


Abstract
Background: Treatment recommendations in chronic lymphocytic leukemia (CLL) are based upon selected, otherwise healthy study populations mostly under 72 years of age. The Project group Internistic Oncology (PIO) embarked on an analysis of the ‘real-world’ safety and efficacy of bendamustine with and without rituximab in unselected outpatients. Patients and Methods: A multicenter, open-label, prospectively stratified, retrospective study was conducted to determine routine feasibility, toxicity, and response rates obtained by bendamustine with and without rituximab in a random population of mostly elderly patients with CLL. Records were obtained from 775 patients with CLL from 60 private medical oncology practices. Informed consent was obtained prior to study participation. The median observation time was 28 months. Patients were stratified according to age, and treatment. Response criteria and statistics followed international guidelines adopted by the “German Chronic Lymphocytic Leukemia Study Group”. Results: Overall, 57.5% of patients were over 70 (range=36-95) years old. Eastern Cooperative Oncology Group performance status and age influenced the total dose given, decreasing by 20% between ECOG 0 and 3, and by 15% above 80 years old. Response rates did not differ between the ages of 60 to 80 years, with an overall remission rate for bendamustine of 83%, and for the combination therapy of 89%, decreasing above the age of 80 years. Febrile neutropenia occurred in 25% of 775 patients, and grade 3 or 4 non-hematological adverse events in 9.55% (n=74), not interfering with the treatment. Conclusion: Bendamustine with and without rituximab was associated with high activity and tolerability, irrespective of age and risk factors. The median overall survival was 64 months with a 3-year survival rate of 72%; progression-free survival was 30.6 months, and the 3 year PFS was 43%. The good tolerability and feasibility of bendamustine with and without rituximab, in particular for the elderly population with CLL argues for it being a safe outpatient treatment.
The prevalence of chronic lymphocytic leukemia (CLL), the most common form of leukemia of adulthood in the Western hemisphere, is increasing in part due to demographic reasons (1). CLL is a clinically diverse disease originating from B-lymphocytes that may differ in activation, maturation state, or cellular subgroup. In the majority of cases, CLL is an indolent, incurable disease, depending on its molecular genetic profile, modified by biological factors, age and comorbidity. CLL comprises a heterogeneous disease entity: some patients live for decades, never requiring treatment; other courses vary from slowly progressing to an aggressive disease with survival of 2 years or less (2). The etiology of CLL is unclear. The possible influence of environmental and lifestyle factors has not yet been established, (epi)genetic factors do play their part (3). For diagnosis, prognosis, and treatment decisions, hematologists rely on clinical staging systems such as Rai (4) and Binet (5), detailed with the help of cytogenetic factors (2).
Depending on the aggressiveness of the disease course, the clinical (geriatric) assessment, age, comorbidity, staging, cytogenetic analysis, and the exclusion of benign monoclonal B-cell lymphocytosis (6), treatment relying on evidence-based guidelines (7) can be initiated. Exceptions granted, the asymptomatic patient will first undergo a watch-and-wait strategy, in order to observe the individual biology of the disease, defining the required treatment intensity. Treatment recommendations are based upon a number of randomized, prospective phase III trials excluding patients with any comorbidity, and mostly above the age of 72 to 75 years. The impact of age is considered to be relevant to the outcome of systemic treatment (8). Therapy in the elderly population must balance efficacy and tolerability, bearing in mind their diminished organ functions, significant comorbid medical conditions, and possibly interfering co-medication. For these patients, a careful approach is advised, e.g. beginning with a reduced dose initially. Whether this is relevant for the outcome in patients older than 75 years, however, has not yet been established.
The chemoimmunotherapy protocol (CLL8) of the German CLL Study Group (GCLLSG) with fludarabine, cyclophosphamide and rituximab (FCR) has been shown to be currently the most active regimen (9) (objective remission rate (ORR)=95%, clinical complete remission rate (CR)=72%): at a median follow-up of 6 years, the overall survival rate (OS) was 77% and the progression free survival (PFS) 51% (10). However, these findings were associated with increased toxicity: 76% of the patients experienced at least one grade 3 or 4 event; hematological toxicity grade 3 or 4 occurred in 56%.
Clinical studies with bendamustine (B), developed in the 1970's (11) have shown overall response rates (ORR) of 68%, and 88% for bendamustine plus rituximab (BR) in previously untreated patients of 34 to 78 years of age (12, 13). Toxicity was markedly reduced in comparison with the FCR regimen: Because of these favorable results with nearly equivalent activity, the BR regimen is currently considered evidence-based treatment of CLL (14). However, the scientific evidence we rely upon is limited to otherwise healthy, biologically fit patients. Apart from age >65 to 75 years, a long list of exclusion criteria limits the general validity of the results (15-17) for the clinical routine. The Project group Internistic Oncology (PIO) therefore embarked on a follow-up analysis, assessing ‘real-world’ efficacy and safety of bendamustine (B) without, and with rituximab (BR) in four age groups of B / BR – treatment-naïve patients, defining the impact of comorbidity, stage, and Eastern cooperative oncology group performance status (ECOG PS) on dose intensity, and end results. Data were collected using the large PIO registry from private medical oncology practices in Germany.
Patients and Methods
Study design and objectives. We conducted this multicenter, open-label, prospectively stratified, retrospective study to determine the routine feasibility, toxicity, and response rates obtained by bendamustine with and without rituximab in a random population of mostly elderly patients with CLL.
Eligibility. From May 2008 to December 2014, records were obtained from 775 unselected patients with CLL, independent of their line of therapy, consecutively taken care of by 60 private medical oncology practices in Germany, members of PIO. Informed consent was obtained prior to study participation. All patients were included. Data have been reanalyzed yearly up to 2015. The median observation time during data collection was 28 months (842 days).
Treatment. Baseline evaluation included a general medical history, physical examination, routine laboratory studies, serologic tumor markers, and radiographic and ultrasound imaging. Baseline and follow-up diagnostics by bone marrow/histology and cytogenetics (17q-) were performed at the discretion of each participating physician.
The standard treatment protocol as developed in 2005 (18) consisted of rituximab at 375 mg/m2 on day 1 (first cycle; and 500 mg/m2 thereafter) followed by bendamustine at 90 to 120 mg/m2 as a 30-minute infusion on days 1 and 2, q3-4 weeks, varying according to ECOG PS, stage, age and hematological involvement.
The review of the charts showed variations of bendamustine dosage: The mean total dose was 163 mg/m2 (median=160 mg/m2, range=50-300 mg/m2) for at least four, and up to six cycles. Dose reductions of bendamustine and additional cycles, co-medications (corticosteroids, granulocyte colony stimulating factor (GCSF), transfusions) were given at the discretion of the physician.
Prednisone was given concomitantly orally day 1 and 2,days 1-3,days 1-4 at doses ranging from 40 mg to 50/60/100 mg/m2 every 4 weeks. Treatment-related toxicity was evaluated according to WHO criteria (20). Patients were stratified into the following age–treatment groups (age at beginning of therapy): those aged ≤60 years receiving bendamustine; those aged ≤60 years receiving bendamustine with rituximab; those aged >60 to ≤70 years receiving bendamustine; those aged >60 to ≤70 years receiving bendamustine and rituximab; those aged >70 to ≤80 years receiving bendamustine; >70 to ≤80 years receiving bendamustine with rituximab; those aged >80 years receiving bendamustine and those aged >80 years receiving bendamustine with rituximab.
Criteria for response and toxicity. Response criteria followed international standards and guidelines (19), adapted by the GCLLSG (14), modified for routine clinical use: Response rates were defined by clinical and ultrasound examination, lack of B – symptoms, a regular peripheral blood smear, and bone marrow. The primary aim was the clinical ORR (CR) plus partial remission (PR), and stable disease (SD), and toxicity with dose reductions, treatment delays, supportive measures. The secondary aim included the rates of CR, PR, PFS, and OS. Safety measures included adverse events (AEs), use of concomitant medications (e.g. antiemetic's, antibiotics, GCSF). Response was assessed after each cycle, at the end of treatment, and then every 3 months for 2 years, thereafter yearly until 2014. Treatment toxicity was reported by the investigators according to the National Cancer Institute Common toxicity Criteria (CTC) version 3.0 (20).
Statistical methods. We hypothesized that bendamustine with and without rituximab would produce an ORR ≥70%. Statistical analyses for continuous variables are reported as means, medians, standard deviations (SDs), and ranges. Categorical variables are reported using frequencies and proportions. Kaplan-Meier analysis was conducted for PFS and OS. Absolute dose intensity of bendamustine and rituximab (mg/m2/cycle) was calculated.
Patients' demographics and baseline characteristics (n=775).
Patients' characteristics (n=775).
Results
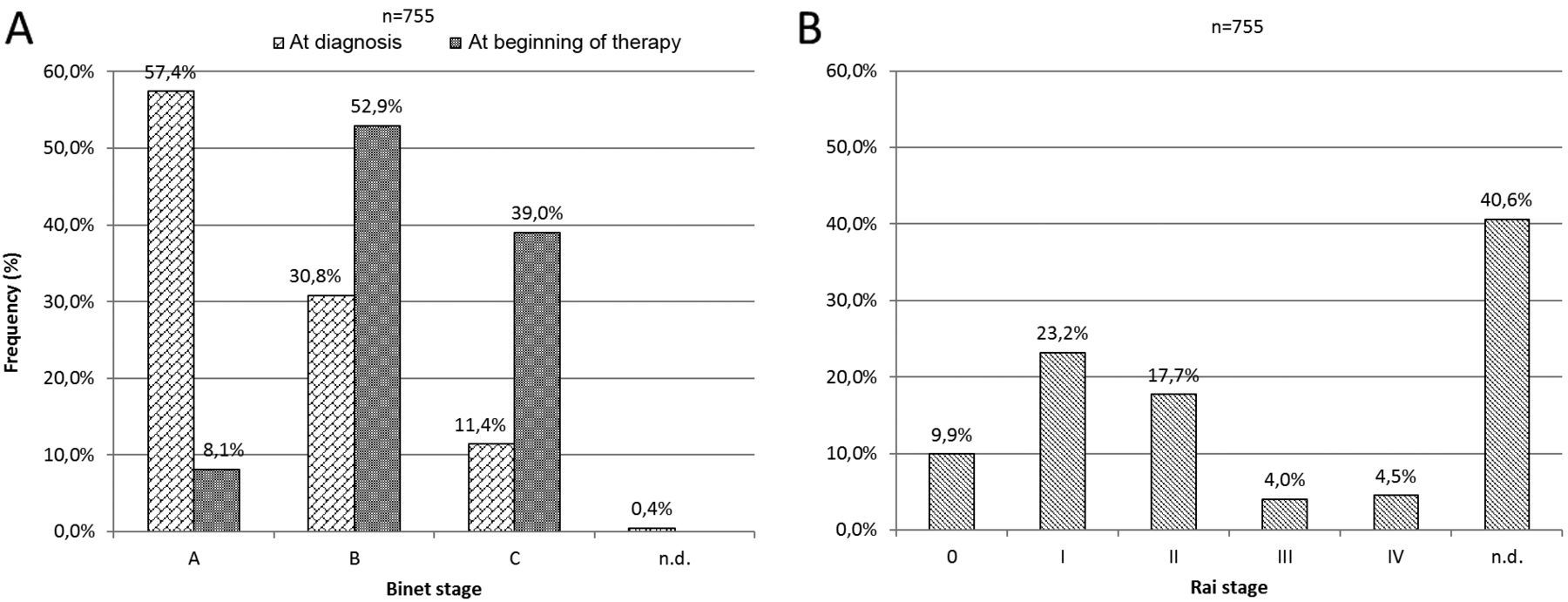
The study enrolled 775 patients with B-CLL, 532 of them (68.6%) treated with first-line therapy. Of the latter, 94 patients (17.7%) received bendamustine alone, and 406 (76.3%) in combination with rituximab. Patient demographics and baseline characteristics are shown in Tables I and II. The majority of patients (445/775=57.5%) were over 70 years of age. The mean age was 72 years, range 36-95 years (Figure 1), with a male to female ratio of 2:1. The majority of the patients (57%) were in Binet stage A, and Rai stage 0 and I (33%) at the time of diagnosis (Figure 2), and had progressed to Binet stage B (53%) when treatment was started. Cytogenetic abnormalities (see Table III), and their frequency were available for 190 patients, of whom 18% had del (17p) corresponding to a high level of risk, and 75% had del (13)(q14) with a low level of risk.
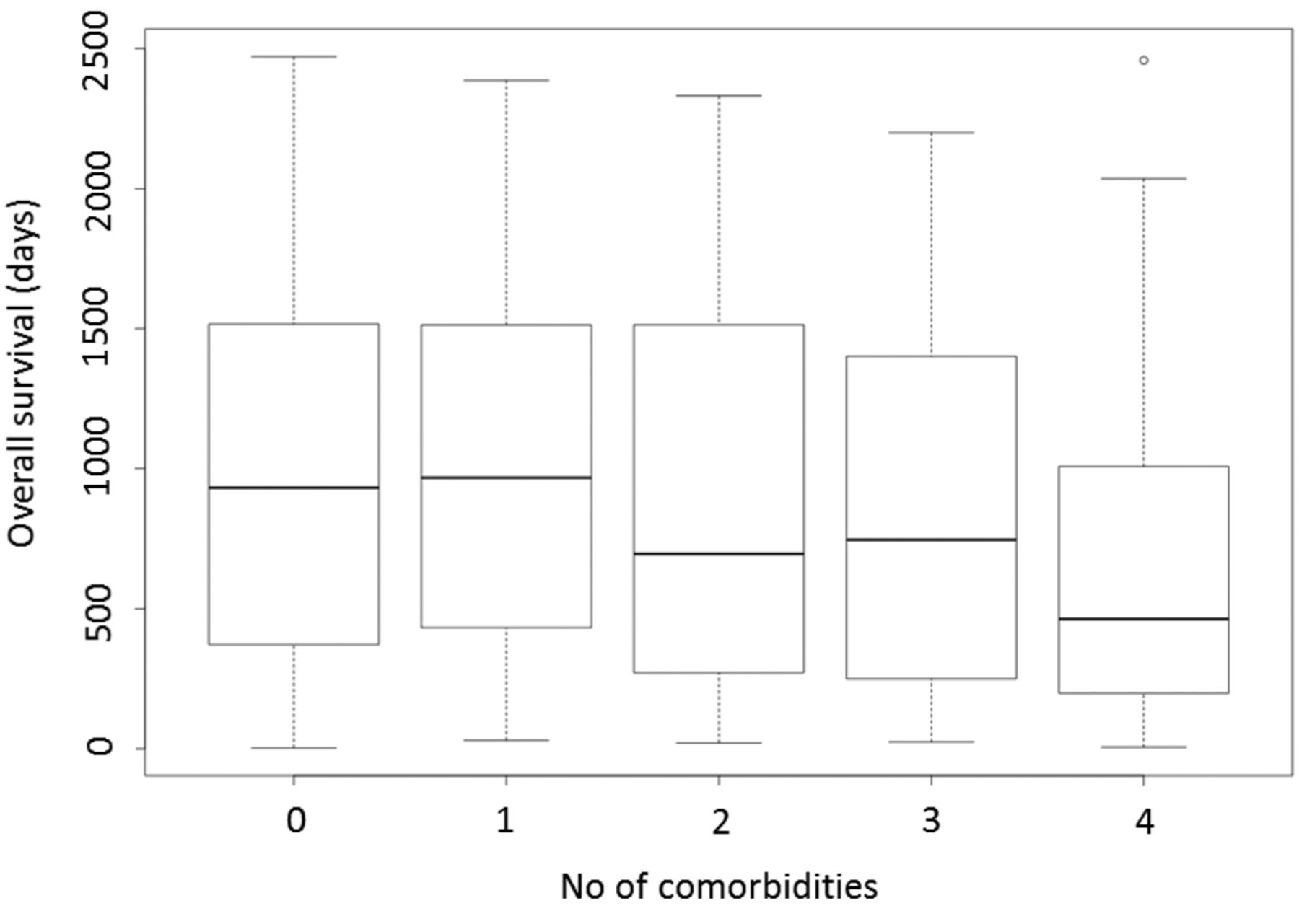
Comorbidities are shown in Figure 3 and Table IV. The number of comorbidities correlated with OS (Figure 4) (p<0.0001), 12% developed secondary autoimmune disease. Using values 1 to 4 for very low to high risk, the risk level was not found to be significantly correlated with age (r=0.076; p=0.304), OS (r=0.046; p=0.537) or therapy response (1 to 2 for PD, NC, PR, CR (r=0.130; p=0.087).

Age distribution at the beginning of therapy.

Binet (A) and Rai (B) stages at diagnosis and beginning of therapy. n.d.: Not documented.
The ECOG PS and age of the patients (r=0.18, p<0.0001) both significantly influenced the total dose given, significantly reducing it by 20% between ECOG 0 and 3, and by 15% from age 60 to 70 years, and above age 80 years.
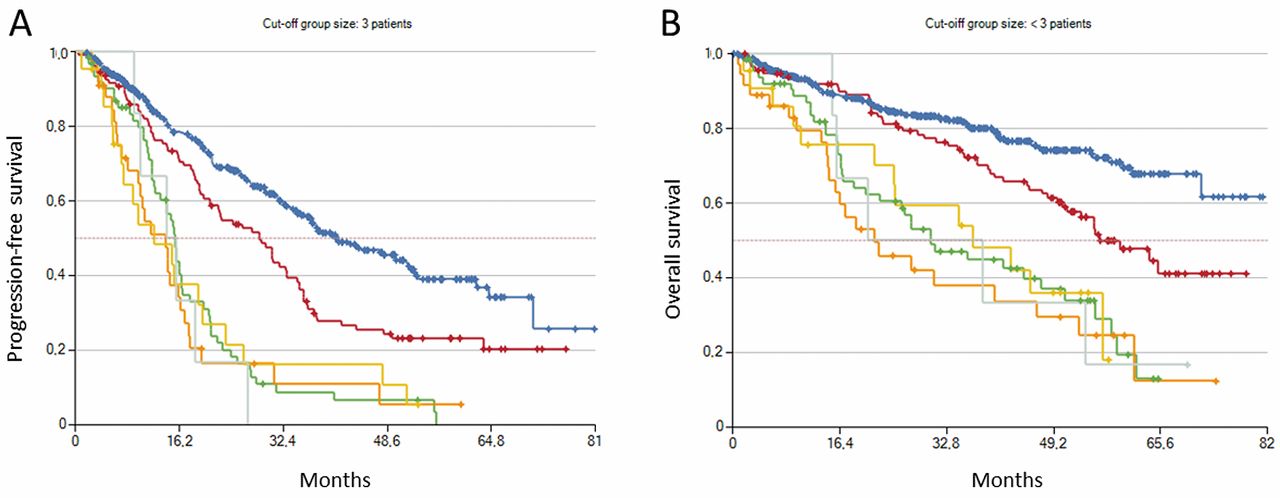
Clinical response rates after first-line bendamustine and bendamustine with rituximab according to age did not differ significantly between 60 to 80 years, with a clinical ORR of 81-83% (p=0.889), and 87-89% (p=0.793), respectively. Comparing ages below 60 and above 80 years showed a decreasing trend in clinical ORR for the combination therapy from 93% to 76% but equal rates of 81-83% (p=0.033) for bendamustine alone (Table V). Bendamustine dose related to ECOG performance status, and to age is shown in Figure 5. With progressing treatment lines, the clinical response rates dropped significantly (r=−0.776, p=0.024) (Figures 6 and 7). As compared to the first and second lines, the third to seventh attempts to improve PFS and OS were ineffective (Figure 8).
In Table VI, the patterns of care summarize dose densities, e.g. delay of the subsequent cycle, and dose reductions, as well as the requirement for GCSF interventions. The mean absolute dose for bendamustine decreased by 20% between age <60 and >80 years, without reducing the response rates accordingly. The clinical ORR for the age groups below 70 years corresponds with the literature, despite an unselected population regarding comorbidity and treatment. The ORR for patients above 80 years fell by about 20%. Granulopoietin (GSF) was dispensed in 0-18% of bendamustine courses, and 12 to 20% of the combination therapy courses, irrespective of age. Hospitalizations occurred in 13-18% of the total treatment courses under bendamustine, and 8-28% under bendamustine with rituximab, increasing with age over 70 years. Treatment delays of up to 1 week were deemed necessary in 3-5% of all cycles, and for over 2 weeks in 2-5%. Increasing age correlated with a non-significant trend for a higher frequency of febrile neutropenia for both therapies, being somewhat more pronounced in the combination groups. Other hematological toxicities, as well as the non-hematological toxicities, appear to be age-irrelevant (Table VII).

Number of patients with comorbidities.

Pearson's correlation of overall survival (OS) and number of comorbidities (p<0.00001).
Cytogenetic abnormality and frequency (n=190).
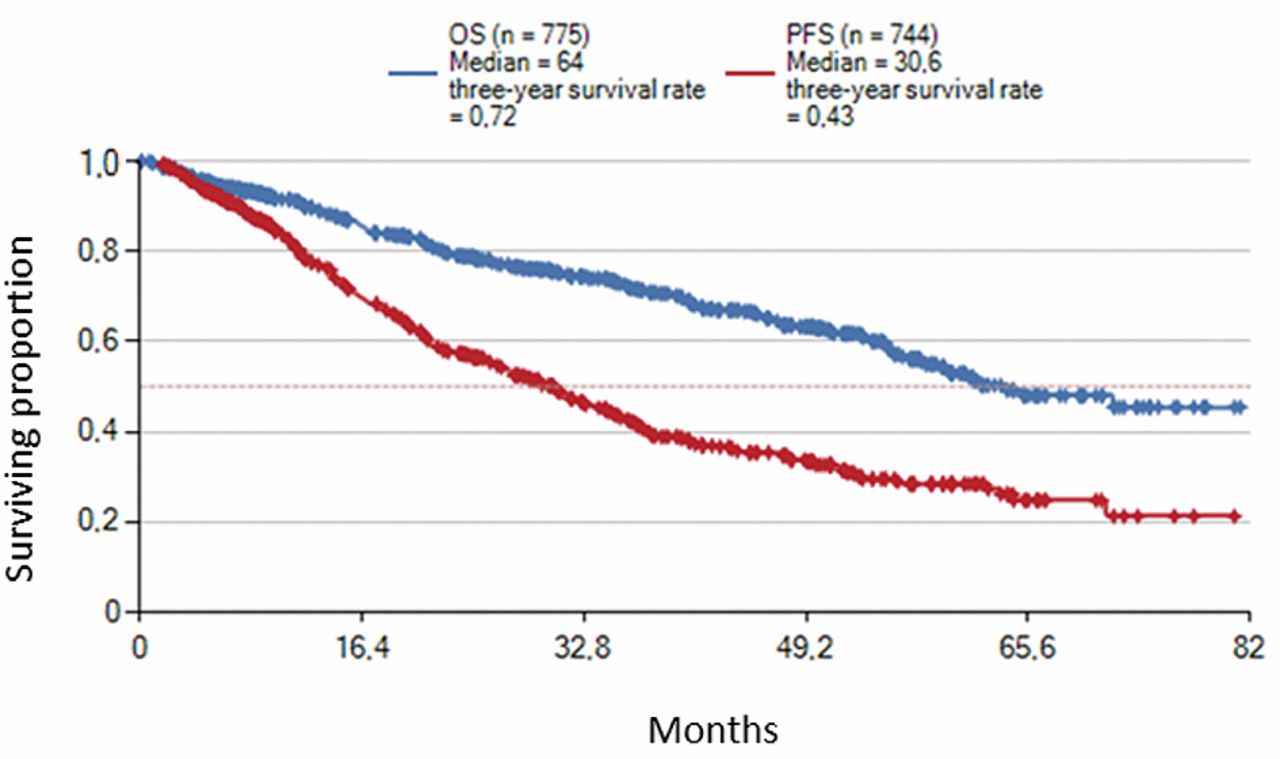
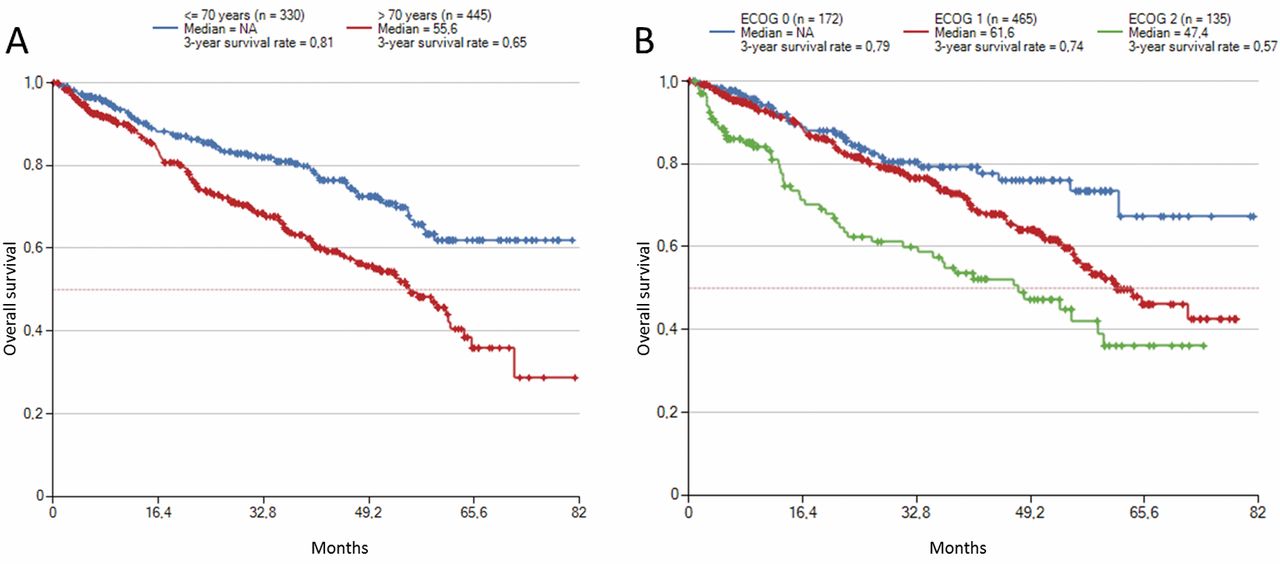
Figures 9 and 10 give the Kaplan-Meier estimates for survival by treatment group. The median follow-up was 27.7 months with 226 patients dead, 138 lost to follow-up, and 42 (5.4%) developing a second malignancy. The median time interval to the next therapy was 17.1 (range=0-68.8) months. The median OS for the total population (n=775) was 64 months, with a 3-year OS rate of 72%. The median overall PFS (n=744) was 30.6 months with a 3-year PFS rate of 43%. As shown in Figures 11 and 12, patients above 70 years of age had a significantly shorter median PFS, and OS compared to younger ones, the median being 10 months shorter: 26.7 rather than 36.7 months (p=0.02). The difference in survival between patients with ECOG 0 and 2 amounted to 20 months (p=0.0001). Age (r=0.197; p<0.0001), and ECOG PS (r=0.073; p=0.041) at the beginning of therapy with bendamustine (n=247) (age: r=0.384; p<0.0001; ECOG: r=−0.131; p=0.04) as well as bendamustine and rituximab (n=528) (age: r=0.139; p=0.001; ECOG: r=0.073, p=0.092) had a significant impact on survival of the total CLL - population. Decreasing doses of bendamustine, given alone or in combination with rituximab, had a significant impact on the remission rates: CR (p=0.003; PR (p=0.057, and no change (p=0.023. Once resistance had developed, increasing the dose intensity of bendamustine was ineffective (Figure 13).
Frequency of comorbidity (≥3%).

Bendamustine dose (median mg/m2) according to Eastern Cooperative Oncology Group (ECOG) performance status (A) and age (B). Correlation (Pearson) ECOG and age: r=0.18, p<0.00001.
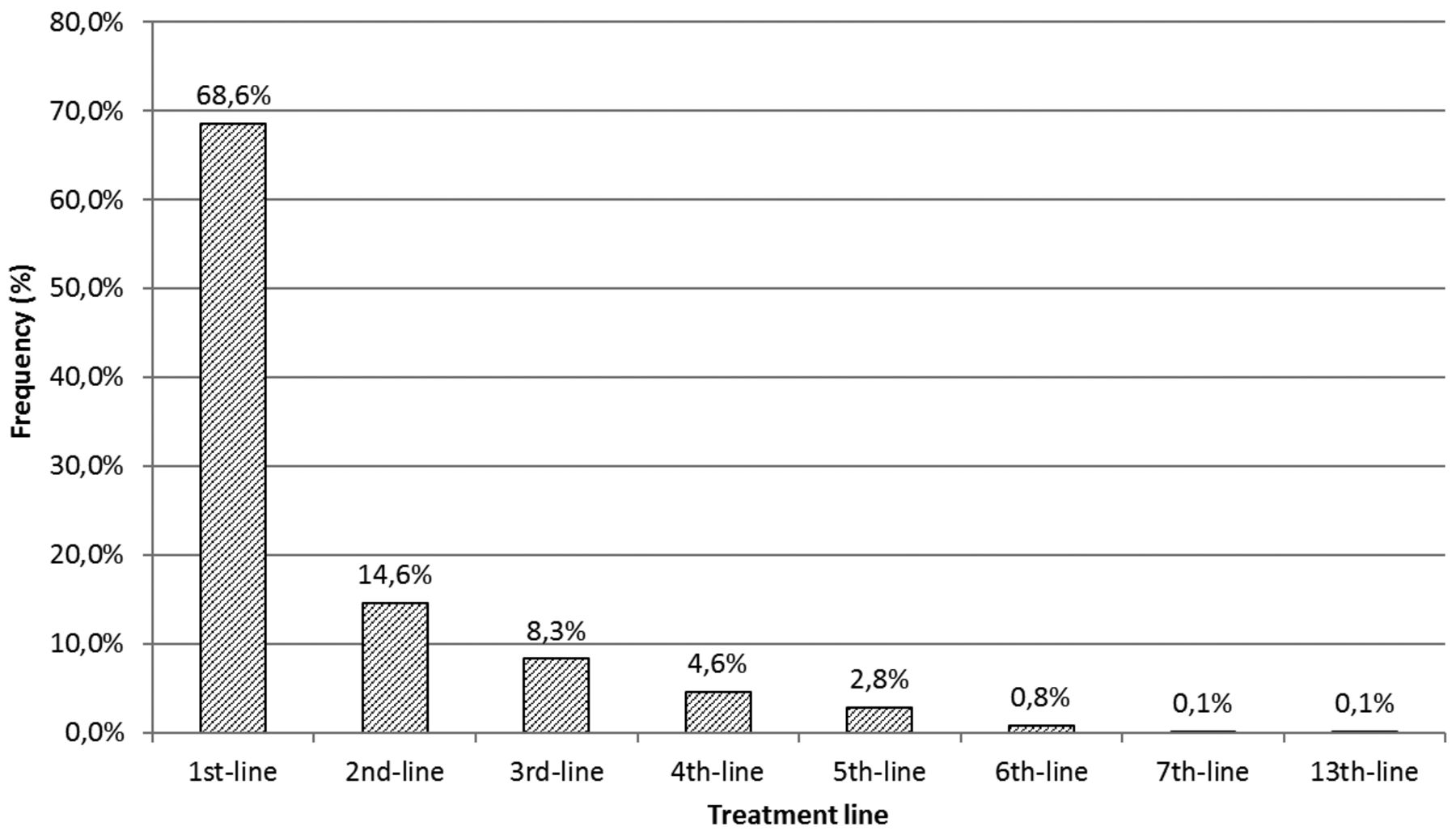
Distribution of treatment lines.

Response rate according to treatment line.

Progression-free (A) and overall (B) survival from start of treatment by line of therapy.
Discussion
To properly select patients with CLL for optimal treatment requires an individual comprehensive assessment of the relevant comorbidity, geriatric assessment if indicated, and the analysis of molecular risk factors – always bearing in mind the prior development, and current presentation of the disease. Good clinical practice and joint decision-making are obligatory in order to reach an optimal outcome for the patient.
Our presentation of 775 unselected patients who presented in 60 outpatient general hematology practices argues convincingly that first consideration should be of the somatic, intellectual and psychosocial fitness of this mostly elderly population, the patient's lifestyle, and endurance. Based on this, the hematological analysis, staging, and definition of biological aggressiveness led to an optimal process defining the necessity, treatment intensity, and onset of treatment. A watch and wait strategy, initially as well as repeatedly during the course of disease, was considered important for electing the proper process, an immediate intervention being rarely necessary.
Factors considered as increasing untoward side-effects and complications were evaluated individually, with only a few being relevant for the dose intensity which was tailored to include patients of any age and PS without the need to withhold treatment.

Total overall (OS) and progression-free survival (PFS) (median in months).
With the introduction of rituximab in addition to chemotherapy, the prognosis of patients with CLL has improved markedly, whilst only increasing the toxicity of the treatment to a marginal degree. This development documented in a number of clinical trials, conducted on selected patient populations, also holds true in general, as was shown in our unselected, retrospective observational documentation. Only for patients older than 80 years, and with a compromised ECOG PS greater than 1 did remission rates and PFS drop significantly. We confirmed that the simultaneous combination of bendamustine with rituximab is an easily managed treatment protocol, limiting the technical and nursing requirements for the hematological team, and improving the quality of life of the patient within days. After a median observational period of 2 years, treatment was started in the majority of patients in Binet stage B (53%) and C (39%), most being in stage A (57.4%) at diagnosis. In only 8% was immediate treatment considered necessary. Up to the age of 70 years, and with an ECOG PS of 0 or 1, full dose intensity could be given. In patients aged 70 to over 80 years, the dose of bendamustine was reduced by a mean of some 15%, keeping that of rituximab unchanged. Febrile neutropenia secondary to bendamustine as well as rituximab, the only relevant hematological complication requiring treatment, occurred in 25% of patients, with a rising, non-significant trend above 70 years. Reductions of dose intensity were necessary in patients aged more than 80 years or with an ECOG PS of more than 1. No patient died from treatment toxicity, dose adjustments avoided further complications. Other grade 3 and 4 non-hematological adverse events, such as fatigue, infections, skin toxicity, and renal impairment with a rising creatinine level, occurred in 9.6% (n=74) of the total population, not interfering with the treatment itself. No manifestations of cardiotoxicity were observed. To avoid unexpected toxicity, it became common practice to start the combined therapy protocol with 50% of the bendamustine dose in the first cycle (omitting day 2), without compromising efficacy to any relevant degree.

Overall (A) and progression-free (B) survival by therapy.

Progression-free survival by age and Eastern Cooperative Oncology Group (ECOG) at begin of therapy (median in months).

Overall survival from start of treatment by age (A) and Eastern Cooperative Oncology Group (ECOG) (B).

Bendamustine dose (median in mg/m2) according to response rate.
Response rates after treatment in all patients. Overall remission rate (ORR) for the whole patient population was 86% (n=664).
Patterns of care (n=775).
Patients with grade 3 and 4 adverse events.
Leukemic transformation is initiated by specific genomic alterations that impair apoptosis of clonal B-cells (21). Knowing the cytogenetic abnormality in an individual patient allows for biological risk stratification, and is helpful in guiding the clinician with regard to prognosis, and follow-up. In our study, such an analysis was obtained in 190 from 775, one-fourth of the documented patients only. The results, however, did not influence the treatment choice, nor was another line of the combination therapy protocol withheld. Results with the combination treatment beyond the second line were disappointing, despite increasing the dose intensity of bendamustine, reflecting rapidly developing resistance. It is, therefore, advisable to limit the combination protocol to the first two treatment phases with four to six cycles each. Bendamustine has been approved by the European Medicines Evaluation Agency (EMEA) for those patients with CLL in whom first line treatment with fludarabine combinations is not appropriate. However, current scientific evidence and guidelines from national and international hematological societies include bendamustine and rituximab as first-line therapy. As documented in the literature (7, 8, 21), and shown in our study, treatment using bendamustine with rituximab has matured to become an international and national standard in particular for the elderly CLL population, and irrespective of risk. In line with the US National Institute of Health, the EMEA and German authorities should license use of bendamustine with rituximab for immediate first-line therapy for CLL.
In conclusion bendamustine, and bendamustine with rituximab as chemoimmunotherapy, has matured to become a useful treatment for patients with CLL, in particular for the elderly population. Our prospectively planned and retrospectively documented observations in 775 unselected patients treated with bendamustine with rituximab gave better results in terms of PFS, and OS compared to bendamustine alone, probably also influenced, however, by differences in age, dosage, comorbidity, and line of therapy. The bendamustine with rituximab combination is rather easy to handle with only minor acute and subacute side-effects, and only occasional WHO grade 3 or 4 toxicity, such as febrile neutropenia, requiring dose adjustments. Reductions of dose-intensity were necessary in patients aged over 80 years, or with ECOG PS of over 1.
Regular daily recreational physical exercise was advised to improve quality of life during therapy and thereafter (22, 23). The survival rates documented in this registry adequately reflect the treatment reality in an off-center outpatient setting, the patients being older with more comorbidity, a worse ECOG PS, and more advanced Binet stages. The reduced dose intensity initially did not appear to negatively affect PFS and OS. It should be noted, however, that the data presented were collected in a registry, and that treatment groups therefore were not composed of randomized, and stratified patient populations. Our aim was to show how CLL patients are currently being treated in every day routine, and with which outcome. Nevertheless, the treatment results turned out to be comparable to those of clinical trials, and underline the quality and feasibility of bendamustine alone and in combination with rituximab in the outpatient setting of private hematological practices.
Acknowledgements
The Authors thank rgb Onkologisches Management GmbH for supporting the registry for the collection of the anonymous patient data.
Footnotes
This article is freely accessible online.
Disclosure Statements
The Authors state that they have no conflicts of interest in regard to this study. The Authors state that they all have contributed to the data presented in this overview.
- Received February 9, 2016.
- Revision received April 19, 2016.
- Accepted April 25, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}