


Abstract
Background: Circulating tumor cells have been described in prostate cancer patients at diagnosis and in the metastatic phase but little is known on their role at biochemical PSA recurrence. Patients and Methods: Patients radically cured with either prostatectomy or radiotherapy were sequentially included at PSA recurrence. The presence of CTCs was evaluated by the CellSearch system. Results: Twenty-nine patients were accrued at PSA recurrence. Median PSA at recurrence was 7.2 ng/ml (range=3.86-51.0 ng/ml). The median time to PSA progression was 4.66 years (range=0.1-16 years). CTCs were detected in one patient (3%) with low numbers (1 CTC/7.5 ml). Conclusion: In patients radically cured for prostate cancer at biochemical recurrence, CTCs are detected at very low levels in a minority of patients. Further studies are required to investigate alternative methods of CTC detection and the possible role of the bone marrow pre-metastatic niche at biochemical recurrence.
Patients with clinically localized prostate cancer (PrCa) are treated with a definitive local treatment including either radical prostatectomy or external-beam radiotherapy (EBRT). However, approximately 30% of all radically cured PrCa patients develop a prostatic-specific antigen (PSA) progression within 10 years, without any other clinical evidence of disease. Following biochemical recurrence, the mean time to developing overt metastases is highly variable, but consistently long, being reported to be 8 years on average (1). There is however a subgroup of patients with biochemical progression with poor prognosis, therefore PSA progression does not reflect the biological heterogeneity of PrCa leading to the extremely different clinical outcome of patients at this disease stage. The PSA doubling time after radical prostatectomy or radiation therapy is a prognostic marker and may distinguish between local and distant recurrence but other more robust parameters are needed (2-4).
At PSA progression, a great proportion of patients is addressed to androgen deprivation therapy (ADT) although there is no demonstration of efficacy of ADT in this setting. Since prognosis is on average very good, these patients are destined to receive ADT for a long time period and are at risk of long-term morbidity, namely diabetes, metabolic syndrome, cardiovascular diseases that increases the mortality risk (5, 6). In this context, the search of new-generation PrCa biomarkers accounting for tumor aggressiveness and patient prognosis is of paramount importance in the clinical decision making process to prescribe ADT or not (7).
Circulating tumor cells (CTCs) are biomarkers that fulfill the requisites to be defined a “liquid biopsy”. CTCs are dynamic, real-time markers with proven predictive and prognostic value in different solid metastatic neoplasms including PrCa (8-12). Moreover, when added to clinicopathological models in metastatic PrCa, CTCs have proven superior to serum PSA in terms of patient prognosis and prediction of treatment efficacy (13-15).
The presence of disseminated tumor cells (DTCs) in the bone marrow of non-metastatic PrCa patients is an early event in the disease continuum and represents an independent predictor of PSA recurrence and survival (16-19). Homing and engagement of the BM pre-metastatic niche can represent a reservoir for PrCa cells and can direct their entry in the bloodstream and secondary dissemination as CTCs. Therefore, given the presence of DTCs in the BM of PrCa patients at diagnosis, it would be rationale to speculate an increase of CTCs at PSA progression. However, while several reports exist on CTCs at diagnosis (20-24) and at the macro-metastatic phase, their role at biochemical PSA progression has not been extensively investigated. We, therefore, designed a prospective cohort study aiming to investigate the prognostic role of CTCs levels in PrCa with biochemical relapse.
Patients and Methods
Study design and patient selection. This was a prospective, single-center study conducted at the Spedali Civili, University of Brescia, Italy. The Institutional Review Board at the Spedali Civili of Brescia approved the study as part of a wider project of genotype characterization in liquid biopsies for the early identification of lethal disease in prostate cancer patients with PSA progression after primary treatment. All patients provided a written informed consent for diagnostic and research procedures. The study was conducted in accordance to the ethical principles for medical research involving human subjects of the Helsinki Declaration. This study was sponsored by a grant from the Fondazione Comunità Bresciana Onlus. The sponsor had no role in conducting the trial and in manuscript preparation.
Patients sequentially observed at the Departments of Urology, Radiation Oncology and Medical Oncology were eligible with the following inclusion criteria: histology-proven diagnosis of prostatic adenocarcinoma, Gleason score ≥6, biochemical (PSA) progression after radical prostatectomy or EBRT with curative intent and documented by two consecutive PSA determinations. Patients with metastatic disease, previous or concomitant neoplasms, previous hormonal treatment or serious comorbidities were excluded. Previous hormonal treatment was permitted if interrupted more than 12 months before enrollment. At PSA progression, staging procedures included total body computed tomography and either a Technetium-99 scintigraphy bone scan or a choline positron-emission tomography (Cho-PET). All patients were evaluated for performance status according to the ECOG scale and for the presence of local symptoms according to the International Prostate Symptom Score (IPSS) of the American Urological Association (25).
PSA recurrence was defined according to the criteria of the Radiation Therapy Oncology Group-American Society of Therapeutic Radiation and Oncology (RTOG-ASTRO-Phoenix consensus): PSA rise of ≥0.2 ng/ml for prior prostatectomy or >2 ng/ml rise for post-nadir in prior EBRT (26).
CTC analysis. CTCs analysis was performed using the CellSearch technology (CellSearch-TM, Janssen, Raritan, NJ, USA). Peripheral blood samples were drawn at baseline into 10 ml evacuated tubes which contained a cell preservative (CellSave Preservative Tubes, Veridex LLC, Raritan, NJ, USA), maintained at room temperature and processed within 96 h from collection. The cell detection system consists of a sample preparation and a cell analysis platform that have been described in details elsewhere (27). Briefly, ferrofluids coated with anti-EpCAM antibodies were used to immuno-magnetically enrich epithelial cells from 7.5 ml of blood. The enriched samples were stained with phycoerythrin (PE)-conjugated antibodies directed against cytokeratins 8, 18, 19, an allophycocyanin (APC)-conjugated antibody to CD45 and the nuclear dye DAPI. The isolated and stained CTCs were transferred to a MagNest cartridge and analysed on the CellTracks Analyser II, a four colours semi-automated fluorescence microscope. Automatically selected images were reviewed by a trained operator for identification and counting of CTCs, which were defined as cytokeratin-positive and DAPI positive nucleated cells lacking CD45 staining. Quality controls were included for each determination. Results are reported as number of CTCs/7.5 ml of whole blood.
Patients' characteristics.
Statistical considerations. This study is part of a wider project on the lethal phenotype in PCa. We hypothesized that because CTCs are described in approximately 10% of patients at diagnosis (22, 23) and resident BM-DTCs can further contribute to blood spreading, a higher proportion of CTCs could be detected in patients at PSA progression. Therefore, we established a null hypothesis (no difference) and an alternative hypothesis (CTCs in 40% of patients) and calculated a sample size of 31 patients to detect a difference of 30% with an alpha error of 5% and a power of 80%. For the purposes of this study descriptive statistics was used to describe results. The SPSS software package (version 17.0) was used for statistical analysis.
Comparison of CTC studies by the CellSearch system in patients with rising PSA and no evidence of disease.
Comparison of CTC studies by the CellSearch system in patients with prostate cancer in different clinical settings.
Results
Patients' characteristics. From May to September 2014, 31 consecutive patients were accrued in the study and 29 were eligible for final analysis. Table I summarizes patients characteristics. Briefly, all patients had previously undergone radical prostatectomy and two (7%) of them had received adjuvant radiotherapy because of stage (pT3), extracapsular disease and microscopic involvement of surgical margins (R1). At initial diagnosis the median age was 70 years (range 53-72 years), the median Gleason score was 7 (range=6-9) and the median PSA value was 7.4 ng/ml (range=3.86-51.0 ng/ml). Thirteen (45%) patients had previously received hormonal treatment (after surgery) and 16 (55%) were hormone treatment-naïve. The median time from prostate cancer diagnosis to PSA progression was 4.5 years (range=0.1-16 years). At enrollment, the vast majority (97%) of patients had a good (ECOG 0) performance status and the median PSA value was 0.82 ng/ml (range=0.2-4.0 ng/ml). The median PSA doubling time (PSADT) was 9 months (range=2.6-43.6 months). Restaging at PSA progression demonstrated no evidence of disease in 19 (65%) patients and local relapse in 10 (35%) patients, respectively. Three (10%) patients with local relapse after surgery alone were treated with radiotherapy on the prostatic bed and started hormonal treatment thereafter. Patients without evidence of local or distant recurrence did not receive any treatment. At 6 months the median PSA value was 0.49 ng/ml (range=0.01-3.75 ng/ml) and after a median follow-up of 12 months 28 patients are alive and progression-free. At 6 months from enrollment, one patient developed bilateral lung metastases and started hormonal therapy.
CTC analysis and correlation with PSA levels and metastatic patterns. Twenty-nine patients were eligible for CTCs analysis at PSA recurrence. Only one patient out of 29 (3%) showed one single CTs/7.5 ml. This patient was a 59-year-old man with a pT2cN0 prostate cancer and Gleason score 6 at diagnosis. In February 2007, he underwent radical prostatectomy with negative margins followed by adjuvant hormonal therapy with bicalutamide 150 mg daily for 4 years. After a time-to-PSA progression of 36 months, PSA started rising in January 2010. The patient was enrolled after more than 12 months of hormonal treatment wash-out. After enrollment the patient remained metastasis-free with a fluctuating PSA at 3 and 6 months and is clinically monitored. Notably, no CTCs have been detected in the patient with lung metastases. No correlation was made between the presence of CTCs and clinico-pathological characteristics.
Discussion
The setting of PSA recurrence represents a “grey zone” in the clinical management of PrCa patients. While, on one hand, the majority of patients will have and indolent course and will develop overt metastases after a median time of 8 years, a small fraction will display an aggressive disease with rising PSA, early macrometastatic pattern at multiple levels and rapid onset of hormone-independent growth. Differently from the first group, the second one is destined to have dismal prognosis. Therefore, it is mandatory to identify early this so-called “lethal phenotype” in order to limit prescription of ADT to this patient setting and avoid useless hormonal treatments in the remaining patients.
CTCs are generally considered to better reflect the biological features of the neoplasm, which they are derived from, rather than its overall burden (28). The pre-specified hypothesis in this study was that biochemical progression of PSA in radically cured PrCa patients could be related to an increase of CTCs in blood and may, therefore, represent a potential early marker of aggressive disease. Surprisingly, in our study we observed that at PSA progression only one patient (3%) had one CTC, as detected by the CellSearch system. To the best of our knowledge, only two other studies by Aragon et al. (29) and by Lowes et al. (35) investigated the same setting of patients with this technology. Aragon reported similar results with 3 patients having a median of 1 CTC/7.5 ml (Table II). However, two of these patients were finally diagnosed with bone metastases limiting to only one (3%) patient the setting of “pure” biochemical recurrence. The authors suggested that the presence of CTCs at biochemical recurrence could serve as an early predictor of metastatic disease. However, in our study we did not detect CTCs in the single patient with lung metastases. In the Lowes's study a higher proportion (17%) of CTC patients was detected but the median number of CTCs/7.5 ml of blood was the same.
Despite the fact that these studies and ours include a limited number of patients (Table II), they are interesting to the fact that they all confirm that a biological difference exists between an active macroscopic disease (i.e. untreated local or metastatic PrCa) and a microscopic biochemical recurrence. The literature analysis reveals that CTCs are detected, albeit at different levels, both in localized disease and in the metastatic one but not at biochemical recurrence (Table III). Several explanations of this phenomenon can be tentatively identified.
First, CTCs are very rare events in the blood (in the order of 1/107-8 mononuclear cells/mcl), so 7.5 ml of blood may represent an insufficient sample to detect extremely low numbers of CTCs as at PSA recurrence. To overcome this problem with the CellSearch system either a larger sample volume of blood or a cellular enrichment step should be considered. In fact, in a study by the MD Anderson Cancer Center in patients with non-metastatic early PrCa, the authors reported that 21% of patients had at least one CTC but only 8% of patients had 3 or more CTCs when the analysis was performed in 22 ml of blood (31). In another study, Pal et al. used an enrichment-based separation step to identify a median of 3 CTC in 49% of patients with untreated localized PrCa (38).
Second, it is possible that at biochemical recurrence, cancer cells have undergone epithelial-to-mesenchymal transition (EMT) processes with down-regulation of the Epithelial Cell Adhesion Molecule (EpCAM) and may therefore become not detectable for the CellSearch system which is based on EpCAM expression for cancer cell capture and analysis (32, 38).
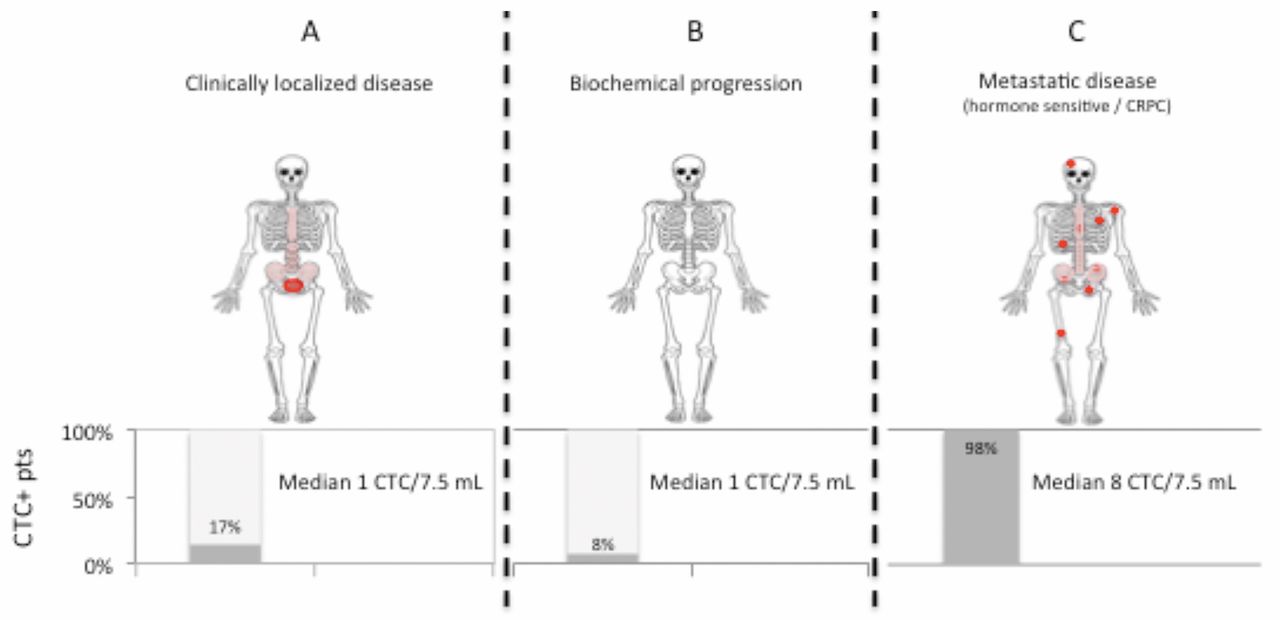
Third, several lines of research indicate that the bone marrow can function as a reservoir for cancer cells to form a “secondary” cancer site when the primary one has been surgically removed or irradiated. Within the bone marrow, cancer cells compete for the hematopoietic stem cell niche where they may remain in a dormant state or undergo apoptosis (17). Interaction with a variety of soluble factors such as cytokines and chemokines or BM-derived cells can regulate the transition from an inactive to an active state leading to detachment of DTCs and their entry in peripheral blood as CTCs which in turn may give rise to overt metastases (33). The functional state of BM-DTCs could, therefore, have a translational meaning with the presence of blood CTCs being the marker of an active versus inactive BM niche. In this view, the absence of higher numbers of CTCs at PSA recurrence, would indicate an inactive BM compartment (Figure 1).
To provide further background to support this hypothesis, we conducted a literature search on published papers on CellSearch-based CTC detection within the three main settings of PrCa natural history: untreated localized disease, biochemical relapse without evidence of disease and metastatic disease. The systematic analysis of results of individual studies offers a summary of published evidence of CTCs by the reference technology in each of the three settings (Table III). Overall more than 1,200 PrCa patients have been studied by the CellSearch platform to detect and enumerate CTCs in peripheral blood. CTCs are detected in 17%, 8% and 98% in the three clinical settings, respectively. Median CTC levels are low (1 CTC/7.5 ml) in patients with untreated localized disease and with biochemical relapse without evident disease while the highest number is observed in patients with metastatic disease (8 CTC/7.5 ml).
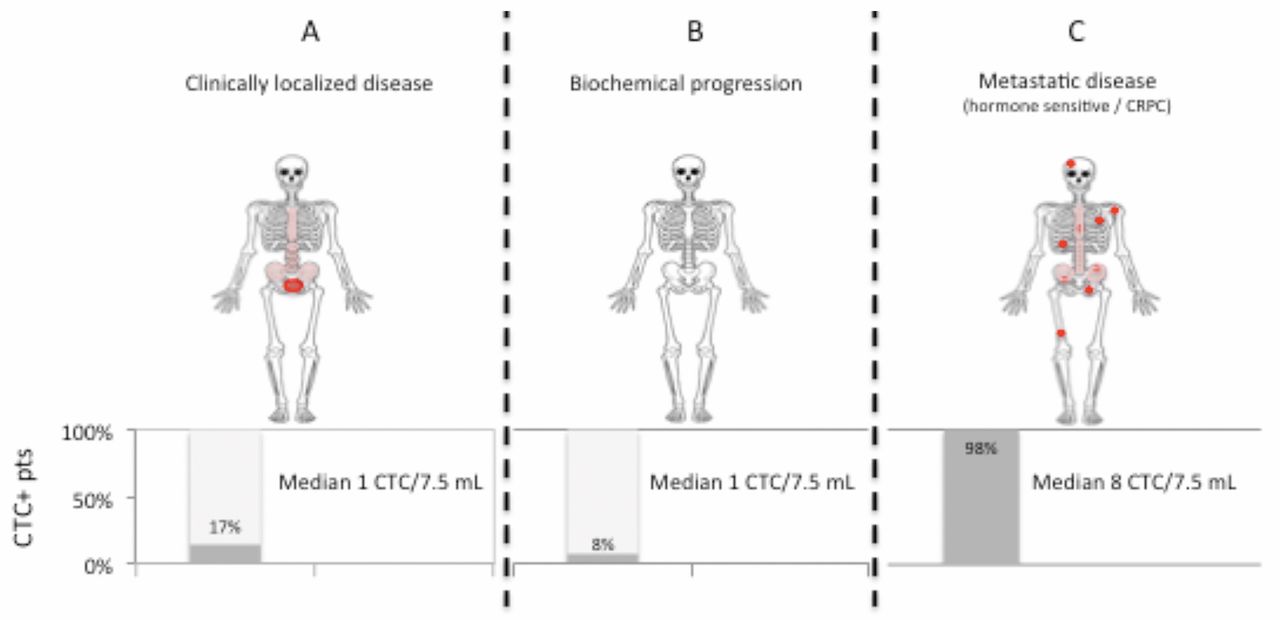
Prostate cancer clinical states and CTCs levels based on literature analysis (Table III). A. Localized disease before treatment. B. Biochemical PSA recurrence. C. Metastatic disease. Red: clinically evident primary disease or distant metastases; Light red: Sites of bone marrow involvement by cancer cells (pre-metastatic niche); red dots: macroscopic bone metastases.
Given the expanding role of circulating tumor cells as a measure to understand tumor heterogeneity and dynamics over time, other technologies are being developed besides the CellSearch system. With regard to PrCa, two technologies have recently obtained significant results. In order to investigate the emergence of resistance to androgen receptor (AR)-directed therapies, Antonorakis et al. used a commercially-available platform (Alere™ CTC-AdnaTest) to study the AR axis. They successfully detected CTCs in over 80% of CRPC patients and identified AR splice variants (AR-V7) with poor predictive and prognostic significance in approximately 50% of on-treatment patients (40). Compared to the lower CellSearch analytical sensitivity, AdnaTest combines EpCAM-based immunomagnetic cell separation with multiplex tumor-specific mRNAs expression analysis allowing for a higher detection rate. In the context of minimal residual disease such as the biochemical recurrence of PrCa, this technology could be useful.
Furthermore, very recently, Scher et al. presented a new platform to study tumor heterogeneity in CTCs from CRPC patients (41). CTCs were studied using a no-selection platform (Epic Sciences™) and analyzed on a cell by cell basis for morphology, protein phenotype and genotype. High CTC heterogeneity resulted as prognosticator of poor survival outcomes and predicted favourable response to taxane chemotherapy.
Although these and others platforms require validation, they represent a step forward in the integration of cell-based- and nucleic acids-based systems for CTCs detection and characterization. Particularly, these new technologies are designed to deal with extremely rare populations of CTCs and sub-clonal alterations.
In conclusion this work confirms previous studies indicating that in patients radically cured for PrCa, PSA biochemical recurrence is not associated with the presence of higher levels of CTCs compared to those observed in the untreated localized disease. Refinement of the cellular and molecular characterization of CTCs in blood and the elucidation of the reciprocal interactions between PrCa cells and the BM niche will provide further insight to help the clinician in the management of the difficult setting of PSA recurrence.
Acknowledgements
The Authors wish to thank the patients and their families for the participation in this study.
This study was funded, in part, by a grant from the Fondazione Comunità Bresciana Onlus.
Footnotes
Conflicts of Interest
The Authors declare that they have no conflict of interest.
- Received April 2, 2016.
- Revision received May 16, 2016.
- Accepted May 17, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}