


Abstract
Background: Serum lactate dehydrogenase (LDH) has been reported as a prognostic biomarker in malignant diseases. However, little is known on the dynamics of serum LDH levels during systemic treatment. We focused on the association of changes in serum LDH with outcome of patients with advanced-stage non-small cell lung cancer (NSCLC) treated with erlotinib. Patients and Methods: Clinical data of 309 patients were analyzed. Serum samples were collected within one week before initiation and after one month of treatment. Results: The change in serum LDH during the first month of erlotinib treatment was independently associated with disease control rate (p=0.006), progression-free survival (PFS) (p=0.010) and overall survival (OS) (p<0.001). Conclusion: LDH is a commonly used serum biomarker, that is cheap and easy to detect. The results of our study suggest that the change in LDH serum level during the first month is a surrogate marker on the efficacy of erlotinib in patients with advanced NSCLC.
Lung cancer is one of the most common cancer-related causes of morbidity and mortality in developed countries and non-small cell lung cancer (NSCLC) accounts for approximately 80% of all lung cancer cases (1-3). Targeted therapy based on low-molecular weight tyrosine kinase inhibitors (TKI) directed at epidermal growth factor receptor (EGFR) represents one of the novel effective strategies in management of advanced-stage NSCLC. Erlotinib is a reversible EGFR-TKI that inhibits the EGFR tyrosine kinase by competing with adenosine triphosphate (ATP) at the ATP-binding site and prevents its phosphorylation and downstream signalling. Activating EGFR gene mutations, predominantly exon 19 deletions or the point-mutation in exon 21 termed L858R, are a strong predictive factor of response and survival to EGFR-TKIs (4, 5). On the other hand, the efficacy of EGFR-TKIs, particularly erlotinib, in the predominant patient group harbouring wild-type EGFR gene is low and there is no available predictive biomarker. In these patients, the use of erlotinib is still empirical without options for treatment personalisation. Early detection of EGFR-TKI activity could avoid toxicity and costs of inactive treatment, especially in the dominant group of patients harbouring the wild-type EGFR gene. High serum lactate dehydrogenase (LDH) levels have been reported as a poor prognostic biomarker in various malignant diseases, including NSCLC (6-12). In addition, high LDH protein expression also correlates with advanced stage and poor outcome (13-15). However, very little is known on the dynamics of serum LDH levels during the systemic treatment of patients with advanced-stage NSCLC. The aim of our retrospective study was to evaluate the association of changes in serum LDH with outcome in 309 patients with advanced-stage NSCLC treated with erlotinib.
Patients and Methods
Patients and treatment. We retrospectively analysed clinical data of 309 patients with cytologically or histologically confirmed locally advanced (IIIB) or metastatic stage (IV) NSCLC treated with erlotinib. Patients were treated between 2006 and 2014. Erlotinib was administered orally at the standard approved dose of 150 mg daily. The treatment was continued until disease progression or development of intolerable toxicity. Dose interruption or reduction was permitted in the event of treatment-related toxicity.
Data source. The clinical registry TULUNG (http://tulung.registry.cz/) is a non-interventional post-registration database of epidemiological and clinical data of patients with advanced-stage NSCLC treated with targeted therapies in the Czech Republic. The registry contains anonymised individual patient data, including demographic parameters, initial staging and disease characteristics, baseline patient information at the start of targeted therapy, as well as data on survival and adverse events. It is updated at least twice a year. Data on serum levels of LDH were extracted from the hospital information system and merged to the registry data. The protocol was approved by the independent ethics committee of the University Hospital Pilsen and complied with the International Ethical Guidelines for Biomedical Research Involving Human Subjects, Good Clinical Practice guidelines, the Declaration of Helsinki and local laws.
Clinical monitoring. The treatment was prospectively monitored and the clinical course of patients was continuously assessed at specific time points. Clinical follow-up, including physical examination, plain chest X-ray and routine laboratory tests was performed every 3-4 weeks; computed tomography (CT) was performed every two or three months of the treatment. The objective tumour response was assessed by the attending physician using Response Evaluation Criteria in Solid Tumours (RECIST) version 1.1 (16). The disease control rate (DCR) was calculated as the sum of complete responses (CR) + partial responses (PR) + disease stabilisations (SD) lasting for 6 weeks or more.
LDH measurement. Serum samples were collected and measurements were performed within one week before the initiation and after one month of erlotinib treatment. Serum LDH was measured using the International Federation of Clinical Chemistry (IFCC) method for spectrophotometric determination on an AU 2700 or AU 5800 (since 2014) Beckman Coulter analysers (Brea, CA, USA) (17). The measurements were performed in the central biochemical laboratory at the Department of Clinical Biochemistry and Haematology, Medical School and Teaching Hospital in Pilsen, using the cut-off value of 4.1 μkat/l.
EGFR mutation analysis. The tumour specimens acquired during initial bronchoscopy examination were evaluated by a senior cytologist using standard Giemsa staining. In some cases, a tumour biopsy was processed into formalin-fixed paraffin embedded (FFPE) histological sections. The cytology slides or the FFPE sections were submitted for molecular genetic testing, which included detection of somatic mutations in exon 19 (deletion) and 21 (L858R) of EGFR gene. If necessary, tumour cells were carefully selected and removed from the samples by laser microdissection using a P.A.L.M. microlaser instrument (Carl Zeiss MicroImaging GmbH, Jena, Germany). The microdissected cells were collected directly into the polymerase chain reaction (PCR) buffer and processed without a special DNA extraction step. In all other cases, the DNA was extracted from tissues by a standard spin column procedure using the JetQuick Tissue DNA Isolation Kit (Genomed GmbH, Loehne, Germany). Mutations were tested by Genoscan mutation detection kits (Genomac International, Prague, Czech Republic) utilizing a denaturing capillary electrophoresis (DCE) technique on an ABI PRISM 3100 16-capillary genetic analyser (Applied Biosystems, Foster City, CA, USA). Detected mutations were confirmed by Sanger DNA sequencing using BigDye v 3.0 chemistry (Applied Biosystems). In rare cases, where the overall fraction of mutated DNA was below the 20% threshold for DNA sequencing, a mutation was identified indirectly after forming a homoduplex fragment with a given known mutation reference standard.
Statistics. Standard summary statistics were used to describe the sample data set. The significance of differences in DCR was assessed using Fisher's exact test. Progression-free survival (PFS) and overall survival (OS) were estimated using Kaplan Meier method and all point estimates were accompanied by 95% confidence intervals (CI). PFS was defined from the date of erlotinib initiation until the date of first documented progression or death due to any cause. OS was defined from the date of erlotinib initiation until the date of death due to any cause. Patients who had not progressed or died were censored at the date of last follow-up. Statistical significance of the differences in Kaplan-Meier estimates was assessed using the log-rank test. Multivariable Cox proportional hazards model was used to quantify the influence of change in LDH on survival in the presence of other potential predictive and prognostic factors. As a level of statistical significance, alpha=0.05 was used.
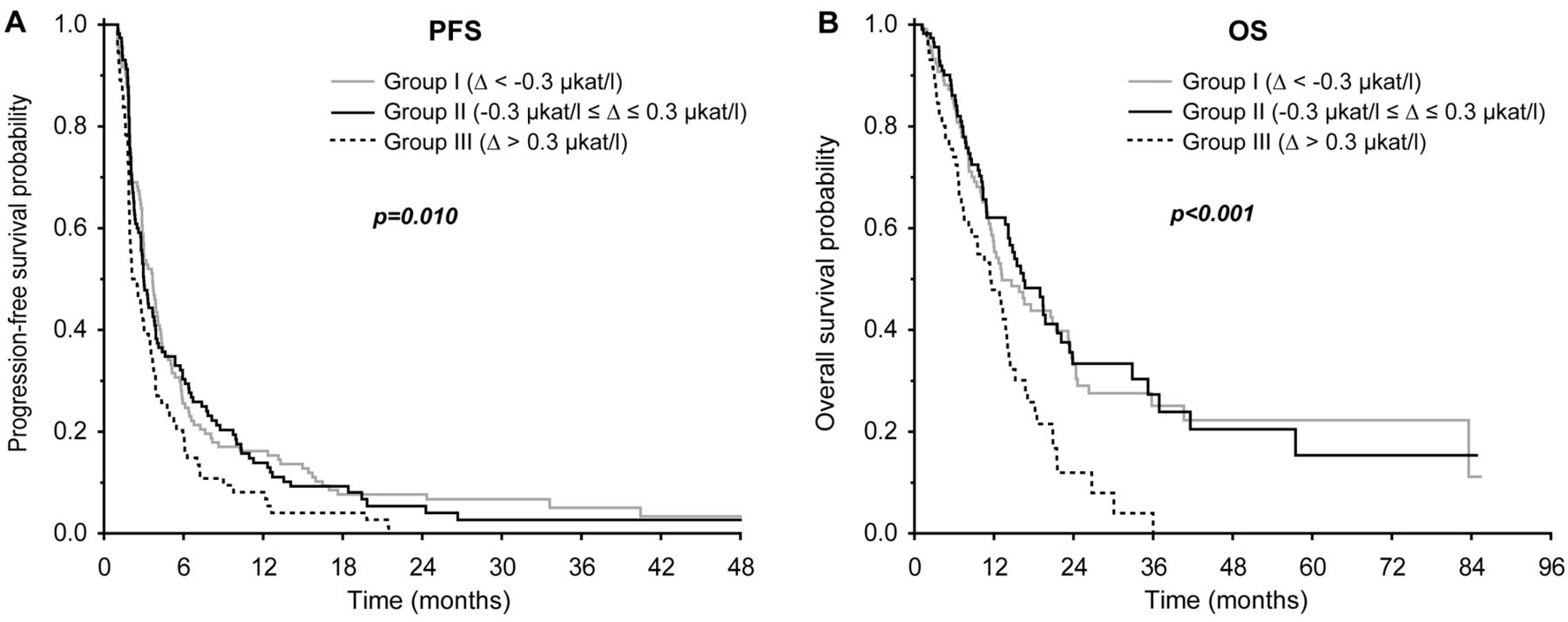
Absolute difference in LDH was defined as: Δ (delta)=value after one month of therapy - value at erlotinib therapy initiation, thus negative delta means decrease in LDH value and positive delta means increase in LDH value. We divided patients in three subgroups according to the change in time: Group I, Δ<−0.3 μkat/l=decrease in LDH; Group II, −0.3≤Δ ≤0.3 μkat/l=stable value; Group III, Δ>0.3 μkat/l=increase in LDH.
Results
Serum levels of LDH. The study included 309 patients. The baseline patient characteristics are summarized in Table I. Before treatment initiation, high baseline levels of LDH (≥4.1 μkat/l) were detected in 79 (25.6%) patients and normal levels of LDH (< 4.1 μkat/l) were detected in 230 (74.4%) patients. Group I (Δ<−0.3 μkat/l) included 120 (38.8%) patients, Group II (−0.3≤Δ≤0.3 μkat/l) included 115 (37.2%) patients and Group III (Δ>0.3 μkat/l) included 74 (23.9%) patients.
Association between change in serum LDH and erlotinib treatment efficacy. The median follow-up of the entire cohort was 10.4 months, with 186 (60.2%) deaths. The median follow-up in patients who were still alive at the time of evaluation (n=123; 39.8%) was 11.3 months. The median PFS of the entire cohort was 3.0 months (95% CI=2.6-3.4) and the median OS was 14.2 months (95% CI=12.2-16.2).
Baseline characteristics of patients.
The DCR for Group I was 86.7% (104/120), for Group II 85.2% (98/115) and for Group III 73.0% (54/74), respectively. The difference in DCR was statistically significant (p=0.006). The best objective treatment response data for Groups I-III are summarized in Table II. The median PFS was 3.7, 3.0 and 2.1 months for groups I, II and III, respectively (p=0.010). The median OS was 13.2, 16.4 and 11.4 months for groups I, II and III, respectively (p<0.001). The PFS and OS data are summarized in Table III and survival curves are shown in Figure 1.
Baseline clinical parameters were assessed together with change in LDH in univariate and multivariable models. The multivariable Cox proportional hazards model revealed that change in LDH serum level Δ>0.3 μkat/l (hazard ratio (HR)=1.55, p=0.006) and wild-type or unknown EGFR mutation status (HR=2.00, p=0.006) remain significant factors independently associated with short PFS, whereas change in LDH serum level Δ>0.3 μkat/l (HR=2.36, p<0.001), Eastern Cooperative Oncology Group Performance Status (ECOG PS) 2 or 3 (HR=1.37, p=0.048) and third- or higher-line of therapy (HR=2.35, p=0.009) remain significant factors independently associated with short OS (Table IV).
Discussion
LDH is widely expressed in cancer cells and is a common biomarker easily measurable in serum. It is a cytoplasmic enzyme reversibly catalyzing the conversion of pyruvate to lactate with concomitant inter-conversion of nicotinamide adenine dinucleotide (NAD) from oxidised to reduced form, the last step of glycolysis that permits the regeneration of NAD+, which is needed as an electron acceptor to maintain cytosolic glucose catabolism (18). There is a distinct metabolic difference between normal and cancer cells. Cancer cells utilize glycolysis for energy production, even under normoxic conditions, known as the “Warburg effect” (19). Therefore, most cancer cells are reliant on lactate production for their survival. This change of metabolism allows cancer cells to sustain higher proliferative rates. It has been previously suggested that the glycolytic fermentation pathway can produce intermediates for macromolecular synthesis needed for cell proliferation. This pathway can provide NADPH, a key element needed for macromolecular synthesis (20, 21) that is faster in ATP production compared to the respiration pathway; thus, the cells can keep up with the rate of cell proliferation (22). Nevertheless, hypoxia is a characteristic property in solid tumours, especially in tumour centre due to rapid division of tumour cells, high metabolic demands and tumour avascular area formation (23). Although it has been previously reported that high serum LDH levels are associated with poor prognosis in various malignancies, including NSCLC, there is still a lack of data on the potential role of dynamics of serum LDH levels in monitoring of treatment efficacy in advanced-stage cancer patients, in particular those with advanced-stage NSCLC treated with EGFR-TKIs (6-12).
Objective treatment response according to change in LDH serum level.
Progression-free (PFS) and overall survival (OS) according to change in LDH serum level.
Phase III randomised clinical trials proved the efficacy of erlotinib in the treatment of patients with advanced-stage NSCLC after failure of previous chemotherapy and also for first-line treatment of patients with tumours harbouring activating EGFR mutations (24-27). Several candidate biomarkers have been previously extensively studied but, apart from activating EGFR gene mutations, no reliable biochemical or molecular biomarker for prediction or early monitoring of erlotinib treatment efficacy has been validated. Therefore, biomarkers able to suggest early presence of benefit or resistance during the treatment with EGFR-TKIs would be very useful in clinical practice, especially in patients harbouring wild-type EGFR gene or for whom EGFR molecular profile is not available.
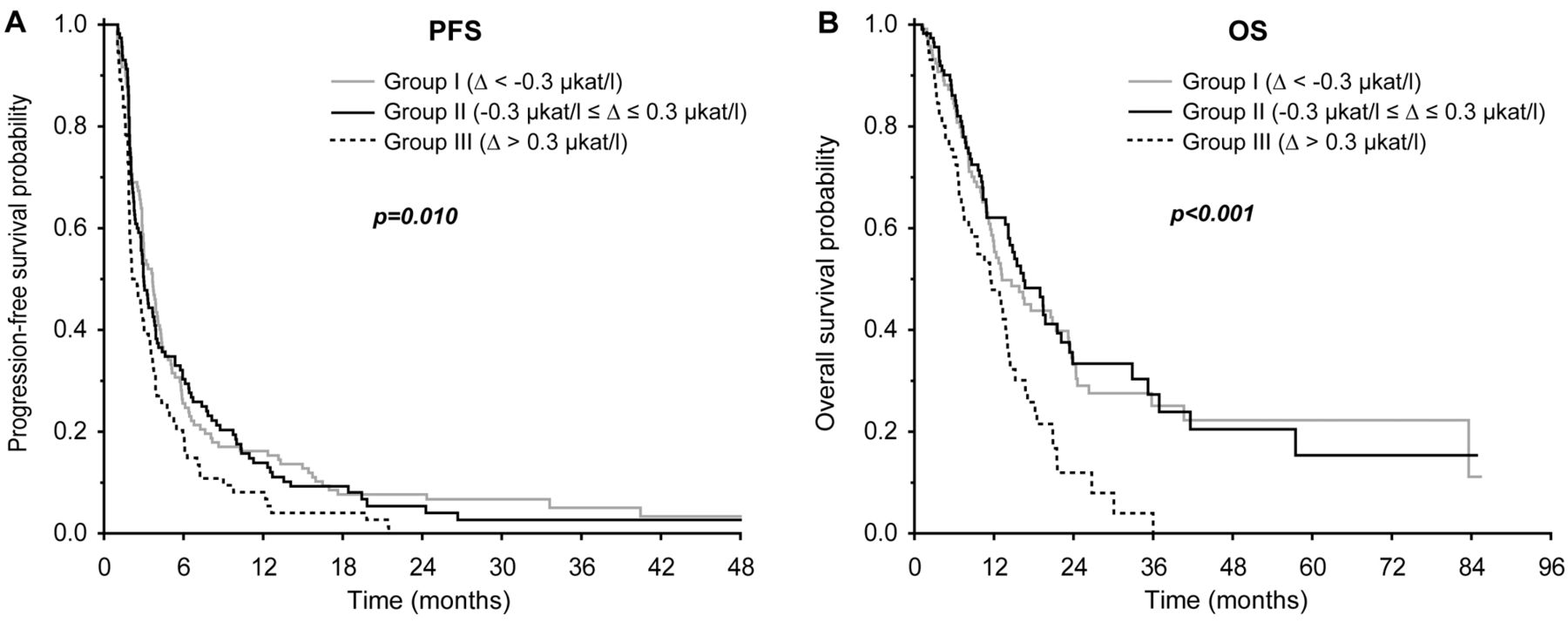
Kaplan-Meier plots showing progression-free (A) and overall (B) survival according to change in LDH serum level.
Multivariable Cox-proportional hazards model for progression-free and overall survival.
Thus, we focused on the association of change in serum LDH after one month of erlotinib treatment with outcome of patients with advanced-stage NSCLC. The present results suggest that early change in LDH may be predictive for the efficacy of erlotinib in NSCLC patients. Given the low DCR and poor survival for patients with increase in LDH serum level (Δ>0.3 μkat/l), early restaging –using clinical imaging–should be considered in these patients to identify disease progression, spare them unnecessary therapy with erlotinib and, perhaps, enable them to participate in high-risk population clinical trials.
Another promising option, to assess the early response to EGFR-TKIs using positron emission tomography (PET), has been recently demonstrated. Zander et al. reported that the change in standardized uptake value (SUV) of 18-fluorodeoxyglucose (FDG) uptake by PET after one week of erlotinib treatment was associated with response independently from EGFR mutational status (28). However this method appears more costly and less widely applicable compared to serum LDH measurement.
The principal limitations of the present study are its retrospective design and relatively small number of patients in the selected subgroups, as well as heterogeneity of the cohort. Nevertheless, it is the first study published so far to use LDH in the follow-up monitoring of erlotinib treatment efficacy in patients with advanced-stage NSCLC.
In conclusion, the results of the conducted retrospective study suggest that the change in LDH serum level during the first month of erlotinib treatment was independently associated with DCR, PFS and OS. LDH is a commonly used serum biomarker, which is easy and cheap to detect and, thus, appropriate for the use in routine clinical practice. Prospective studies on the role of serum LDH dynamics in the follow-up monitoring of advanced-stage NSCLC patients undergoing palliative treatment with EGFR-TKIs or chemotherapy should be performed to confirm these results.
Acknowledgements
The Authors would like to thank all patients voluntarily taking part in the observational, population-based registry TULUNG. This study is supported by Ministry of Health, Czech Republic - conceptual development of research organizations: Faculty Hospital in Pilsen - FNPl, 00669806 and Masaryk Memorial Cancer Institute - MMCI, 00209805; and by the National Sustainability Program I (NPU I) Nr. LO1503 provided by the Ministry of Education Youth and Sports of the Czech Republic.
Footnotes
Conflicts of Interest
JF has received honoraria from Astra Zeneca, Roche and Novartis for consultations and lectures unrelated to this project. TB has received honoraria from Roche for consultations and lectures unrelated to this project. AP has received honoraria from GSK, Roche and Bayer for consultations and lectures unrelated to this project. OF, MP, OT, JR, MS, RK, MM, LB, ZB and RC declare that they have no actual or potential conflict of interest, including any financial, personal or other relationships with other people or organizations that could inappropriately influence this work.
- Received February 20, 2016.
- Revision received April 2, 2016.
- Accepted April 4, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}