


Abstract
Background: There has recently been renewed interest in the use of estrogens as a treatment strategy for castration-resistant prostate cancer (CRPC). The purpose of this study was to evaluate the feasibility and efficacy of ethinylestradiol re-challenge (re-EE) in the management of CRPC. Patients and Methods: Patients with metastatic CRPC who received re-EE after disease progression on prior EE and other therapy were retrospectively reviewed for prostate-specific antigen (PSA) response, PSA progression-free survival (P-PFS) and adverse events. Results: Thirty-six re-EE treatments were performed for 20 patients. PSA response to the initial EE treatment was observed in 14 (70%) patients. PSA response to re-EE was 33.3% in 36 re-EE treatments. The median P-PFS for patients treated with initial and re-EE was 7 months and 4 months, respectively. Interestingly, PSA response to re-EE was observed even in non-responders to initial EE, and those treated with multiple re-EE. No patients developed cardiovascular or thromboembolic events. Conclusion: Re-EE may be safely repeated several times and can lead to a prolonged disease control in selected patients. Re-challenge with EE appears to be a reasonable option worth considering for patients with metastatic CRPC.
The standard initial systemic therapy for advanced prostate cancer is androgen-deprivation therapy. Even patients with metastatic prostate cancer initially respond well to hormone therapy, but then progress to castration-resistant prostate cancer (CRPC), which is accompanied by a high mortality rate (1).
Treatment options for CRPC include palliative chemotherapy, such as docetaxel or cabazitaxel, but also corticosteroids, estrogens, sipuleucel T and, more recently, CYP17 inhibitor (abirateron acetate) and androgen receptor antagonist (enzaltamide) (2-7). Treatment with estrogens was used as a palliative therapy for advanced prostate cancer, however, the discovery of luteinizing hormone-releasing hormone (LH-RH) agonists led them to become less common and they stopped being used in most countries in the 1980s (8). One of the reasons for reduction in their use is the risk of cardiovascular and thromboembolic events during therapy. However, several reports demonstrated the positive oncological results of therapy with estrogens, such as diethylstilbestrol (DES) and ethinylestradiol (EE) for CRPC, and there has recently been renewed interest in their use as a treatment strategy (9-12). European Association of Urology 2013 guidelines concluded that DES can be an effective form of estrogen therapy; however, there is still concern regarding significant adverse events, such as cardiovascular and thromboembolic events (2).
There is currently no standard treatment option for patients with relapsed CRPC. We aimed to determine if re-challenge with EE has oncological benefits for patients whose disease had progressed on initial EE and to identify candidate predictors of benefit and resistance.
Patients and Methods
A retrospective review was conducted in 20 consecutive patients with metastatic CRPC who were re-challenged with EE after progressing on prior EE and other treatments for metastatic CRPC from April 2012 to October 2015. After progression on androgen-deprivation therapy, initial EE treatment (oral administration of 1.5 mg EE daily with 100 mg of aspirin) with LH-RH agonist was administered. Disease in all patients in our cohort had progressed on initial EE treatment with LH-RH analogs and they were resubmitted to EE with LH-RH agonist after several lines of another treatment for metastatic CRPC (such as corticosteroids, docetaxel, abirateron acetate, enzaltamide etc.). Re-challenge with EE was repeated unless contraindicated (e.g. an inadequate performance status, new comorbidities) or patients had experienced unacceptable toxicities. Twenty patients underwent 36 re-challenges with EE. LH-RH agonist was continued during the overall treatment period for all patients. Patients with severe or uncontrolled cardiovascular disease and concomitant other advanced malignancies were excluded.
Patients' characteristics (n=20).
Patients were followed-up at our hospital every 4 weeks. Prostate-specific antigen (PSA) was serially measured every 4 weeks during re-challenge EE treatment. Written-informed consent was obtained from all of the included patients, and the review of patient data was undertaken with Institutional Review Board approval for chart review at our hospital.
We evaluated the patients' clinical outcomes [PSA response rates, PSA-progression free survival (P-PFS) and adverse events]. According to the PSA Working Group Criteria, a PSA response was defined as a 50% greater decrease in serum PSA confirmed by two separate measurements at least 4 weeks apart. PSA progression was defined as an increase of at least 50% above the nadir, with an absolute increase of 5 ng/ml, or a PSA increase over 25% from the nadir or from baseline for those not meeting the PSA decline criteria (2). After progression on re-challenge with EE, patients were treated with various other treatments for metastatic CRPC at their physician's discretion.
Fisher's exact tests and Mann-Whitney U-tests were used for evaluating the relationship between clinical factors and the PSA response. Median time for PSA progression was calculated with the Kaplan-Meier method. The statistical analysis was undertaken using SAS software, version 8.2 (SAS Institute, Cary, NC, USA) and a value of p<0.05 was considered to be statistically significant.
Main findings of re-challenge with ethinylestradiol (EE) (n=36).
Results
Clinical characteristics of the patients in this study are shown in Table I. The median age at diagnosis was 75 (range 68-88) years, median initial PSA was 178 (range 74.7-7641) ng/ml, and median time to CRPC was 11 (range 3-77) months. PSA response to the initial EE treatment was observed in 14 (70%) out of 20 patients.
Ten patients underwent one re-challenge, three underwent two, four underwent three, and two underwent four.
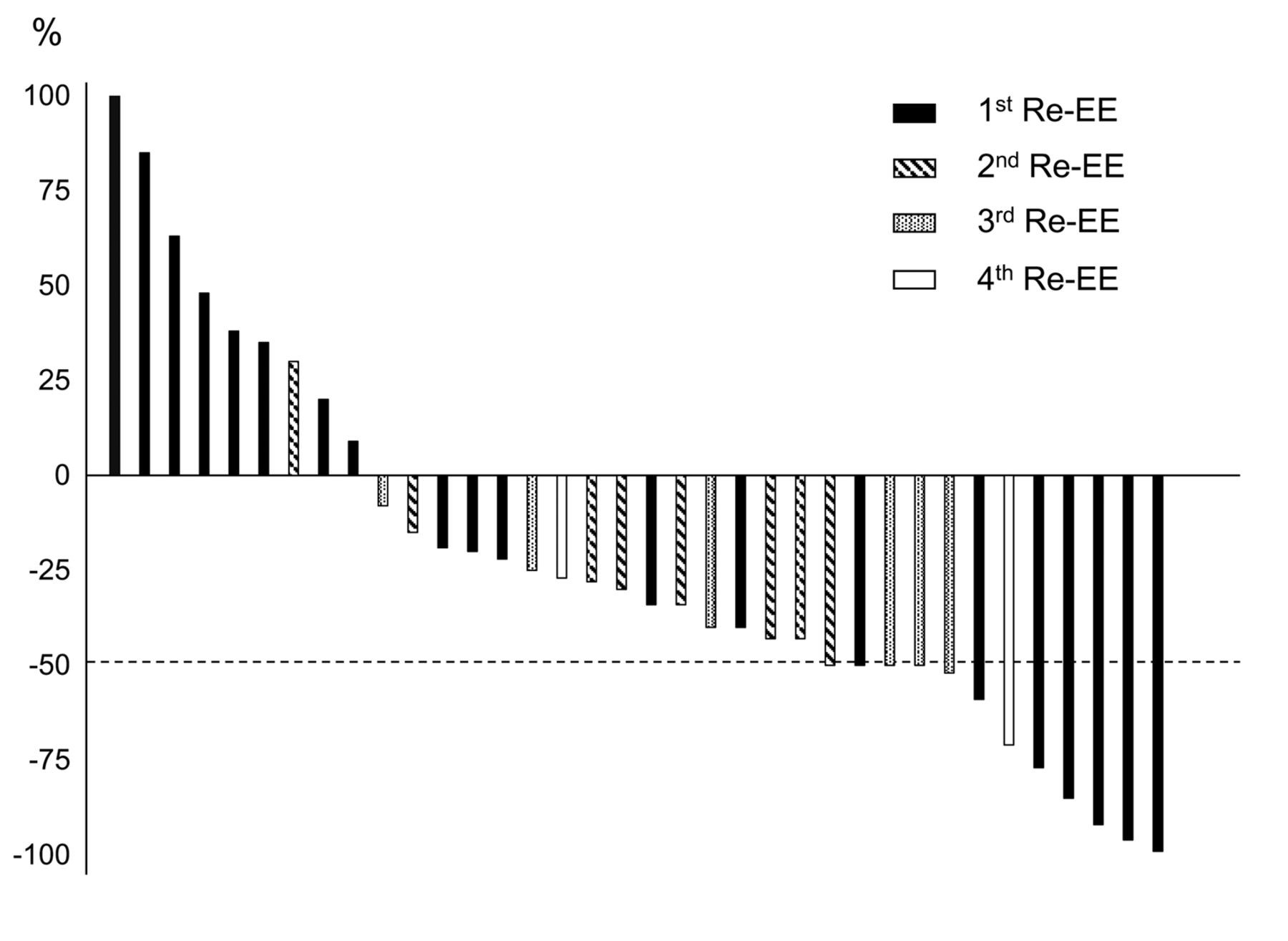
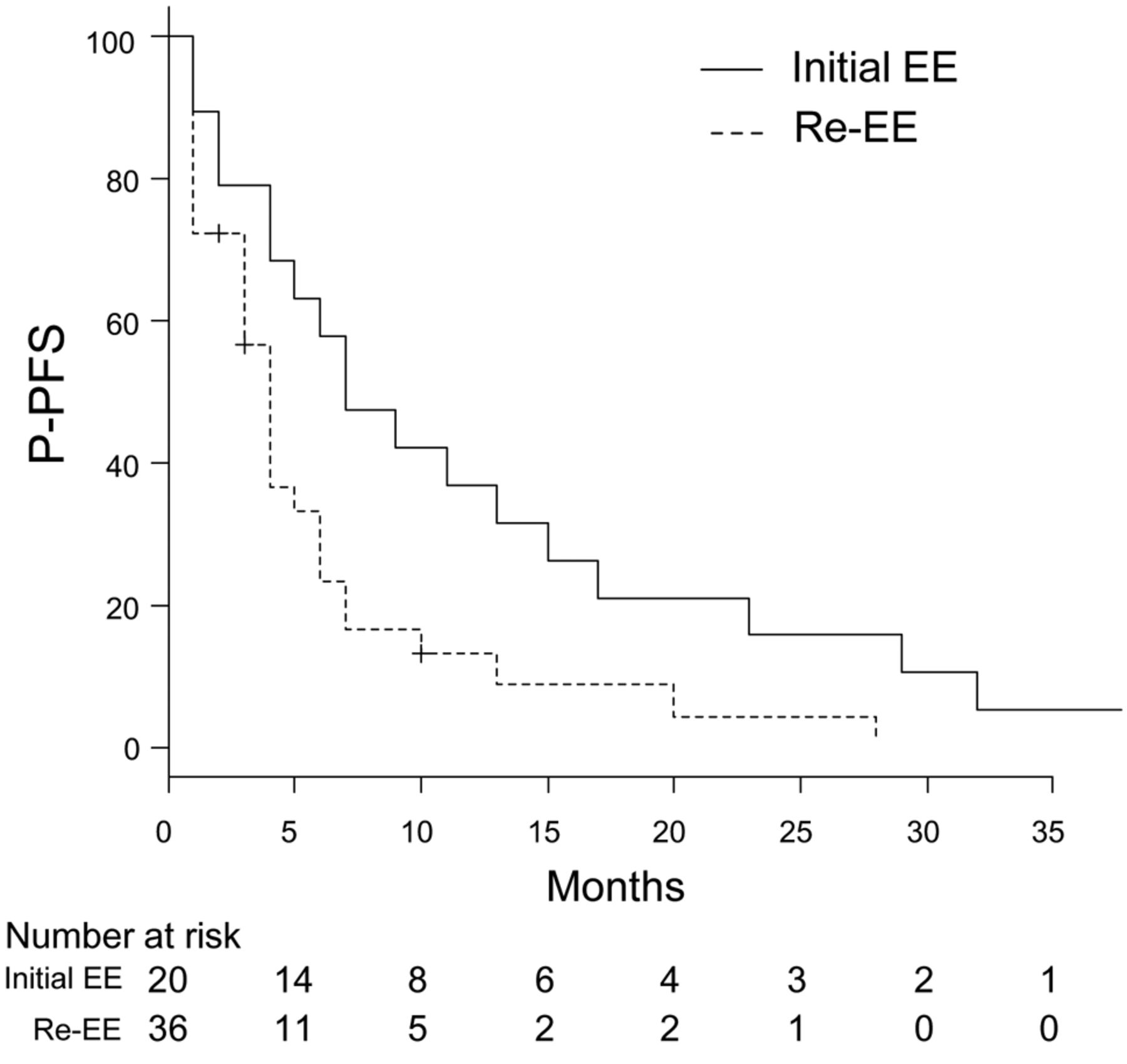
The main findings of 36 re-challenges with EE are shown in Table II. Median PSA at the start of re-EE was 49 (range 2.5-2,200) ng/ml. The best PSA response for each EE re-challenge is displayed as a waterfall plot in Figure 1. Notably, five out of 12 PSA responders had a PSA response with multiple re-challenges with EE (second: n=1, third: n=3, and fourth: n=1), two out of 12 did not have a PSA response to their initial EE treatment. Although we evaluated the clinical factors predicting PSA response in re-challenge with EE, no predictive factors had significant correlation with response to re-challenge (data not shown). Kaplan-Meier curves for P-PFS for both initial and re-challenge with EE are shown in Figure 2. The median P-PFS with initial EE treatment in this cohort was 7 months [95% confidence interval (CI)=4-15 months] compared with 4 months (95% CI=3-5 months) for re-challenge with EE. Only five out of 36 re-challenges with EE had longer P-PFS compared with initial EE treatment (Figure 3). These data suggest that, although re-challenge with EE has some efficacy, overall it appears to be less than that seen with initial treatment; PSA response was less frequent (p=0.01) and P-PFS shorter (p=0.015). After a median follow-up of 18 (range=3-42) months from the start of first re-challenge with EE, 13 patients were still alive and seven had died.

The best prostate-specific antigen (PSA) response for 36 ethinylestradiol re-challenges is displayed as a waterfall plot. 1st, 2nd, 3rd, and 4th Re-EE represent the first, second, third, and fourth re-challenge with ethinylestradiol, respectively.
Appetite loss (grade 1) was seen in two patients. No severe adverse events such as cardiovascular and thromboembolic events were observed during the period of re-challenge with EE (median=4 months, range=1-28 months). Only one patient with fatigue (grade 2) during re-challenge with EE required treatment cessation.
Discussion
The oral administration of EE was associated with a high PSA response rate (approximately 70%), and a relatively long median time to progression (10-15 months) for metastatic CRPC (11, 12). In our cohort, the PSA response rate was 70% and median time to progression was 7 months at the initial EE treatment. In addition to the effect on CRPC, EE has the benefits of ease of medication and cost effectiveness.
This study demonstrates that patients with metastatic CRPC can demonstrate PSA response to re-challenge with EE after failure of prior EE treatment. Although the clinical effects observed were less than those under initial EE treatment, re-challenge may be a viable therapeutic strategy in a selected subset of patients who are able to receive further therapy. To our knowledge, this is the first study to evaluate the efficacy and safety of re-challenge of EE for patients with metastatic CRPC.
We found that PSA response (≥50% reduction) was seen in 33% and partial response (≥25% reduction) was observed in 61% of re-challenges. Interestingly, PSA response was observed even in patients with multiple re-challenges, non-responders to initial EE or prior re-challenge with EE, and patients post-docetaxel therapy. Thus, our results would suggest potential change in the biology of CRPC over time in response to various other treatments received.
Few reports about re-induction of hormone sensitivity in CRPC have been published. Shamash et al. reported on the re-induction of hormone sensitivity in patients with androgen-refractory prostate cancer following chemotherapy with lomustin and chlorambucil. In their study, endocrine therapy was stopped during chemotherapy. PSA response was observed in 8 out of 17 (47%) patients who were re-challenged with hormone therapy following chemotherapy failure (13). Cox et al. reported the cases of two patients who responded to re-challenge with DES after their disease progressed on chemotherapy (14). A prospective phase II study suggested that endocrine sensitivity can be reintroduced by stopping endocrine therapy during chemotherapy for patients with androgen-independent prostate cancer (15). Similarly to our study, Clemons et al. reported that DES led to PSA response in patients with CRPC whose disease previously progressed on DES but were re-challenged after a drug holiday. In their study, seven out of eight patients had a PSA response with a re-challenge of DES. Among the seven responders, three had not had a PSA response in their initial treatment period. Two patients had three separate DES treatments and experienced a PSA response during each treatment (16). Taken together with our findings, although both groups were too small to lead to firm conclusions, sensitivity to estrogens can be reintroduced after a drug holiday, and re-challenge with estrogens may be worth considering for patients with metastatic CRPC even after chemotherapy failure.

Kaplan–Meier curves comparing the prostate-specific antigen progression-free survival (P-PFS) in patients with initial ethinylestradiol (Initial EE) treatment and those with re-challenge of ethinylestradiol (Re-EE).
Several mechanisms of action have been proposed for the effect of estrogens on CRPC. Adrenal androgens are thought to continually stimulate the androgen receptor in patients with castration levels of testosterone, thereby fuelling disease progression. The administration of estrogen to patients with CRPC has been associated with a decrease in adrenal androgens (17, 18). Montgomery et al. reported that estradiol significantly suppressed tumor testosterone and dihydrotestosterone and inhibited growth of CRPC in an estrogen receptor-independent manner (19). DES has been shown to induce cell-cycle arrest at G2/M phase and apoptosis in hormone-insensitive prostate cancer cells (20). DES has also been shown to inhibit the cytochrome bc1 complex in the mitochondrial respiratory chain, thus disturbing cellular energy metabolism (21). Furthermore, estrogens have been demonstrated to inhibit tubulin polymerization, which is an integral component of the mitotic apparatus in prostate cancer (22), and directly to inhibit DNA synthesis and angiogenesis (23). Recently, DES was demonstrated to inhibit telomerase activity in both androgen-dependent (LNCaP) and -independent (PC3) prostate cancer cell lines (24). Thus several different possible mechanisms of action might affect the re-induction of EE sensitivity at different points along the course of metastatic CRPC.

Prostate-specific antigen progression-free survival (P-PFS) with initial ethinylestradiol treatment (Initial EE) compared with P-PFS with re-challenge of ethinylestradiol (Re-EE).
It is extremely difficult to treat metastatic CRPC and no consensus has been reached with regard to the management strategy, especially for relapsed metastatic CRPC. In general, docetaxel plus prednisolone is a standard treatment for metastatic CRPC, and best supportive care is usually selected after the chemotherapy failure in clinical practice. Re-challenge therapy for patients with CRPC whose disease had previously progressed on initial treatment has not yet been established in the treatment strategy. In patients with tumor progression after first-line docetaxel chemotherapy, docetaxel re-challenge has shown to retain antitumor activity (25, 26). The effect of abiraterone acetate re-challenge was recently demonstrated (27). Antitumor activity in patients with PSA response at first-line treatment was preserved at the re-challenge with both docetaxel and abiraterone (25-27). Furthermore, re-challenge with dexamethasone also led to PSA responses in our cohort (data not shown). Thus re-challenge with not only estrogens but also other treatments might be considered for treatment strategy for relapsed metastatic CRPC.
This study clearly has several limitations. The retrospective nature of this review and the small number of patients with short follow-up period introduces several biases. With a sample size of 36 re-EE treatments, the power of the study may have been too low to identify predictors of PSA response in re-challenge with EE. Imaging assessment of measurable disease was not routinely performed. Furthermore our cohort was Japanese, therefore the effect of re-EE and the adverse events, especially cardiovascular events, may be different between different races. In light of the multiple treatment options now available and with increased funding limitations, our findings of the efficacy of re-challenge with EE might provide an additional opportunity and clinically meaningful benefit in patients with CRPC with limited therapeutic options.
Conclusion
Currently, no consensus on treatment sequencing for CRPC exists, all approved treatments, including re-challenge of EE, are variable options. Randomized control trials looking at the effect of re-challenge with EE are warranted. To the best of our knowledge, this is the first report demonstrating the feasibility and activity of sequential multiple EE re-challenge in patients with relapsed metastatic CRPC.
Footnotes
Conflicts of Interest
The Authors declare that they have no conflicts of interest with regard to this study.
- Received March 16, 2016.
- Revision received April 18, 2016.
- Accepted April 20, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}