


Abstract
Background/Aim: By definition, tumor cells do not pass the epithelial basement membrane in pre-invasive lesions. However, recently, it was shown that hematogenous tumor cell dissemination already takes place in patients with ductal carcinoma in situ (DCIS), giving disseminated tumor cells (DTCs) in the bone marrow the opportunity to interact with the peripheral immune system. We, therefore, investigated the relationship between DTCs and the peripheral innate and adaptive immune system of DCIS patients, as immunosurveillance might also be impaired in pre-invasive lesions. Materials and Methods: We analyzed the peripheral immune status of 115 DCIS patients by flow cytometry. Results were correlated with presence of DTCs, that were detected in the bone marrow by immunocytochemistry (pan-cytokeratin antibody A45-B/B3) using the automated cellular imaging system (ACIS) according to the international society of hematotherapy and graft engineering (ISHAGE) evaluation criteria. Apoptotic DTCs were characterized by positive M30 staining and cytomorphological criteria. Results: In contrast to breast cancer, we found no significant correlation between appearance of DTCs and quantitative distribution of T-cell sub-populations, B and NK-cells neither in the bone marrow nor in the peripheral blood. Moreover, DTCs did not affect the expression of important immunomodulatory antigens for functional integrity of specific immune response such as, TCR-ζ, CD28 or CD95. Interestingly, 39% of DTCs were positive for M30 expression and showed cytomorphological signs of apoptosis. Conclusion: In contrast to breast cancer, DTCs of DCIS seem to be less immunogenic, which might result in a diverging way to evade immunosurveillance.
- Ductal carcinoma in situ
- breast cancer
- disseminated tumor cell
- immunosurveillance
- tumor cell dormancy
- tumor escape
- apoptosis
Abbreviations: BM, Bone marrow; CK, cytokeratin; DIN, ductal intraepithelial neoplasia; DCIS, ductal carcinoma in situ; DTC, disseminated tumor cell(s); PBL: peripheral blood lymphocyte; n.s., not significant; VNPI, Van Nuys Prognostic Index.
Ductal carcinoma in situ (DCIS) is the most frequent pre-invasive breast cancer. Over the past three decades, with introduction of screening mammography, its incidence has increased significantly (1). By definition, tumor cells do not pass the epithelial basement membrane in DCIS patients. However, recently, it was shown that tumor cell dissemination already takes place in patients with DCIS (2-5). Hüsemann et al. detected disseminated tumor cells in the bone marrow (DTCs) in 13 % of DCIS patients and Sänger et al. in 21% of their DCIS patients (2, 5).
Consequently, tumor cells that have passed the epithelial basement membrane may also have the opportunity to interact with the peripheral immune system. It is known, that invasive breast cancer patients present with T-cell impairment that extend tumor microenvironment; this is also seen in peripheral blood lymphocytes (PBLs) (6-10). Immunomodulatory antigens, such as CD28, an important ligand to the co-stimulatory molecule of the T-cell receptor, and TCR ζ-chain, an essential signal complex for T-cell activation and functional integrity of specific immune response, are down-regulated in primary breast cancer patients (6, 7). It was proposed that CD95L overexpression in breast cancer cells counter-selects tumor-specific (CD95-positive) T-cells and initiates apoptosis of the immune cells (11). Compared to healthy donors, a significant up-regulation of CD95 antigen could be found in peripheral T-cells of primary breast cancer patients (7).
Moreover, it was shown that there is a relationship between circulating tumor cells (CTCs) and peripheral T-cells in primary breast cancer patients (8). CTC-positive patients present with a significant increase of peripheral CD95(FAS)-positive T-helper cells (8). As tumor cells induce apoptosis of cells via the CD95/CD95L (ligand) pathway, this might lead to tumor cell escape by apoptotic T-helper cells and may open the door for tumor cell dormancy in the blood (8).
Furthermore, it was seen that DTCs significantly increase the proportion of natural killer cells (NK) and T-cells in the bone marrow, which led to the hypothesis that the immune system apparently tries to attack growing cancer in the patient (12).
In this context we investigated whether pre-invasive cancer, such as DCIS, also leads to hematogenous tumor cell dissemination with systemic influence on the peripheral innate and adaptive immune system.
Materials and Methods
Patients. After informed consent, 115 patients that were treated for their DCIS with primary operative therapy and bone marrow aspiration were recruited routinely from the Department of Obstetrics and Gynecology of the University Hospital of Tuebingen between January 2004 and December 2011. Bone marrow aspirates were analyzed for existence of DTC, expression of M30 (a marker for apoptosis) on DTC and distribution of lymphocyte subpopulations in bone marrow. Patients with a preexisting history of cancer, auto immune diseases or a disease of the hematological or lymphatic system were not included into the study. Retrospective analyses were approved by the local clinical ethical committee of the University of Tuebingen (502/2010A and 117/2011BO2) and research was carried out in compliance with the Helsinki Declaration.
Detection of DTC. Mononuclear cells were separated from bone marrow aspirates by density centrifugation with Biocoll (Biochrom, Berlin, Germany). After cytospinning on microscope slides (SuperFrost®, Langenbrinck, Germany) epithelial tumor cells were detected by immunochemical staining with anti-cytokeratin (CK)-antibody A45B/B3 against CK8, CK18 and CK19 (Micromet AG, München, Germany) using an autostainer and detection kit (Dako REALTM Detection System APAAP, Aachen, Germany) according to the manufacturer's instructions. Two slides with 2×106 cells were analyzed per patient by an automated cellular imaging system ((ACIS); ChromaVision Medical Systems, San Juan Capistrano, CA, USA). Details of this system have been described elsewhere (13). DTC were analyzed based on recommendations of the European ISHAGE Working group for standardization of tumor cell detection and the consensus statements (14, 15).
From DTC-positive patients, additional slides were stained using the M30 antibody (Roche Applied Science, Mannheim, Germany) and the APAAP kit detection. The antibody reacts with a neo-epitope expressed only after caspase cleavage of cytokeratin 18 during early apoptosis (6, 17). Identification of apoptotic tumor cells was based on positive M30-staining and on cytomorphological criteria, as described elsewhere (18-21).
Analysis of lymphocyte sub-populations. Not later than five hours after collection, samples of 100 μl bone marrow and peripheral blood were stained with 10 μl conjugated mouse anti-human monoclonal antibodies, CD3-PerCP, CD4-APC, CD8-APC, CD19-PerCP, CD20-APC, CD95-FITC, Simultest CD3/16+56+ FITC (Becton Dickinson, Heidelberg, Germany), CD28-RPE (Biozol, Echingen, Germany) and CD56-RPE (Dako, Hamburg, Germany). After incubation, 0.5 ml FACS-Lyse-Reagent (Becton Dickinson, Heidelberg, Germany) was used to lyse erythrocytes and thrombocytes. Peripheral blood mononuclear cells were recovered and washed with 500 μl CellWASH™ (Becton Dickinson). To detect intracellular antigens, cells had to be permeabilized with 10 μl/ml Digitonin Working Solution (Sigma-Aldrich, Munich, Germany) before staining with 10 μl TCR-zeta FITC antibodies (Biozol). After incubation with the antibodies for up to 60 min on ice, samples were washed twice with CellWASH™ and fixed with 0.5% paraformaldehyde. Afterwards, viable cells were detected by three-color flow cytometry using a FACSCalibur™ with Cell Quest Pro® software (Becton Dickinson). At least 20,000 events were recorded per sample and data were visualized as dot plots.
Statistical analysis. Absolute numbers of lymphocyte subpopulations were compared. Means and standard deviations were calculated with SPSS Statistics (IBM, version 20). A Mann-Whitney-U-test for nonparametric, independent data was used to test for statistical correlation between the detection of DTC in patients with DCIS and distribution of lymphocyte subpopulations in their bone marrow and peripheral blood. p-Values <0.05 were considered to be significant.
Results
Patients' characteristics. One hundred and fifteen patients with pure DCIS were included in the study. In 52 patients (group 1) appearance of DTCs was correlated with quantitative distribution of T-, B-, NK cells in the bone marrow (BM). Among this group, 16 patients (31%) were DTC-positive and 36 patients (69%) were DTC-negative. Clinicopathological data are summarized in Table I.
Forty percent of tumors were ≤15 mm, 36% were between 16 and 40 mm and 23% measured >41 mm (group 1; Table I). With regard to grading, 46% presented with ductal intraepithelial neoplasia (DIN) grade 3, 44% with DIN 2 and 10% with DIN 1c. A fair number (77%) of the tumors were estrogen receptor (ER)-positive and 79% were progesterone receptor (PR)-positive in this group.
In 63 patients (group 2), appearance of DTCs was correlated with quantitative distribution of T-, B-, NK cells in the peripheral blood (PB) (group 2; Table I). Almost one-fifth (19%) of these patients were DTC-positive and 81% were DTC-negative. In 25%, tumor size amounted ≤15 mm, 44% were between 16 and 40 mm and 30% were >41%. With regard to grading, the majority of patients presented with DIN 3 (54%) and DIN 2 (36%), followed by 9% with DIN1c. Sixty-eight percent of the tumors were ER-positive and 70% showed PR-positivity (group 2, Table I).
There was no significant difference between group 1 and group 2 related to grading, tumor size, hormone receptor status, Van Nuys Prognostic Index, menopausal status (data not shown).
Correlation of DTCs with quantitative distribution of BM T-, B- and NK-cells in DCIS patients. Appearance of DTCs in DCIS patients had no significant correlation with the quantitative distribution of T-, B- and NK-cells in the bone marrow (Table II). Concerning the BM T-cell sub-populations we found similar numbers of CD3+/CD8+ cells/μl (p=0.5) and CD3+/CD4+ cells/μl (p=0.4) in DTC-positive and DTC-negative patients. Also, CD19+/CD20+ cells/μl did not significantly differ with appearance of DTCs (p=0.5). Absolute number of CD3−/CD16+/CD56+ cells/μl in the bone marrow was reduced in DTC-positive patients, but not significantly (p=0.5).
Presence of DTCs did not affect expression of CD 28 and TCR-ζ antigen in cytotoxic specific T-cell population in the bone marrow. Moreover, regulation of CD95 (FAS) expression in CD3+/CD8+ and CD3+/CD4+ T-cells population did not correlate with appearance of DTCs in patients. Quantitative distribution of PB T-, B- and NK-cells in DCIS patients with and without DTCs. DTCs showed no significant effect on the quantitative distribution of peripheral blood T-cells (Table III). Patients with DTCs had a higher number of CD3+/CD4+cells/μl compared to patients without DTCs (p=0.8). Concerning cytotoxic T-cells, we found a similar number of CD3+/CD8+cells/μl in DTC-positive and DTC-negative cases (p=0.7).
CD19+/CD20+ cells/μl and CD3−/CD16+/CD56+ cells/μl population in peripheral blood were not significantly associated with the number of DTCs and did not differ in DTC-positive and DTC-negative patients. Expression of CD28 and TCR-ζ on peripheral T-cytotoxic and T-helper cells were not regulated by presence of DTCs and expression of CD95 (FAS) antigen on CD3+ cells was also not significantly influenced by DTCs (p=0.6).
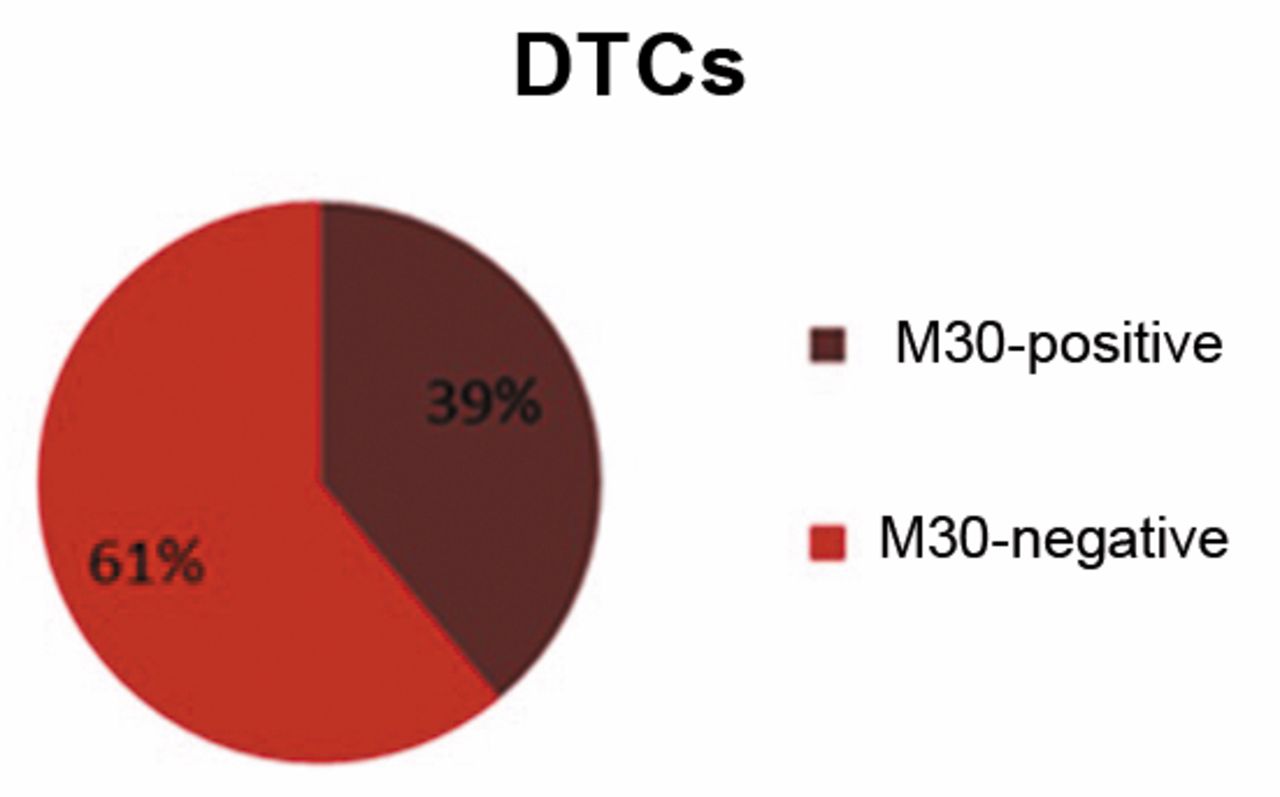
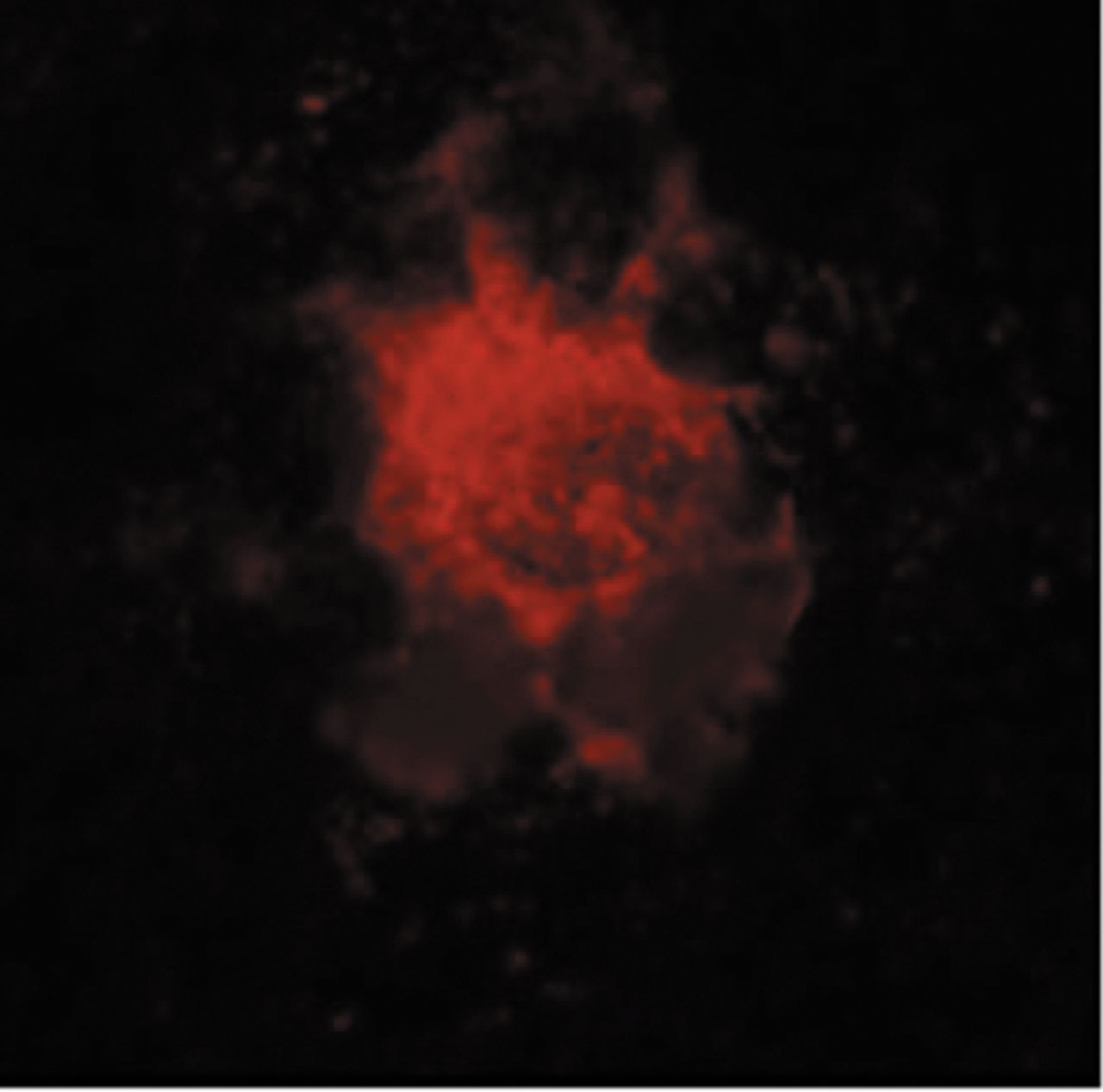
Expression of M30 on DTC. A sample of 46 DTC-positive patients was evaluated for expression of M30, a neo-epitope expressed only after caspase cleavage of cytokeratin 18 during early apoptosis. Thirty-nine percent (n=18) were found to have DTCs expressing M30 and cytomorphological criteria for apoptosis (Figure 1). An example of a DTC stained for M30 seen with Texas Red filter in 1000× magnification is shown in Figure 2.
Discussion
Tumor cell dissemination in DCIS patients. By definition, DCIS is a pre-invasive breast cancer from clonal proliferation of ductal epithelial cells, which does not grow beyond the basement membrane. Mokbel et al. and Tsikitis et al. postulated that these pre-invasive lesions cannot shed tumor cells since they are restricted to the epithelial layer and do not come in contact with blood or lymphatic vessels (22, 23). However, it was recently discovered that tumor cell dissemination is not only restricted to invasive breast cancer but is also seen in DCIS patients (3, 5). Tumor cells passing the basement membrane in early epithelial lesions of the breast were detected by electron microscopy (3, 5). Therefore, Hüsemann et al. proposed the hypothesis that the first step of metastasis takes already place in early lesions of the breast-like DCIS (5), which can be confirmed by the observation that up to 3 % of patients with pure DCIS present already with axillary lymph node metastasis (24). Our results also support this hypothesis. In 28 of the 115 analyzed DCIS patients (24%), we detected tumor cell dissemination in the bone marrow. These findings are in accordance to other studies. Banys et al. found DTCs in 16% (25), Sänger et al. in 21% (2) and Hüsemann et al. in 13% of analyzed patients with pure DCIS (5). In primary breast cancer, DTCs are found in 20-40% of cases and are strongly associated with poor clinical outcome (26). It is known that, years after diagnosis, persistent dormant disseminated tumor cells may change into an active state and initiate metastatic spread. The mechanisms initiating disease progression are not fully understood. There exists evidence that immunological factors trigger tumor escape (27-29) and immunosurveillance against micrometastasis might be affected by functional impairment of T-cells, which extent tumor microenvironment, also seen in peripheral blood and bone marrow (7, 8, 12, 30).
Clinicopathological characteristics of patients with DCIS included in this study.
Lymphocyte sub-populations in bone marrow of DCIS patients with and without DTCs.
Lymphocyte sub-populations in peripheral blood of DCIS patients with and without DTCs.
Relationship between DTC and cellular immunity in DCIS patients. The concept of immunological surveillance includes the immune system's ability to recognize and eliminate tumor cells (31). As soon as disseminated tumor cells have reached blood and/or lymphatic vessels, interaction with peripheral immune cells is possible. Recent studies have shown, that the peripheral immune system of primary breast cancer patients is compromised (7, 12, 32-34). Breast cancer patients present with less T-lymphocytes, T-helper cells and cytotoxic T-lymphocytes than healthy donors in their bone marrow (12, 32, 33) and in their blood (34). Moreover, there is a relationship between circulating tumor cells (CTCs) and peripheral T-cells in primary breast cancer patients as CTC-positive patients present with a significant increase of peripheral CD95(FAS)-positive T-helper cells (8). In this context, it is of special interest how DTCs affect cellular immunity of DCIS patients.

Expression of M30 on DTCs.
In our study the existence of DTCs did not show any significant influence on the quantitative distribution of T-lymphocytes, T-helper cells, cytotoxic T-cells, NK-cells or B-lymphocytes neither in bone marrow nor in peripheral blood of DCIS patients. Although no change was seen in absolute numbers of lymphocytes, a functional impairment of lymphocytes may also lead to ineffective immunological surveillance. Therefore, the expression of immunomodulatory antigens, such as CD28, TCR ζ-chain and CD95 on lymphocytes, in correlation to existence of DTC, was analyzed. Interestingly, we could not find any association between presence of DTCs and influence on the expression of CD28, TCR ζ-chain and CD95 antigen on T-cells in the bone marrow or peripheral blood of DCIS patients.
These findings are contrary to studies on patients with invasive breast cancer where the activation of T-lymphocytes via co-stimulation with CD28 and intracellular signal transduction via TCR ζ-chain were found to be disturbed (6-9). Moreover, CD95 is up-regulated in cytotoxic T-cells of primary breast cancer patients (7) and, therefore, might be susceptible to apoptosis via the CD95/CD95L (ligand) pathway. Depending on presence of hematogenous tumor cell dissemination in the bone marrow, primary breast cancer patients are presented with an increased proportion of BM natural killer cells (NK) and T-cells (12). Moreover, circulating tumor cells affected peripheral T-helper cells by up-regulation of CD95 antigen (8).
Evidence of M30 expression on DTC in DCIS patients. Since we did not observe any difference in cellular immunity of DCIS patients dependent on hematogenous tumor cells dissemination, the question raised was if DTCs of DCIS patients might have less immunogenity than DTCs of primary breast cancer patients. Therefore, expression of M30, a neo-epitope expressed only during early apoptosis (16, 17), was analyzed on DTCs. Apoptotic DTCs were found in 39% of the examined patients. Thus, DTCs appear as a heterogeneous population of apoptotic and non-apoptotic cells. The presence of apoptotic DTCs seems to be higher in DCIS patients than in patients with primary breast cancer. Even after neoadjuvant systemic therapy, Fehm et al. only described 23% and Hartkopf et al. 29% of M30-expressing DTCs (35, 36).
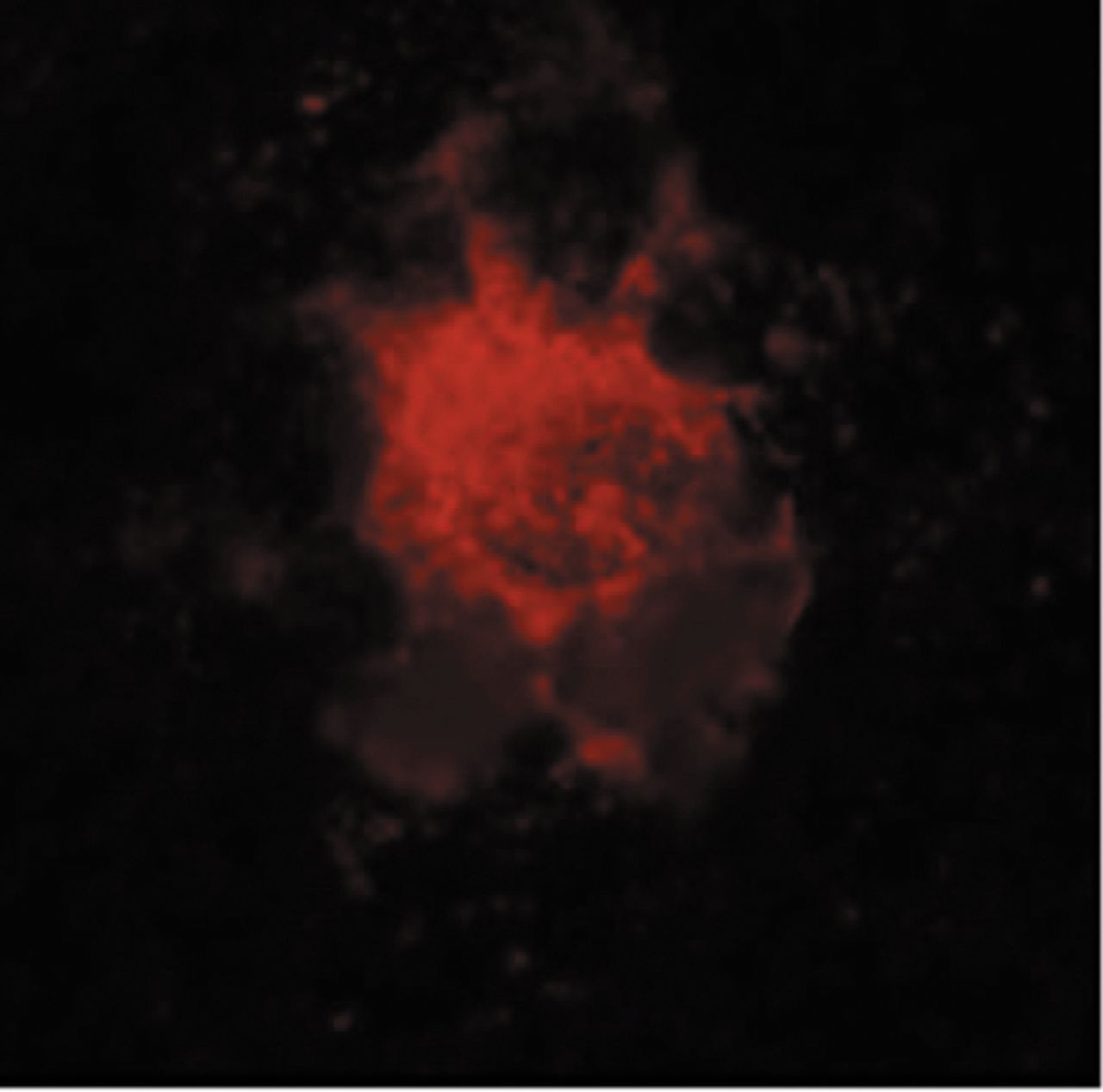
DTC-expressing M30 in 1,000× magnification seen with Texas Red filter.
Conclusion
Hematogenous tumor cell dissemination already takes place in DCIS patients. In contrast to breast cancer, DTCs of DCIS patients seem to have no effect on the peripheral cellular immune system and, therefore, seem to be less immunogenic. This impaired immunogenity may be caused by DTCs being in the state of tumor cell dormancy and/or DTCs being apoptotic. Regarding this point, we observed DTCs to be apoptotic in 39% of our DCIS patients. These findings raise the question if DTCs in DCIS might differ from DTCs in breast cancer by diverging ways to evade immunosurveillance. Further ongoing studies on DCIS patients will contribute to investigate the mechanism(s) of tumor escapement by DTCs.
Acknowledgements
All Authors who are funded by the Department of Obstetrics and Gynecology, University of Tuebingen, Germany, thank Angelika Amann, Ingrid Teufel and Silke Dürr-Störzer in data acquisition.
Footnotes
↵* These Authors contributed equally to this article.
Competing Interests
The Authors declare that they have no conflicts of interests.
- Received February 15, 2016.
- Revision received April 8, 2016.
- Accepted April 11, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}