


Abstract
Once considered an obscure tumor entity with poor prognosis, gastrointestinal stromal tumors (GISTs) are nowadays recognized as the most common mesenchymal tumors of the alimentary tract. GISTs differ from other mesenchymal neoplasms at pathology since 90% of them exhibit strong immunohistochemical staining for KIT, a tyrosinase kinase growth factor receptor. In the early 2000s, the ability of imatinib mesylate, a tyrosine kinase inhibitor, to inhibit KIT established a new paradigm for cancer treatment. A reduction in lesion size may not be observed or may appear many months after therapy; thus, tumor response criteria alternative to the Response Evaluation Criteria in Solid Tumors were developed. This review highlights the role of imaging in the detection, characterization, preoperative staging, postoperative assessment, therapy-response evaluation and treatment-related toxicities. All this information is crucial in optimizing patient management. Contrast-enhanced computed tomography is the most commonly used modality for staging the disease and assessing treatment response, whereas positron-emission tomography adds valuable functional information. Magnetic resonance imaging (MRI) may also be useful, especially in ano-rectal GISTs. Diffusion-weighted MRI may provide promising indicators of tumor response to targeted molecular therapy. Radiologists and oncologists should be aware of all these issues related to GISTs, since multidisciplinary teams gathering different expertise are usually needed to properly treat patients with GISTs.
- Gastrointestinal stromal tumors
- multidetector computed tomography
- magnetic resonance imaging
- Response Evaluation Criteria in Solid Tumors
- diagnostic imaging
- review
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumorS of the gastrointestinal tract, with an incidence of up to 14-20 cases per million and a prevalence of about 130 cases per million population (1, 2). GISTs are considered originating from the interstitial cells of Cajal, which are located in the myenteric plexus of the gastrointestinal tract being responsible for its peristaltic contractions (3-5). GISTs differ from other mesenchymal neoplasms at histology since 90% of them display strong immunohistochemical staining for KIT (CD 117), a tyrosinase kinase growth factor receptor (6). The morphological types of GIST are spindle cell (70%), epithelioid (20%), and mixed (10%) (7). Spindle-cell morphology has a worse prognosis than the epithelioid type. Some GISTs are associated with inherited syndromes, notably neurofibromatosis type 1, Carney triad (gastric GIST, pulmonary chondroma and paraganglioma), Carney-Stratakis syndrome (gastric GIST and paraganglioma), and familial GIST syndrome (2, 7). These inherited GISTs differ from sporadic GISTs since they occur at a younger age (first two decades of life) and have a female preponderance, whereas sporadic GISTs can arise at any age, even though more than 80% are reported in individuals older than 50 years (median age=63 years), without any significant difference between men and women (2).
GISTs may occur anywhere along the gastrointestinal tract; they are most commonly located in the stomach (50-60%) and the small intestine (30-35%) and less frequently in the colon and rectum (5%) and the esophagus (<1%) (8). More rarely, GISTs may arise from other intra-abdominal soft tissues within the abdominal cavity, usually in the omentum, mesentery, or the retroperitoneum (<5% of all GISTs); in this latter case it is considered extra-gastrointestinal tract tumor (8). The malignant potential of GISTs ranges from small harmless tumors to aggressive, metastasizing and life-threatening sarcomas (1).
Although most patients have symptoms or a palpable tumor at presentation, 25% of GISTs are incidentally discovered at imaging or surgery, and a few of them (about 5%) are found at autopsy (2). The most frequent symptoms are bleeding into the bowel or abdominal cavity, anemia, and abdominal pain, but others can include dyspepsia, nausea or vomiting, constipation or diarrhea, frequent urination, and fatigue (9). Hemorrhage, tumor rupture, and bowel perforation or obstruction might need emergency surgery; however, symptoms are not predictive of patient survival (9).

Barium imaging in a 48-year-old male with jejunal gastrointestinal stromal tumor. A large exophytic submucosal mass with a sharply defined, smooth filling defect is visible in the jejunum (arrows).
This review presents imaging features of GISTs with emphasis on detection and characterization by different imaging techniques, differential diagnosis, staging and follow-up, including issues related to new molecular targeted therapies.
Imaging Evaluation
GISTs show a wide spectrum of radiological appearances depending on imaging technique and tumor size, site of origin and growth pattern.
GISTs on different imaging techniques. Conventional radiographs may incidentally show a non-specific soft-tissue mass, rarely with calcifications, displacing the gastric air shadow in the gastric location or associated with small intestinal dilatation in the small intestine location (10). Barium imaging has a limited role in staging GI tract tumors by showing the features of intraluminal or submucosal masses, smoothly circumscribed and with the margins forming obtuse or right angles with the gastric wall, usually with sharply defined margins but with some possible luminal irregularity or focal ulceration (Figure 1) (10, 11). These tumors may also show mass effect and cavity and fistula formation may occur (10).

Abdominal ultrasound of a 46-year-old male with gastric gastrointestinal stromal tumor and liver metastasis. Subcostal ascendent ultrasound image shows a 4.7 cm hypoechoic metastasis in the sixth hepatic segment in the subcapsular region (calipers).
Abdominal ultrasound (US) frequently depicts a large mass filling the abdomen, of heterogeneous reflectivity and with frequent necrosis. The site of origin is often undetectable at US (12). Liver metastases from GIST are usually hypoechoic relative to background hepatic parenchyma (Figure 2). Contrast-enhanced US (CEUS) is a useful tool for detecting the presence of viable tumoral tissue in the primary tumor, and in the detection of liver metastases (Figure 3) (13). Endoscopic US is a valuable imaging technique for diagnosing small (<2 cm), incidentally detected submucosal GISTs, by clearly delineating the gut wall layers and also allowing biopsy confirmation (14).
The intraluminal, mural and extra-serosal components of GISTs are better depicted on computed tomographic (CT) images (15). Since GISTs usually involve the outer muscular layer, they usually exhibit exophytic growth. Therefore, the most common appearance is that of a mass arising from the wall of the gastrointestinal tract and projecting into the abdominal cavity (16). Mucosal ulceration is seen on the luminal surface of the tumor in up to 50% of cases (17). The majority of GISTs appear to be well-defined, extraluminal or intramural masses, with varying attenuation on CT based on size.
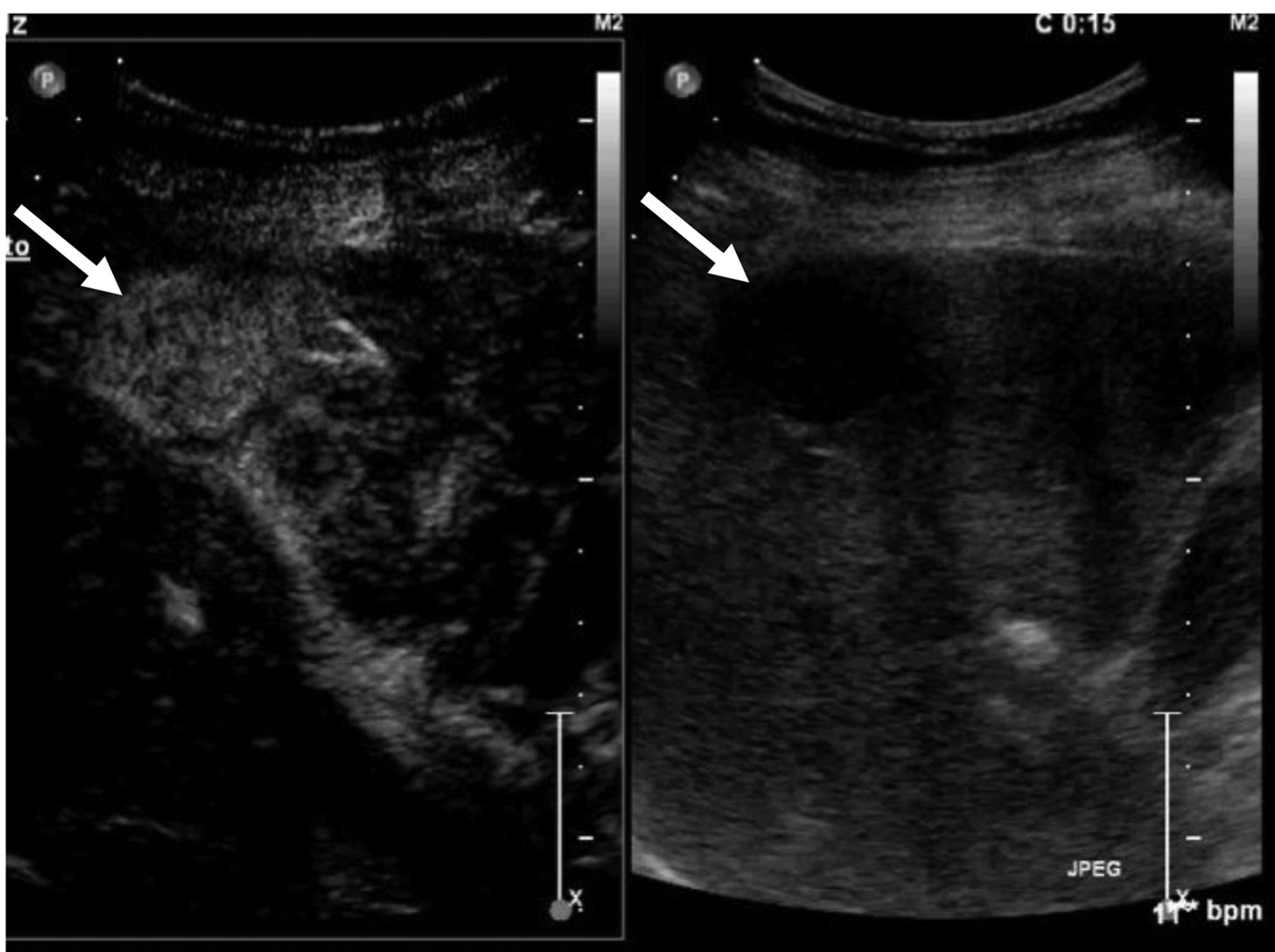
Contrast-enhanced ultrasound in a 70-year-old female with jejunal gastrointestinal stromal tumor and liver metastasis. Intercostal ultrasound image acquired 15 s after i.v. injection of a microbubble-based contrast agent shows a 2.8 cm hypervascular lesion (left side) in the fifth hepatic segment in the subcapsular region (arrows).
Small GISTs (<5 cm), which are usually benign, usually appear on CT as sharply margined, smooth-walled, homogeneous, soft-tissue masses, involving the wall of the stomach or small intestine and often presenting an intraluminal component (18). Moreover, they tend to be homogeneous on contrast-enhanced CT images (Figure 4) although focal areas of low attenuation on CT, due to hypocellular tumor, hemorrhage, necrosis, cystic degeneration and fluid in an ulcer, may be present but without any proven relationship with malignant potential (19, 20).
Larger lesions normally have well- or ill-defined margins, inhomogeneous density both on unenhanced and contrast-enhanced CT scans, with combined intraluminal/extraluminal growth and a tendency to spread to surrounding structures. Large tumors (>6 cm) frequently exhibit central areas of necrosis or hemorrhage, while mural calcifications are rarely seen (Figure 5) (16). Contrast-enhanced CT usually depicts heterogeneously enhancing masses with peripheral enhancing areas due to viable tumoral tissue and central low attenuating areas due to previous hemorrhage, necrosis, or cystic degeneration (10). Large GISTs may also present with a ‘dumbbell-like’ appearance, with masses protruding both into the lumen and growing exophytically from the serosa of the bowel wall (14). Large GISTs may also appear as well-demarcated extraluminal masses, and this appearance can make it difficult to appreciate the real origin of the tumor. Multiplanar reconstructions on multidedector row CT may help in the identification of the organ of origin (15, 21). Calcification, either mottled or extensive, is an unusual feature of GISTs (10, 15). Larger lesions with extensive hemorrhage or necrosis may form large cystic spaces or cavities that may communicate with the lumen and contain air, air-fluid levels, or oral contrast medium (10, 22).
Thanks to its high soft-tissue contrast, magnetic resonance imaging (MRI) allows visualization of the extent of the tumor and central necrosis, including hemorrhage (23). MRI findings confirm that small GISTs tend to be round and with strong homogeneous arterial enhancement, whereas large GISTs tend to be lobulated and usually show mild, heterogeneous, gradual enhancement with intratumoral cystic change (24). The degree of necrosis and hemorrhage greatly affects the signal-intensity pattern. The solid portions of tumor typically exhibit low signal intensity on T1-weighted images, high signal intensity on T2-weighted images, and enhancement after administration of contrast medium (10). Areas of hemorrhage within the tumor will exhibit from high to low signal intensity on both T1- and T2-weighted images, depending on the age of the hemorrhage (25). MRI is a useful adjunct to CT, particularly in the evaluation of large tumors (22, 26).

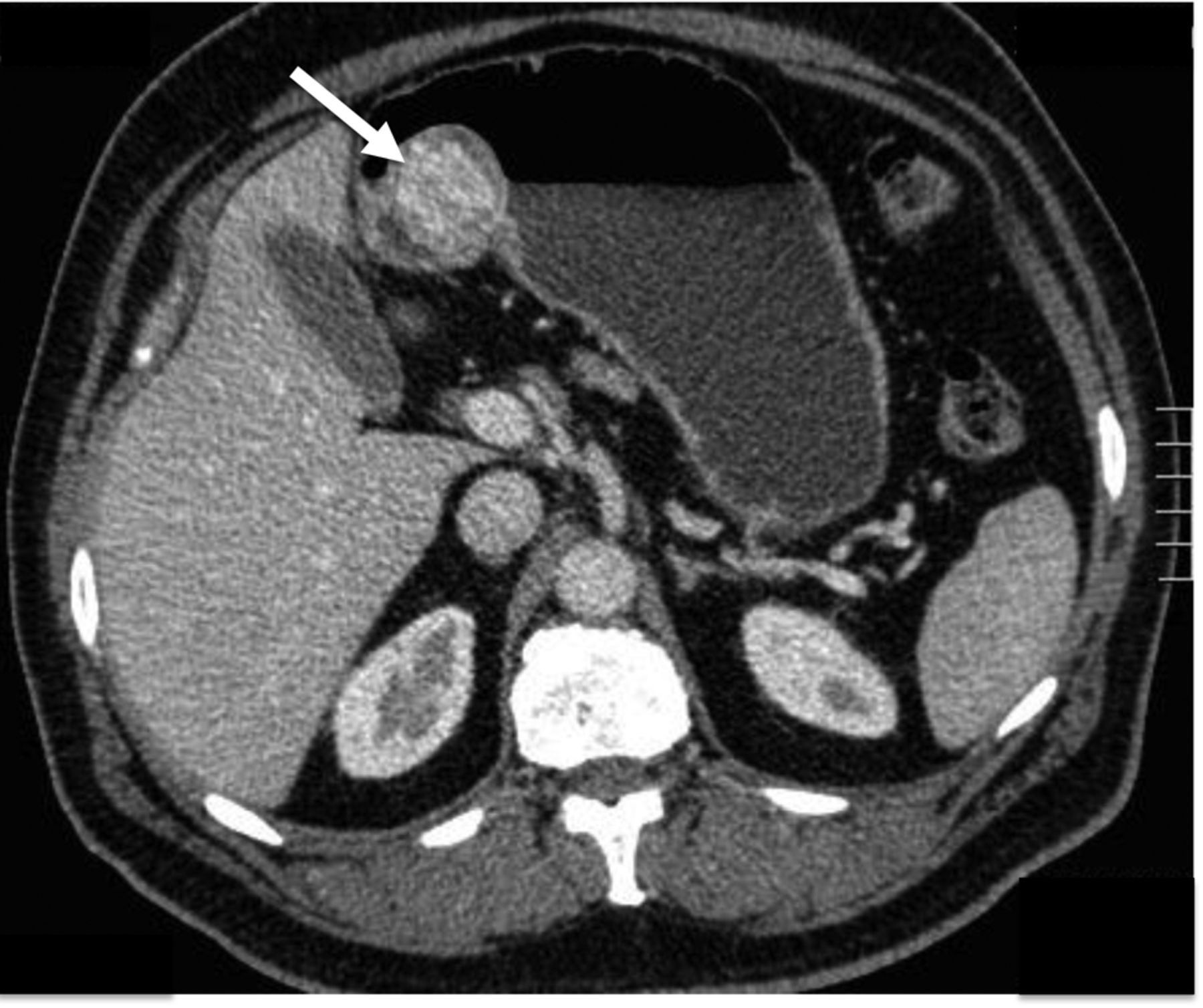
Contrast-enhanced computed tomography in a 60-year-old male with gastric gastrointestinal stromal tumor. Contrast-enhanced computed tomographic in the portal phase depicts a small intraluminal submucosal mass with sharply defined margins and homogeneous contrast enhancement in the stomach (arrow).
Differential diagnosis of GISTs depending on location. Gastric GISTs must be differentiated from other mesenchymal neoplasms that may arise in the gastric wall such as leiomyomas, leiomyosarcomas, schwannomas, neurofibromas, and neuroendocrine neoplasms (e.g. solitary gastric carcinoids). In a series of 120 patients, non-cardial location, heterogeneous enhancement, presence of necrosis, larger lesion size, and absence of lymphadenopathy are highly suggestive CT findings for large gastric GISTs in differentiation from schwannomas or leiomyomas (27). Gastric schwannomas more frequently exhibit an exophytic or mixed growth pattern, homogeneous enhancement pattern and peritumoral lymph nodes and grow more slowly than GISTs (28). Gastric adenocarcinoma and lymphoma rarely demonstrate marked exophytic growth, but they may occasionally mimic GISTs, with a predominantly mural location or an intraluminal component. Advanced gastric carcinomas and lymphomas commonly have associated perigastric, hepatoduodenal ligament, and celiac lymphadenopathy, which are not usually seen in malignant GISTs (29).
Duodenal GISTs are well-circumscribed, round or oval masses, and more commonly occur in the second portion of the duodenum, without lymphadenopathy or duodenal obstruction. Duodenal GISTS frequently metastasize to the liver and peritoneum (30). The differential diagnosis for small intestinal GISTs includes primary and metastatic small intestinal neoplasms. Adenocarcinoma is the most common primary malignancy of the small bowel, usually appearing as an annular lesion in the proximal small intestine; thus, its appearance usually does not overlap with that of GISTs. Lymphoma, however, produces large masses within the small intestine that may ulcerate, cavitate, and extend into the adjacent mesentery. In these cases, lymphoma may be indistinguishable from a GIST on radiological images, although the presence of associated lymphadenopathy would favor a diagnosis of lymphoma (10).
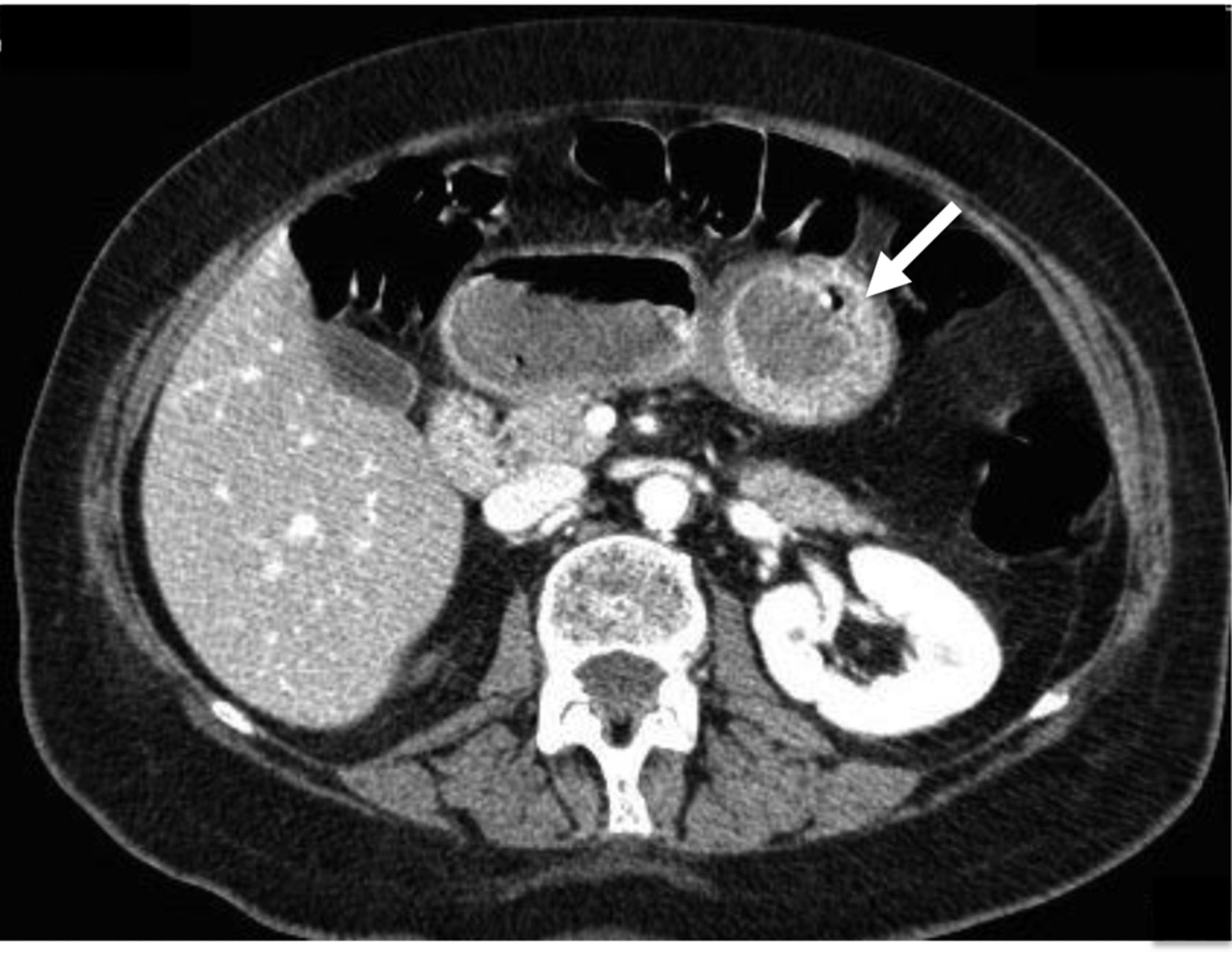
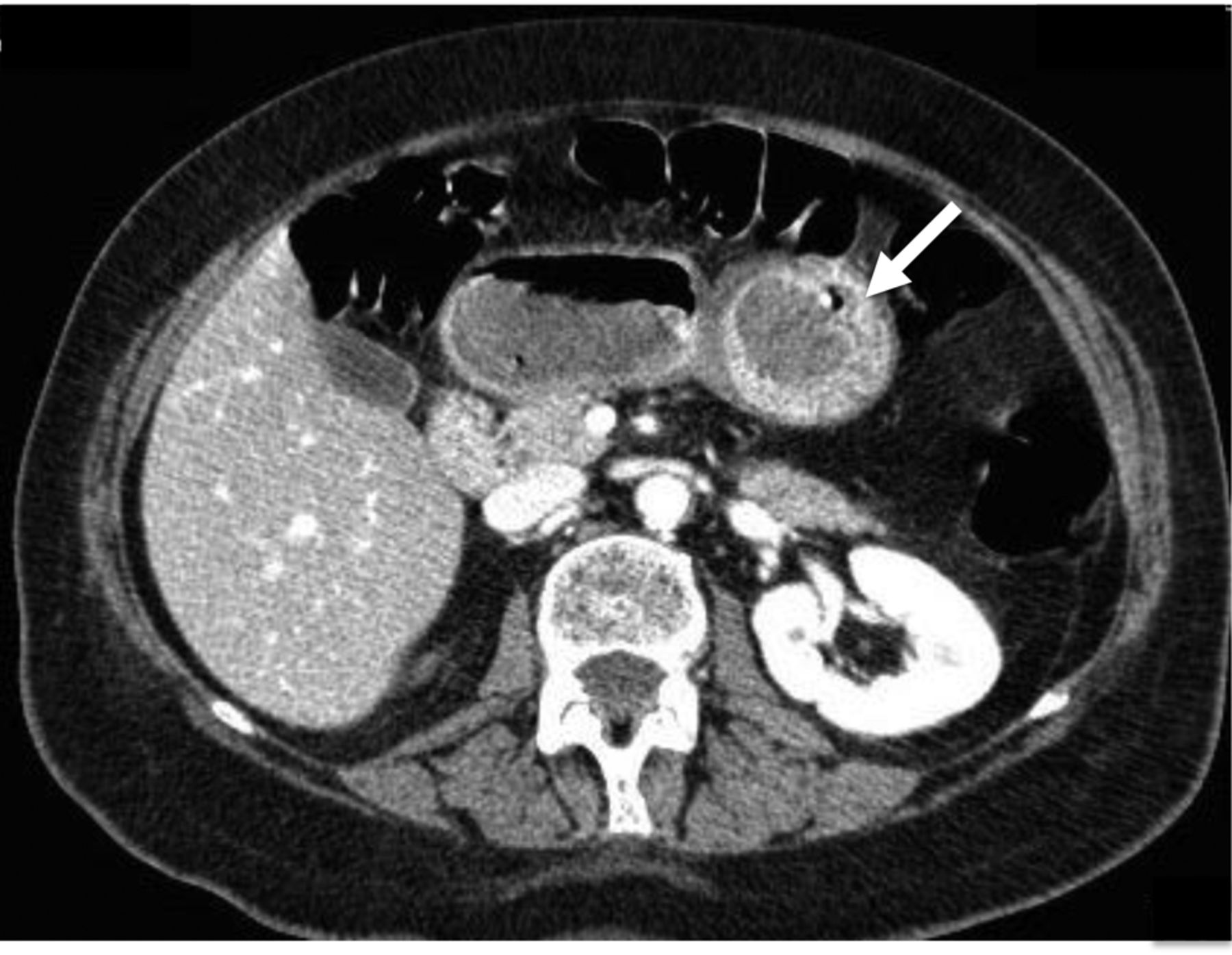
Contrast-enhanced computed tomography in a 72-year-old female with gastric gastrointestinal stromal tumor. Contrast-enhanced computed tomography in the portal venous phase depicts an intraluminal submucosal mass with a sharply defined margin, but inhomogeneous contrast enhancement in the stomach (arrow).
Neoplasms that originate from the mesentery and secondarily involve the small intestine, such as mesenteric fibromatosis (desmoid tumor), inflammatory pseudotumor, lymphoma, sclerosing mesenteritis, and metastatic disease, should also be included in the differential diagnosis (10).
Anorectal GISTs are well-circumscribed, non-circumferential, predominantly infralevator, intramural or exophytic, fluorodeoxyglucose (FDG)-avid, hypoattenuating masses, and present without lymphadenopathy or intestinal obstruction (31). Cross-sectional imaging allows a good visualization of the origin of the mass, its internal components, and other organ involvement, and is indicated for surgical planning (26). The differential diagnosis for anorectal GISTs includes both epithelial and nonepithelial neoplasms of the anorectal region. Rectal adenocarcinoma, anal squamous cell carcinoma, lymphoma, malignant melanoma, carcinoid, leiomyoma, and leiomyosarcoma may have imaging appearances similar to that of GISTs, although leiomyosarcoma may have a dominant polypoid intraluminal component (10). Carcinomas tend to have irregular margins and may be associated with perirectal lymphadenopathy, whereas GISTs tend to have well-defined margins without any perirectal adenopathy. GISTs with perirectal extension may be mistaken as tumor arising from adjacent structures, such as prostatic adenocarcinoma or sarcomas of the prostate and perineum. Anorectal lymphoma may be seen in patients with AIDS; radiographically it presents as an eccentric or annular mural mass that may be associated with mucosal ulceration or perianal fistulation.
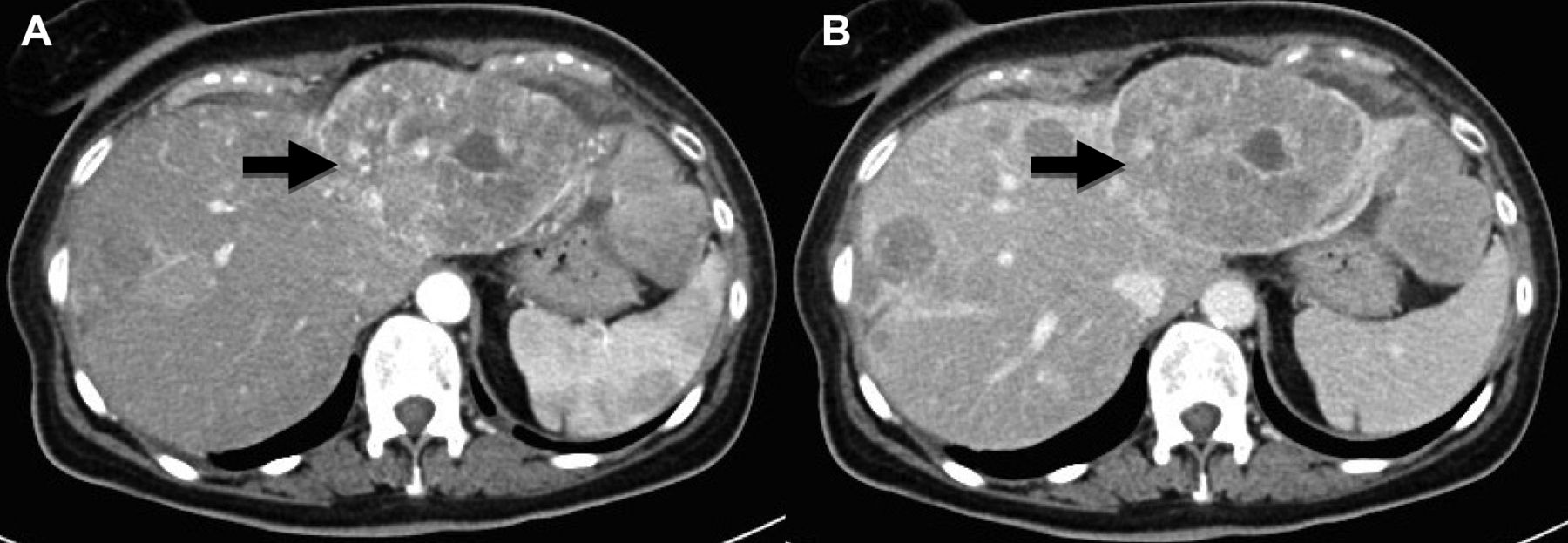
Contrast-enhanced computed tomography in a 70-year-old female with jejunal gastrointestinal stromal tumor liver metastasis. Contrast-enhanced computed tomography in the arterial phase (A) depicts a large, inhomogenoeus, hypervascular metastasis in the left lobe of the liver (arrow). In the portal phase the lesion shows ‘wash-out’ (arrow) (B).
Primary esophageal and colonic GISTs, as well as mesenteric or omental GISTs, are much less common than gastric, small bowel, and anorectal GISTs (10).
Pre-operative staging. Since 30% of GISTs are frankly malignant, an accurate assessment is crucial in order to identify resectable disease and to evaluate the need for adjuvant or neo-adjuvant therapy. The clinical diagnosis is mainly based on imaging, as biopsy runs the risk of tumor rupture or seeding of the biopsy tract, in otherwise resectable disease (32). When recommended, a biopsy sample obtained by endoscopy is preferable to transcutaneous biopsy because of the lower risk of tumor spillage into the abdominal cavity. If accessible liver metastases are present, a biopsy specimen from a metastasis can establish the diagnosis (2). Contrast-enhanced CT is the investigation of choice in the imaging algorithm of GIST. Usually GISTs displace adjacent organs and vessels, whereas direct invasion of the adjacent structures is rarely seen, usually in advanced disease (15). CT and MRI may also demonstrate omental and peritoneal spread of tumor, or liver metastasis, whereas ascites and metastatic lymphadenopathy are uncommon features (10). Extension of gastric GISTs may occur into the gastrohepatic ligament, into the gastrosplenic ligament, or posteriorly into the lesser sac (10). The main sites of metastases are the liver and the peritoneal cavity, including the omentum and the mesentery (33). Hepatic metastases are usually hypervascular on arterial-phase images with wash-out in the venous phase and can remain occult on portal venous-phase images or in single-phase scans (Figure 6) (34). Rarely GISTs metastasize to the lymph nodes, bones, lungs, or to subcutaneous tissues (35). The presence of an ulcer, mesenteric fat infiltration, direct organ invasion, and metastasis were more frequently observed in gastric GISTs with a high mitotic rate, but no CT feature other than size was found to have any predictive value (36). Furthermore, although the risk of metastases is highest in patients with large tumors with a high mitotic index, small tumors with low mitotic activity may still metastasize, making it difficult to reliably predict malignant potential (37). The correlation between the degree of contrast-enhancement and the malignant potential of GISTs is still unclear. In a study focused on MRI, markedly enhancing GISTs had a high mitosis index (23). On the other hand, on MRI, the presence of intratumoral cystic change and a low mean apparent diffusion coefficient (ADC) value were found to be helpful for predicting the high malignant potential of GISTs, but no correlation was found between the degree of enhancement and risk of malignancy (38). For large exophytic tumors and GIST of the anorectum, the multiplanar capability of MRI may be of particular importance in determining the organ of origin of large tumors and the relationship of the tumor to other organs and major blood vessels (22, 26).
Positron-emission tomography (PET) provides functional information that may help in staging, especially when combined with morphological information provided by CT (22). PET/CT may be useful for differentiating viable tumour from necrotic tissue, malignant from benign tissue, and recurrent tumor from scar tissue, especially acting as a baseline, pre-treatment scan (22).
Post-operative surveillance. The optimal treatment for GISTs is surgical resection, although even after complete (R0) resection, a substantial proportion of patients will suffer disease recurrence, with an overall 5-year survival ranging between 40 and 65% (39). In a pooled analysis of data from 2,459 patients, estimated 5- and 15-year recurrence-free survival rates for GISTs treated with surgery alone were 70.5% and 59.9%, respectively (8). Only a few tumors recurred after the first 10 years of follow-up, suggesting that most patients (about 60%) with operable GIST are probably cured by surgery (2). The most important independent prognostic factor for GIST recurrence after surgery is a high tumor mitotic rate but also large tumor size, tumor site (gastric GISTs being less aggressive than other GISTs), and tumor rupture before surgery or at surgery have been identified as independent prognostic factors for recurrence (2, 6, 40-43). Hence, these prognostic factors have been used to create the modified US National Institutes of Health classification (43).
Since extra-abdominal metastases are infrequent, contrast-enhanced CT or MRI of the abdomen and pelvis is usually adequate for post-operative surveillance, but the optimum follow-up scheme is still subject to debate (2). The high incidence of GIST recurrence in the high-risk group in the first 3 years after surgery supports the use of intensive imaging surveillance (i.e. intervals of 3-4 months) during this period. Relapse is often asymptomatic and commonly occurs in the liver, omentum and mesentery. Stratification by tumor factors and replacing CT with MRI for young people may enable improved tailoring of surveillance protocols within the high-risk group in the future (44).
Response assessment of treated GISTs. In the early 2000s, the knowledge of the pathogenic role of activating mutations in the receptor tyrosine kinase KIT and the ability of imatinib mesylate, a small-molecule tyrosine kinase inhibitor (TKI), to inhibit KIT established a new standard of care for treating KIT-positive, inoperable, and metastatic GISTs (34, 45). Before the imatinib era, the median survival of patients with recurrent or metastatic GIST was 10-20 months, whereas after the introduction of TKI, survival rose to 51-57 months (46-48). Nowadays, first-line systemic treatment of advanced GIST is with imatinib, unless the tumor has a gene mutation that encodes an imatinib-resistant kinase. Thanks to imatinib, 83-89% of patients will have either a response or a durable stable disease, whereas only 11-17% of cases will progress (47, 49). Response evaluation during early stages of targeted therapy is crucial in order to optimize treatment and prevent unnecessary delays, toxicity and costs (50, 51).
Contrast-enhanced CT is the most commonly used modality for evaluating response to treatment of GISTs. Multiphasic CT with unenhanced, arterial-, and venous-phase images helps better define both the primary tumor and metastatic disease. Unenhanced CT images help detect hemorrhage and calcifications (although these are uncommon) and act as a baseline for assessing enhancement (15, 34, 52, 53). According to the Response Evaluation Criteria in Solid Tumors (RECIST), tumoral response to conventional cytotoxic drugs is categorized as partial response, stable disease, and progressive disease on the basis on the size reduction of a tumor using one-dimensional measurement (54, 55). However, targeted therapies will also determine changes in the tumoral composition, such as cystic areas or calcifications. These changes, as well as reduced lesion vascularity, cavitations and intratumoral hemorrage, are evidence of disease response in patients after imatinib therapy, even without any size reduction (56, 57) (Figure 7). Thus, RECIST criteria might not be a reliable indicator for monitoring metastatic GISTs, especially in the early stage of imatinib treatment (58). Considering that imatinib acts more as a cytostatic than cytotoxic drug, treated metastatic lesions often exhibit minimal vascularity and cellular density, with extensive cystic or myxoid degeneration and no necrosis or inflammation (59). Paradoxically, instead of a decrease in size, a transient increase in size may be seen early in some cases owing to cystic change and intratumoral hemorrhage (60). Hence, alternative tumor response criteria were developed by Choi et al. in order to incorporate density changes along with size reduction (61). According to the Choi criteria, a decrease in tumor CT attenuation by 15%, or 10% decrease in unidimensional size is indicative of treatment response, as opposed to a 30% decrease in the longest dimension by RECIST (61). Furthermore, the early detection of a nodule within a mass is an important sign of recurrent GIST, as well as the appearance of new solid lesions after maximal dose of imatinib suggesting disease progression, and might be helpful in early intervention such as surgery or use of new tyrosine kinase inhibitors (62, 63). Choi response criteria are reproducible, more sensitive, and more precise than RECIST in assessing the response of GISTs to imatinib and correlate with time to tumor progression and disease-specific survival (64).
PET has been found to be highly sensitive in detecting early response, and to be useful in predicting long-term response to imatinib in patients with metastatic GIST (65). The European Organization for Research and Treatment of Cancer (EORTC) has provided both qualitative and semi-quantitative criteria of FDG uptake, such as the standardized uptake value (SUV), to assess metabolic response (66, 67). A decrease of more than 25% in the maximum SUV from the baseline value was documented within the first month of imatinib therapy and as early as 24 h after a single dose of imatinib (68). The integration of FDG-PET and CT, as in the combined hybrid PET/CT scanners now available, offers a way to optimize the evaluation of patients with GIST treated with molecularly targeted drugs, as well as providing a problem-solving technique when CT or MRI are inconclusive (69). However, in more than 20% of lesions, glucose uptake before treatment is not sufficient as to be detected with PET, thus reducing its clinical applications (70).

T2-Weighted fast spin-echo magnetic resonance imaging (T2-w FSE MRI) in a 57-year-old female with jejunal gastrointestinal stromal tumor and liver metastasis. A: T2-w FSE MRI shows a moderately hyperintense metastasis in the fifth segment (arrow). After 5 months of imatinib therapy, T2-w FSE MRI shows lesion enlargement (arrow) with markedly hyperintense areas of cystic change (B) and T1-w gradient echo image in the portal phase after intravenous injection of gadolinium well depicts peripheral areas of contrast enhancement due to viable tumoral tissue (arrowhead) and central area of cystic change (asterisk) (C).
Diffusion-weighted MRI (DWI), a particular techique sensitive to the microscopic motion of water molecules, may provide a functional quantitative indicator, the ADC, as a surrogate marker of tissue cellularity (71-73). On DWI, response to treatment is indicated by increase in ADC values compared to the pretreatment values, and may be seen as early as 1 week after imatinib therapy (74, 75). Recent developments in DWI may also provide new prognostic biomarkers and indicators of tumor response to targeted molecular therapy (76).
Contrast material–enhanced US was also suggested as a possibly biomarker of vascularization and in a study was found that decreased contrast material uptake at 7 and 14 days after treatment was correlated with good response of GISTs to imatinib (77).
Although effective in most patients with GIST, the development of resistance or intolerance to imatinib has been encountered. Such patients may experience clinical benefit from other molecular targeted therapy, as sunitinib and regorafenib (78). The clinical benefit rates of sunitinib and regorafenib using the different response to treatment criteria (RECIST or Choi) have been evaluated only in small cohorts of patients and should be validated using larger study cohorts (79, 80).
Treatment-related complications. Imaging may help in the early diagnosis of imatinib-related complications, such as bleeding into the gastrointestinal tract or intratumoral sites and fluid retention: pleural effusion, pulmonary edema, and ascites (81, 82). Other common abdominal toxicities related to molecular targeted therapies include hepatitis, cholecystitis, pancreatitis and infection (81). Radiologists should also be aware of intestinal complications associated with molecular targeted therapy, including pneumatosis, bowel perforation, and fistula formation (83).
Conclusion
Once considered an obscure tumor with poor prognosis, GISTs are nowadays recognized as the most common mesenchymal tumors of the alimentary tract and set as a new paradigm for cancer treatment. Imaging provides valuable information on detection, characterization, staging and prediction of treatment response of GISTs, contributing to optimization of patient management in all phases of treatment. Radiologists should be aware of all imaging issues related to GISTs, since a multidisciplinary team gathering different expertise is usually needed to properly treat patients with GISTs.
Footnotes
This article is freely accessible online.
Conflicts of Interest
None.
- Received March 20, 2016.
- Revision received April 26, 2016.
- Accepted April 27, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}