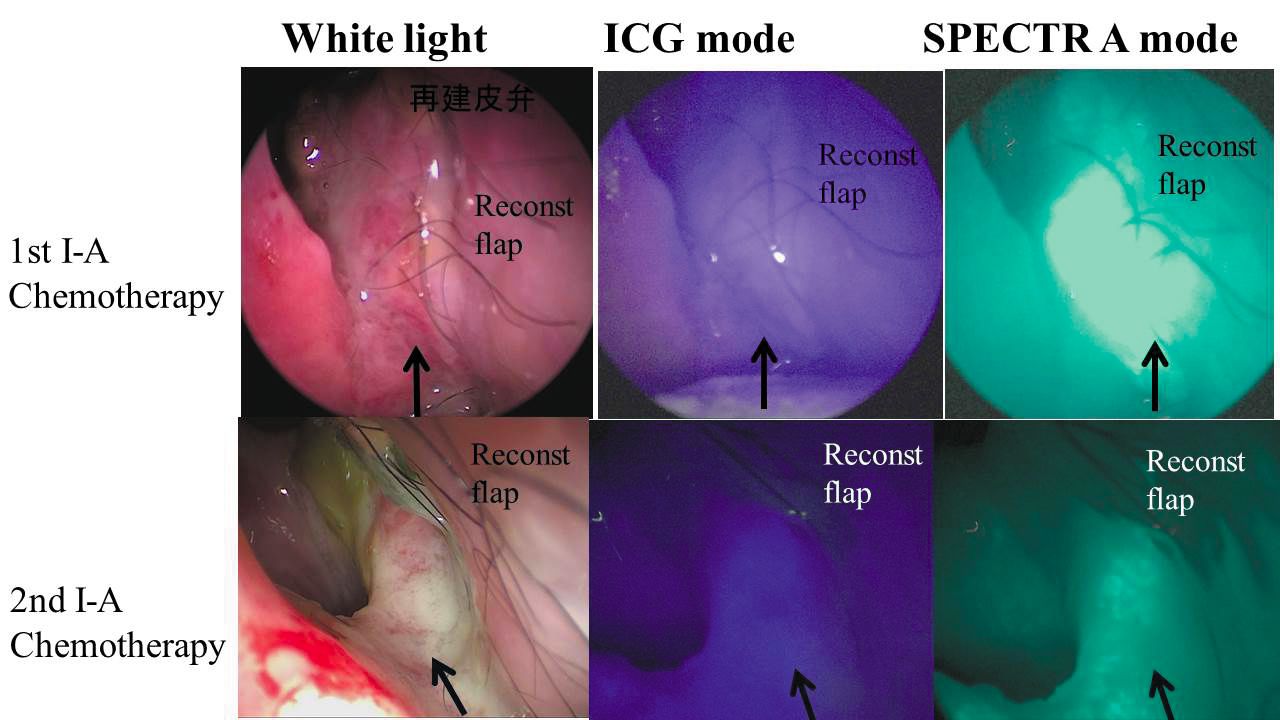
Relationship between the effect of chemotherapy and indocyanine green (ICG) fluorescence imaging. A recurrent paranasal carcinoma reconstructed with rectus abdominal flap occurred at the skull-base. The upper row shows the recurrent tumor displayed with white light, ICG mode and SPECTRA A mode in the first intra-arterial (I-A) chemotherapy. The lower row shows the recurrent tumor displayed with white light, ICG mode and SPECTRA A mode in the second I-A chemotherapy. ICG fluorescence as the second I-A chemotherapy was less than that of the first I-A chemotherapy. The targeted cancer was damaged by the first I-A chemotherapy and the blood supply to the tumor decreased. Arrows indicate the targeted cancer.

A case of carcinoma of the external auditory canal. Lateral (a) and frontal (b) view of the occipital artery shows the feeding artery to the targeted cancer (arrow). c: Computed tomographic angiography infused to the occipital artery. It was difficult to confirm the vascular region due to obstacle enhancement.
Table II shows a list of the infused arteries. The total number of superselectively infused arteries was 92. Recurrent cancer occurred at reconstructive flaps whose pedicles were anastomosed mainly to superior thyroid artery or facial artery. Of the 92 infused arteries, CTA detected 69 arteries supplying tumors. However, CTA was unable to confirm the remaining 23 infused arteries as feeders to skull-base cancer (Figure 2a).
CTA revealed the vascular regions of selected arteries in only three cases (43%). The reason for the failure in detecting the tumor-feeding arteries included the presence of dental metal or reconstruction plates (three cases) and superficial mucosal spread (three cases) (Figure 2b).
ICG fluorescence SPECTRA A mode for I-A chemotherapy revealed the blood supply to tumors more accurately than ICG fluorescence mode. The information obtained from endoscopic fluorescence imaging was valuable for making decisions concerning the administration of chemotherapy agents for skull-base cancer in cases involving dental metal, or mucosal invasion.

Indocyanine green (ICG) fluorescent imaging of carcinoma of the external auditory canal. a: Endoscopic view of carcinoma of the external auditory canal with white light and ICG fluorescent imaging infused through the occipital artery. Arrows show the targeted cancer. Endoscopic ICG fluorescent imaging clearly displayed the blood supply from the occipital artery. b: Computed tomographic angiography infused to the occipital artery. It was difficult to confirm the vascular region due to obstacle enhancement. c: ICG fluorescent imaging by photodynamic eye (PDE) with an otoscope. As the PDE was too large to insert in the external auditory canal involved by cancer, the PDE image was unable to clearly display the blood supply to the tumor.
Additionally, ICG fluorescence imaging revealed various states of the targeted tumor or their blood supply. Figure 3 shows that ICG fluorescence of the second I-A chemotherapy was less than that of the first I-A chemotherapy. This was a result of the targeted tumor being damaged by the first I-A chemotherapy and the consequent decrease in blood supply to the tumor.
In a case of carcinoma of the external auditory canal (T4bN0M0) suspected of being resistant to chemoradiotherapy and in which the patient suffered from facial palsy and trismus, we applied I-A chemotherapy four times. Figure 4 illustrates DSA lateral view and frontal view of the occipital artery supplying blood to the targeted cancer. We found that CTA infusing of the occipital artery did not clearly detect the vascular region due to enhancement of obstacles. An endoscope for ICG fluorescence imaging was inserted into the external auditory canal in order to observe the blood supply to the tumor in detail. We obtained an endoscopic view of the carcinoma of external auditory canal with white light and ICG fluorescent imaging infused through the occipital artery. The arrows in Figure 5a show the targeted cancer and highlight that endoscopic ICG fluorescent imaging clearly revealed blood supply from the occipital artery. However, CTA obtained in the selected occipital artery could not display the vascular area due to obstacle enhancement (Figure 5b). Previously employed PDE was too large to insert into the external auditory canal where the targeted cancer was deeply located. As a result, the PDE image did not clearly reveal the blood supply to the targeted cancer.

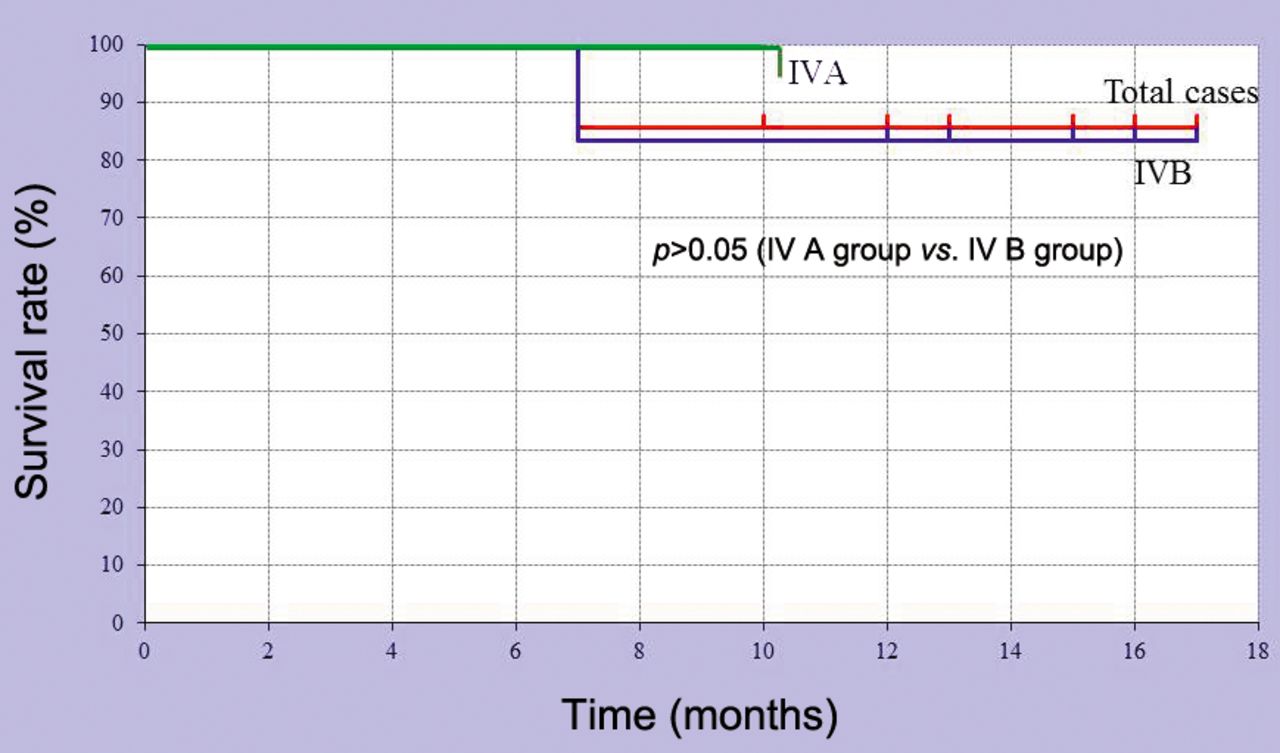
Overall survival rate according to therapy.
Summary of infused arteries.
The effect of I-A chemotherapy was that complete remission and partial remission were 4/7 (57%) and 3/7 (43%), respectively.
The overall survival rates after treatment of all cases, and of the IVA and IVB tumor groups were 87.5%, 100% and 85.5%, respectively (Figure 6). The difference between the overall survival rate of the IVA group and that of the IVB group was not significant according to the generalized Wilcoxon test.
Five patients were administered morphine due to severe pain prior to I-A chemotherapy. Following treatment, none of the patients required morphine for pain relief and all were able to consume food orally.
It cost $5 to purchase ICG (20 mg) for the application of endoscopic ICG fluorescence imaging. It took a mean of 7.5 minutes (range=6-11) to conduct the application of endoscopic ICG fluorescence imaging.
Discussion
Chemoradiotherapy for head and neck cancer plays an important role in organ preservation, however, there are many cases, such as paranasal cancer, for which conventional systemic chemotherapies are ineffective. Cisplatin is the most promising drug for therapy of head and neck cancer. When high doses of cisplatin are administered, various adverse effects can be observed, such as gastrointestinal toxicity, renal toxicity and hematological toxicity. For chemoresistant cancer, including paranasal sinus cancer, superselective I-A chemotherapy is considered to increase the concentration of the anticancer drug in cancer tissue, exerting powerful effects on chemoresistant tumors (1-5). This procedure is reportedly capable of achieving a positive prognosis as well as good organ preservation.
To achieve an effective therapeutic result for recurrent skull-base cancer with I-A chemotherapy, precise evaluation of the tumor-feeding artery and drug distribution is required (6). However, DSA cannot always clearly detect the border between the normal mucosa and surface-invasive tumor. CTA clearly displays the border between normal structure and deeply invasive cancer mass by using 3-dimensional sections. Therefore, CTA in addition to DSA provides more precise identification of the blood supply to the tumor (1, 6, 7). However, it is at times not possible to confirm the tumor-feeding artery in patients with paranasal sinus cancer who have dental metal or reconstruction plates, or surface invasion (17). Furthermore, repeated CTA increases X-ray exposure, which is a significant problem not only for patients but also for medical staff.
Recently, the ICG fluorescence technique was developed and has been used in various fields (3, 11-14). The excitation and emission profiles for ICG lie in the NIR wavelengths, which allow penetration and imaging of vessels below a few millimeters of tissue (11). It provides visualization of the blood supply to reconstructed organs, and sentinel lymph nodes in cancer surgery, including head and neck cancer (3, 12, 14, 18). ICG fluorescence has been used for navigation surgery and intraoperative detection of cancer (11, 19, 20).
We have previously reported that the ICG fluorescence technique can be a very useful method for treating oral or paranasal cancer with I-A chemotherapy in patients with dental metal (15, 17). However, previously employed ICG fluorescence cameras such as PDE are too large to insert within the pharynx or nasal cavity in order to observe tumor-feeding arteries of tumors there. As a result, we were unable to obtain precise information concerning blood supply to tumors located behind the oral or nasal cavity. As recent endoscopic ICG fluorescence imaging has enabled the visualization of the blood supply to intra-abdominal organs (20), we applied endoscopic ICG fluorescence technique for the visualization of the blood supply to skull-base cancer at I-A chemotherapy. In order to observe the blood supply to the skull base, we inserted the ICG fluorescence endoscope in the nasal cavity for all patients. However, the 5.8 mm diameter of the ICG endoscope is a little larger than the flexible endoscope typically employed. Consequently, some patients complained of experiencing slight pain on the insertion of the ICG endoscope.
The nearer the ICG fluorescence endoscope was inserted to the recurrent tumor, the higher excitation of ICG and the deeper penetration of the tissue was obtained up to10 mm. We were able to confirm whether the whole tumor had been successfully covered and filled with the anticancer drug in all cases. As a result, we were able to conduct superselective I-A chemotherapy effectively and safely for recurrent skull-base cancer with critical nerves or organs associated with dysphagia, or visual disturbance. A finer and more sensitive endoscope for ICG fluorescence imaging is required for the detection of blood supply to cancer of the skull base.
We found that the endoscopic ICG fluorescence technique was a very useful method even in patients with recurrent skull-base cancer who had undergone reconstruction using reconstruction plate. For tumors with multiple feeding arteries, ICG fluorescence in superselectively infused arteries was evaluated clearly and lucidly. As ICG fluorescent imaging continues to produce fluorescence for more than 10 min, it is necessary to be aware of the former fluorescent areas prior to ICG infusion to the additional feeding arteries to the skull-base cancer.
However, tumors invading at a depth greater than 10 mm require another imaging method, such as simultaneous CTA. Once the stained field of each feeding artery has been detected by CTA in the case of tumors invading the base of the skull or face, the endoscopic ICG fluorescence technique can then be used to compensate for deficiencies in CT angiography by identifying the feeding artery precisely and safely. As it is difficult to insert the 5.8 mm diameter of the ICG endoscope within the nasal cavity without pain, we inserted 0.1% epinephrine and 4% lidocaine gauze into the nasal cavity prior to the treatment.
It should be noted that a fine and sensitive endoscope for ICG fluorescence imaging is required for the detection of skull-base cancer. This technique is feasible and also achieves new promising options for skull-base or paranasal sinus cancer. Further investigations may lead to development of a new minimally invasive multimodal therapy targeting advanced skull-base cancer in the future.
Conclusion
The application of endoscopic ICG fluorescence imaging together with CTA provides more accurate information in relation to the feeding arteries to skull-base cancer and enables effective I-A chemotherapy without complications.
Acknowledgements
This study was supported by Grants-in Aid for Scientific Research from the Ministry of Education, Culture, Sports, and Technology (22591920) of Japan.
Footnotes
This article is freely accessible online.
Conflicts of Interest
The Authors declare that they have no competing interests.
- Received May 2, 2016.
- Revision received June 3, 2016.
- Accepted June 7, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.