


Abstract
Aim: Malignant effusion is associated with high serum and plasma levels of vascular endothelial growth factor (VEGF). There are no biomarkers of outcome for bevacizumab treatment in patients with malignant pleural effusion (MPE). We previously reported that carboplatin–paclitaxel plus bevacizumab was effective for patients with advanced non-squamous non-small cell lung cancer (NSCLC) and MPE, although we did not evaluate the relationship between treatment outcomes and plasma or pleural effusion levels of VEGF. Therefore, this study evaluated whether plasma or pleural effusion VEGF might predict bevacizumab treatment outcome. Patients and Methods: We enrolled 23 patients with NSCLC and MPE between September 2010 and June 2012. Plasma VEGF levels were measured in 19 patients and pleural VEGF levels were measured in 22 patients. Results: Compared to patients with a low plasma VEGF level, patients with a high level exhibited significantly shorter overall survival (OS: 13.8 vs. 6.5 months, p=0.04), progression-free survival (PFS: 8.7 vs. 4.8 months, p<0.01), and period to re-accumulation of MPE (pPFS: 9.7 vs. 6.2 months, p=0.02). Compared to patients with a low VEGF level in pleural effusion, patients with a high VEGF level exhibited significantly shorter OS (19.6 vs. 6.9 months, p<0.01) and pPFS (9.6 vs. 6.7 months, p=0.04), although there was no significant difference in their PFS (6.6 vs. 5.9 months, p=0.18). Conclusion: VEGF levels in the plasma and pleural effusion may predict the outcome of bevacizumab treatment in patients with NSCLC and MPE.
- Non-small cell lung cancer
- bevacizumab
- vascular endothelial growth factor
- malignant pleural effusion
- prognostic marker
Non-small cell lung cancer (NSCLC) is the leading cause of cancer-related death in Japan, and most patients experience disease progression. Malignant pleural effusion (MPE) is present in approximately 15% of patients with NSCLC at their diagnosis, and approximately 50% of patients with NSCLC will eventually develop MPE, which influences their management and quality of life (1). Moreover, MPE is associated with a particularly poor prognosis, and the seventh edition of the TNM classification for lung cancer classifies pleural effusion from T4 stage IIIB to M1a stage IV (2).
Vascular endothelial growth factor (VEGF) is a dimeric glycoprotein that is specific to endothelial cells and stimulates angiogenesis. In addition to stimulating new vessel formation, VEGF can strongly promote vascular permeability (3), and MPE is associated with high levels of VEGF in the serum, plasma, and MPE (4-6). In this context, VEGF plays an important role in the development of MPE (7), whereby cancer cells use a VEGF-related mechanism to invade or metastasize into the pleural cavity. Thus, cancer cells can promote high levels of VEGF in the pleural cavity, which can induce the formation and accumulation of effusion (8). In our previous study, we reported that plasma and pleural levels of VEGF were very high in patients with MPE (9). Moreover, previous reports have indicated that high immunohistochemical expression of VEGF, and high pre-treatment serum and pleural effusion levels of VEGF, may be independent predictors of poor survival outcomes among patients with advanced NSCLC (10-12).
Bevacizumab is a recombinant humanized monoclonal antibody against VEGF, and bevacizumab is expected to provide a therapeutic benefit in patients with MPE. In a previous report, bevacizumab with carboplatin–paclitaxel (CP) or cisplatin–gemcitabine was more effective than conventional chemotherapy in patients with advanced NSCLC and non-squamous histology, and these combination chemotherapies are currently considered standard regimens for advanced non-NSCLC (13, 14). However, these trials excluded patients with MPE. Therefore, we performed a phase II study of CP plus bevacizumab in patients with NSCLC and MPE that required drainage. Our results revealed reasonable overall response rate, median overall survival (OS), and median progression-free survival (PFS), that were 60.8%, 11.7 months [95% confidence interval (C)]=7.4-16.8 months), and 7.1 months (95% CI=5.6-9.4 months), respectively (9). However, we did not evaluate the relationship between bevacizumab treatment outcomes and plasma or pleural effusion VEGF levels in those patients, and no other studies have evaluated this potential relationship as far as we are aware. Therefore, we retrospectively analyzed the relationship between VEGF levels and bevacizumab treatment outcomes, in order to determine whether they might predict outcomes in patients with NSCLC and MPE treated using bevacizumab.
Patients and Methods
Study design. The details of our previous phase II study have already been reported (9). In brief, CP was administered as the first cycle, and CP plus bevacizumab was administered every 3 weeks up to a maximum of six total cycles. Patients who underwent four or five cycles of the combination chemotherapy could continue to receive bevacizumab monotherapy until they exhibited progressive disease (PD) or intolerable adverse effects. The protocol for that study was approved by the Institutional Review Boards of both participating centers, and the study was performed in accordance with the Declaration of Helsinki and the Guidelines for Good Clinical Practices. All patients provided their written informed consent prior to undergoing any study-specific procedures. The study was registered with the Japanese University Hospital Medical Information Network (UMIN) (UMIN000005284).
Sample collection and testing. The biomarker analysis was predefined in the phase II study's protocol, and blood and pleural effusion samples were collected from all enrolled patients. Blood samples (5 ml in ethylenediaminetetra-acetic acid) were obtained before the start of treatment and after three cycles of chemotherapy. The pleural effusion samples were obtained before the start of treatment.
The plasma and pleural effusion levels of VEGF were evaluated using AlphaLISA Human VEGF kit (GE Healthcare, Tokyo, Japan), which is a multiplex enzyme-linked immunosorbent assay platform for VEGFA and several other angiogenic factors (assay range ≥31.3 pg/ml).
Statistical analysis. The cut-off date for the analyses in the present study was March 31, 2015. PFS was defined as the time from enrollment to the first instance of confirmed PD or death due to any cause. OS was defined as the time from enrollment to death due to any cause. Data for PFS, OS, and the period from enrollment to re-accumulation of MPE (pPFS) were censored at the last observation. To evaluate the response of MPE, we defined PD as an unequivocal increase compared to baseline MPE, using chest radiographic or computed tomographic findings from during the chemotherapy. However, in order to evaluate the disease control rate for CP with and without bevacizumab, we allowed re-accumulation of MPE during the first chemotherapy cycle (CP only), and PD was defined as MPE re-accumulation during all subsequent cycles.
Kaplan–Meier plots were used to evaluate PFS, pPFS, and OS, which were compared using the log-rank test; the median values and 95% CIs are reported. All analyses were performed using R software (version 2.8.1; http://www.R-project.org), and differences with a p-value of <0.05 were considered statistically significant.
Results
Patients and treatment characteristics. Between September 2010 and June 2012, 23 patients were enrolled. Baseline plasma samples were available from 19 patients (82.6%) and MPE samples were available from 22 patients (95.7%). The characteristics of the biomarker population were similar to those of the entire study sample (Table I).
Baseline biomarker levels. The median plasma VEGF level was 498.3 pg/ml (range: 61.0-1,093.4 pg/ml), and the median VEGF level in pleural effusion was 1,798.6 pg/ml (range:=223.4-35,633.4 pg/ml). Based on these findings, we dichotomized the patients according to the median level of plasma VEGF (500 pg/ml) and pleural effusion VEGF (2,000 pg/ml).
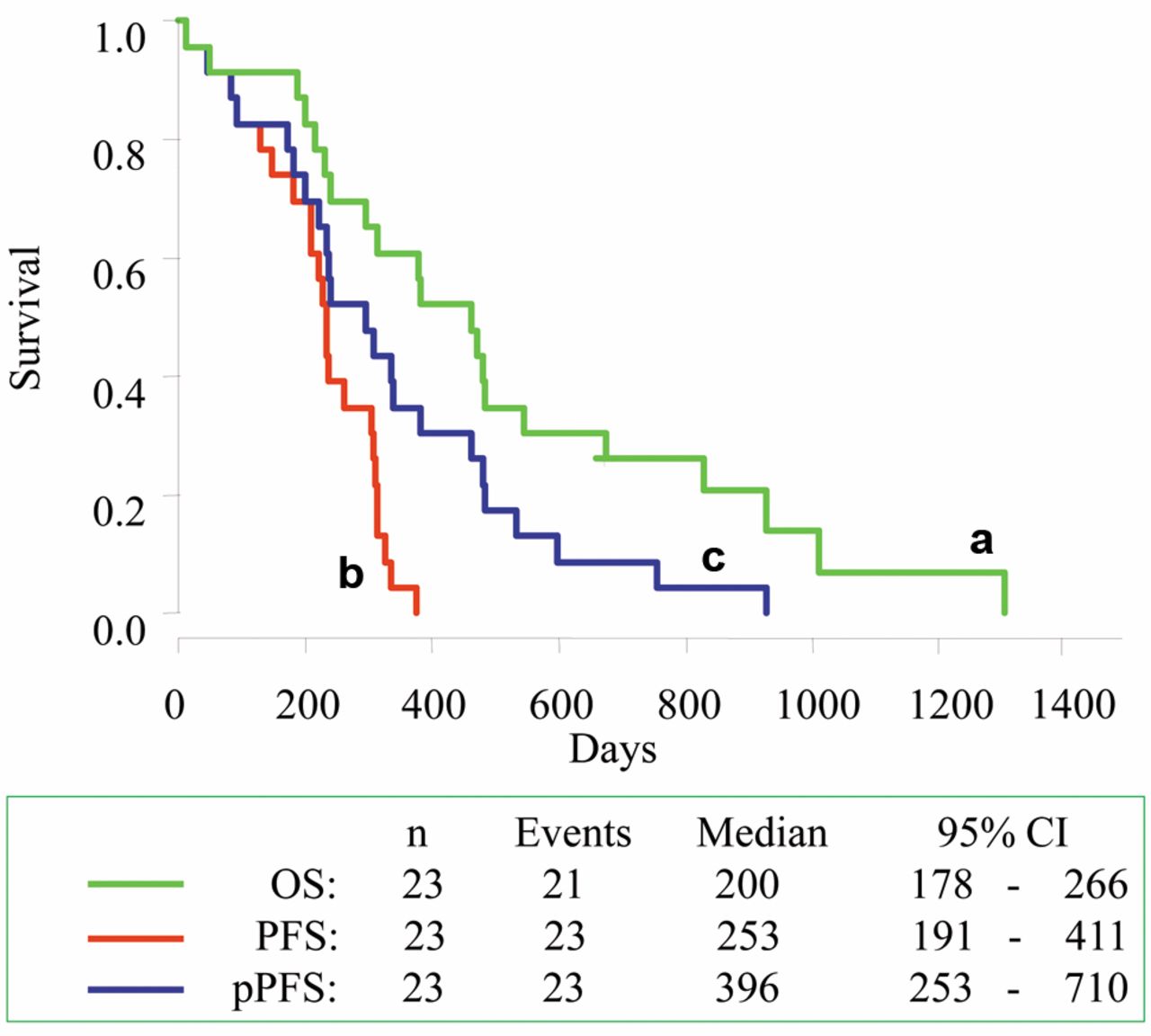
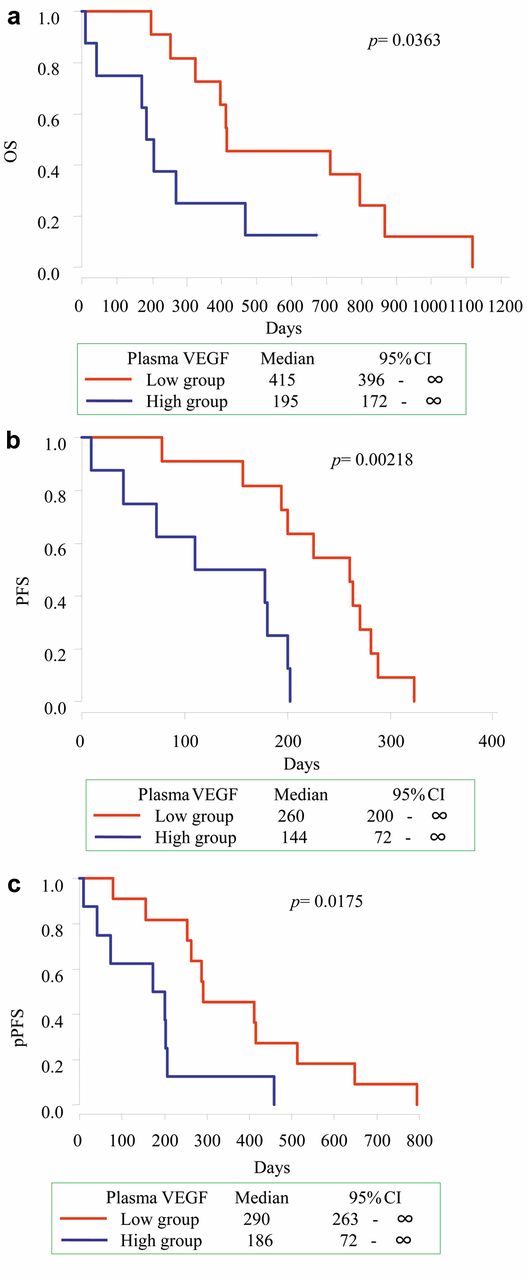
Outcomes and association with biomarker levels. The analyses of all patient outcomes revealed that the median OS was 13.2 months (95% CI=8.4-23.7 months), the median PFS was 6.7 months (95% CI=6.0-8.9 months), and the median pPFS was 8.8 months (95% CI=6.7-13.8 months) (Figure 1). Compared to patients with a low plasma VEGF level, patients with a high plasma VEGF level exhibited significantly shorter OS (13.8 vs. 6.5 months, p=0.04), PFS (8.7 vs. 4.8 months, p<0.01), and pPFS (9.7 vs. 6.2 months, p=0.02) (Figure 2). Compared to patients with a low VEGF level in pleural effusion, patients with a high level also exhibited significantly shorter OS (19.6 vs. 6.9 months, p<0.01) and pPFS (9.6 vs. 6.7 months, p=0.04), although there was no significant difference in their PFS (6.6 vs. 5.9 months, p=0.18) (Figure 3).
Patients' characteristics.
Discussion
To our best knowledge, the present study is the first to reveal that plasma and pleural effusion VEGF levels were associated with PFS, OS, and pPFS among patients with non-squamous NSCLC and MPE who were treated using bevacizumab. Previous studies have reported that platinum-doublet chemotherapy with bevacizumab was more effective than conventional chemotherapy for advanced NSCLC with non-squamous histology, and these combination chemotherapies are currently considered standard regimens for advanced non-squamous NSCLC (13, 14). However, these studies excluded patients with MPE, which precluded any analyses of the relationship between MPE and plasma or pleural effusion VEGF level in patients who were treated using bevacizumab. Therefore, the present study provides important data regarding bevacizumab treatment for patients with MPE.
VEGF is the most potent angiogenic factor, increasing microvascular permeability and stimulating endothelial cell proliferation to prevent the regression of newly-formed vessels. In addition, VEGF plays an important role in the development of MPE by promoting vascular permeability and the leakage of vascular fluid (15). Furthermore, several studies have demonstrated that the plasma or pleural effusion VEGF level in a variety of malignancies is higher than the VEGF level in patients with non-malignant pleural effusion (4, 5, 7). Our findings confirm these reports, as the plasma and pleural VEGF levels were elevated in our patients with NSCLC and MPE.

Kaplan–Meier plots of overall survival (OS) (a), progression-free survival (PFS) (b) and period from enrollment to re-accumulation of malignant pleural effusion (pPFS) (c) in patients with advanced non-squamous non-small cell lung cancer treated with carboplatin–paclitaxel plus bevacizumab. CI: Confidence interval.
Several previous studies have reported a possible association of a poor prognosis in the NSCLC setting with increased plasma, serum, or pleural effusion level of VEGF (12, 16, 17). Furthermore, a similar meta-analysis concluded that a high level of circulating VEGF may predict poor OS among patients with lung cancer (18). However, there are currently no biomarkers or surrogate markers for predicting bevacizumab efficacy, despite numerous phase III studies being performed in a variety of cancer types (19-21). Moreover, the meta-analysis did not reveal any significant association between PFS and the circulating level of VEGF (18). Nevertheless, despite the small sample size, the present study revealed statistically significant associations between bevacizumab treatment outcome and plasma or pleural effusion VEGF level in patients with non-squamous NSCLC and MPE.
In the original phase II study, we reported a significant decrease in plasma VEGF level among all patients who completed three chemotherapy cycles (9). However, bevacizumab provided variable efficacy among the individual patients, despite its universal effect of reducing the VEGF level. Thus, although the present study revealed that a high VEGF level was associated with poor PFS and OS outcomes, there may exist more useful biomarkers. For example, recent studies have evaluated a novel enzyme-linked immunosorbent assay that preferentially detects short VEGFA isoforms, such as VEGF110 and VEGF121, and these studies have suggested that this method provides a promising predictive value (21). Furthermore, angiogenesis is regulated by interleukin-8, and this finding has been confirmed in various types of carcinomas (22, 23), which may indicate that VEGF and interleukin-8 are both biomarkers for MPE (24).
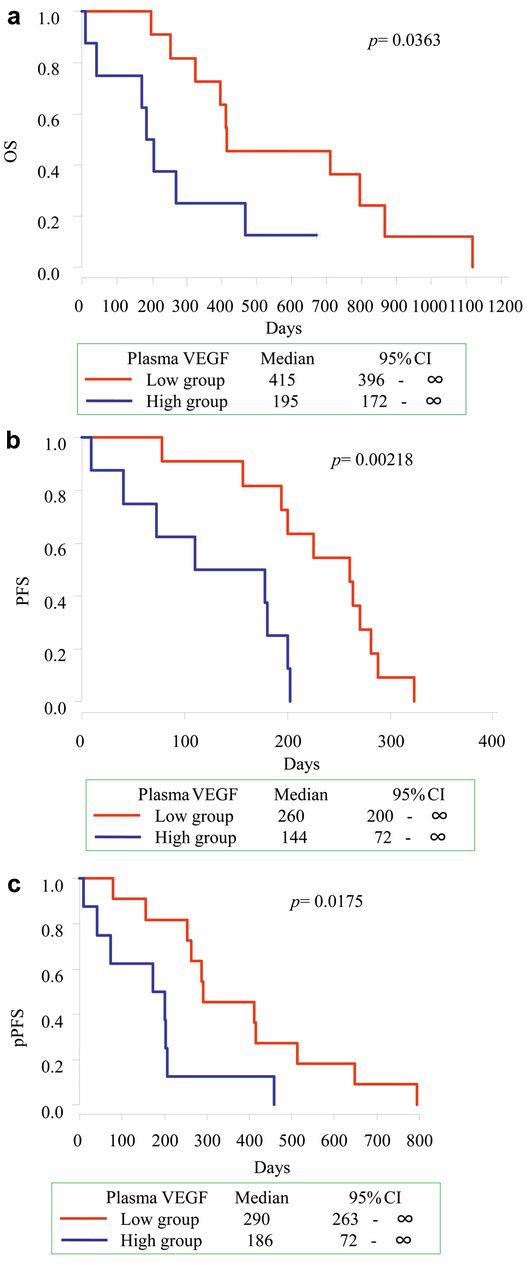
Kaplan–Meier plots of overall survival (OS) (a), progression-free survival (PFS) (b) and period from enrollment to re-accumulation of malignant pleural effusion (pPFS) (c) in patients with advanced non-squamous non-small cell lung cancer treated with carboplatin–paclitaxel plus bevacizumab according to plasma vascular endothelial growth factor (VEGF) level (high group: ≥500 pg/ml, low group:<500 pg/ml). CI: Confidence interval.

Kaplan–Meier plots of overall survival (OS) (a), progression-free survival (PFS) (b) and period from enrollment to re-accumulation of malignant pleural effusion (pPFS) (c) in patients with advanced non-squamous non-small cell lung cancer treated with carboplatin–paclitaxel plus bevacizumab according to the level of vascular endothelial growth factor (VEGF) in pleural effusion (high group ≥2,000 pg/ml, low group <2,000 pg/ml). CI: Confidence interval.
In conclusion, plasma and pleural effusion VEGF levels were associated with survival outcomes in patients with non-squamous NSCLC and MPE who were treated with bevacizumab. This association may indicate that these biomarkers can predict treatment response and prognosis in these patients. However, interleukin-8 may also be an effective biomarker, and prospective clinical studies are needed to validate our findings in patients with lung cancer and MPE who are treated using bevacizumab. A phase II study (UMIN000013329) is currently being performed to compare bevacizumab plus carboplatin or nanoparticle albumin-bound paclitaxel, followed by maintenance nanoparticle albumin-bound paclitaxel plus bevacizumab, as a first-line treatment for chemotherapy-naïve patients with advanced non-squamous NSCLC and MPE.
Acknowledgements
The Authors thank all of the participants in this study.
Footnotes
Conflicts of Interest
The Authors have no conflicts of interest to declare.
Funding
The Authors did not receive any funding for this study.
- Received March 21, 2016.
- Revision received April 26, 2016.
- Accepted April 27, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.