


Abstract
Aim: To compare three total radiation dose levels for their impact on survival in patients receiving palliative radiotherapy (RT) for locally advanced lung cancer. Patients and Methods: Radiation dose (equivalent dose in 2 Gy fractions=EQD2: 31-40 Gy vs. 41-46 Gy vs. 47-52 Gy), completion of RT as planned, plus nine factors were analyzed for survival in 125 patients. Results: On multivariate analysis, EQD2 47-52 Gy (p=0.018), completion of planned RT (p=0.002), lower T-category (p=0.027) and lower N-category (p=0.008) were positively associated with survival. Thirty-six patients (29%) could not receive the complete planned RT dose, 19% in the 31-40 Gy group, 36% in the 41-46 Gy group and 31% in the 47-52 Gy group, respectively. Six-month survival rates of these patients were 0%, 18% and 18%, respectively. Conclusion: Higher RT doses resulted in significantly better survival than lower doses. The favorable results were impaired when the planned treatment could not be completed.
Lung cancer is one of the most common cancer types worldwide (1). Many patients experience symptoms such as thoracic pain, dyspnea and tumor bleeding. In most of these patients, thoracic surgery cannot be reasonably performed. Palliative radiation therapy (RT) was shown to be effective in controlling and preventing symptoms caused by locally advanced lung cancer (2-4). However, the optimum dose remains unclear. Contradictory data particularly exist with respect to the impact of the total radiation dose on survival in these patients. Some trials demonstrated that higher doses led to improved survival, whereas other trials did not find such a dose-effect relationship (5-11). Thus, greater investigation is required before this question can be answered. The present study compared three groups based on their different dose of treatment and analyzed the impact on survival in patients receiving palliative RT for locally advanced lung cancer. Furthermore, the importance of completing the planned treatment was investigated.
Patients and Methods
The radiation dose (equivalent dose in 2 Gy fractions=EQD2: 31-40 Gy vs. 41-46 Gy vs. 47-52 Gy), completion of RT as planned (no vs. yes) and nine additional factors were retrospectively evaluated for survival in 125 patients receiving palliative RT for advanced lung cancer (stage III/IV). The additional factors were age (≤70 years vs. ≥71 years; median=71 years), gender, tumor site (peripheral vs. central), tumor histology (adeno-carcinoma vs. squamous cell carcinoma vs. anaplastic carcinoma vs. small cell lung cancer), primary tumor stage (T-stage: T1-2 vs. T3-4), lymph node stage (N-stage: N0-1 vs. N2-3), distant metastases (no vs. yes), Karnofsky performance score (≥70 vs. ≤60), and history of smoking (no vs. yes). The EQD2 was calculated with the equation: EQD2=TD x (DFx + α/β/2 Gy + α/β) (TD=total dose of RT; DFx=dose per fraction; α/β=10 Gy for tumor cell kill) (12).
RT was delivered after 3D-treatment planning with 6-18 MV photon beams from a linear accelerator. Margins were 6-8mm between GTV and CTV and 8mm between CTV and PTV, respectively. Total dose tanged between 30 Gy and 50 Gy (median: 39 Gy), and doses per fraction between 2.0 Gy and 4.0 Gy (median: 3.0 Gy). Doses were prescribed according to recommendations of the International Commission of Radiation Units and Measurements (ICRU) (dose to PTV=95-107% of the prescribed dose).
The univariate analysis of survival was performed with the Kaplan-Meier method and the log-rank test. The factors that achieved significance in the univariate analysis (p<0.05) were further analyzed for independence with the Cox proportional hazards model.
Survival rates at 6 months and 1 year after radiation therapy (univariate analysis).
Results
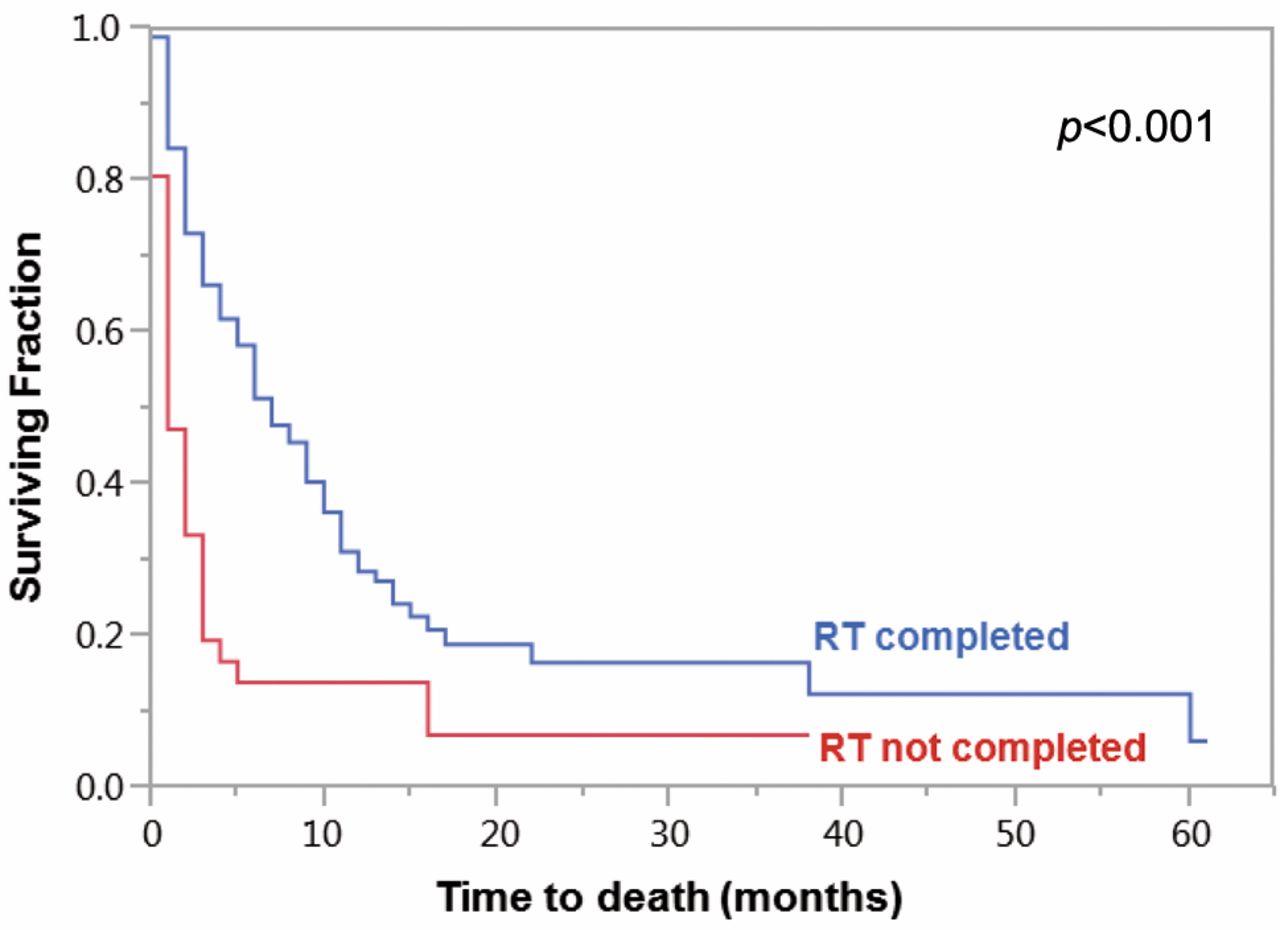
Patients were followed until death or for a median of 13 months (range: 4-61 months) in those alive at their last follow-up. Six-month and 1-year survival rates were 41% and 24%, respectively, in the entire series. Univariate analysis revealed significant positive associations with survival for an EQD2 of 47-52 Gy (p=0.031, Figure 1), completion of the planned RT (p<0.001, Figure 2), peripheral location of the tumor (p=0.017), lower T-category (p=0.002), lower N-category (p<0.001), absence of distant metastases (p=0.027) and no history of smoking (p=0.024). Results of the univariate analysis are shown in Table I.
Multivariate analysis (Cox proportional hazards model) of survival.
In the Cox proportional hazards model, the EQD2 (p=0.018), completion of the planned RT (p=0.002), T-category (p=0.027) and N-category (p=0.008) were still significant, whereas tumor location (p=0.68), distant metastases (p=0.20) and history of smoking (p=0.13) were not. The entire results of the multivariate analysis including the risk ratios and the 95%-confidence intervals are shown in Table II.
Due to acute decrease in performance status or acute treatment toxicity, 36 patients (29%) could not receive the complete RT dose as planned, 8 patients (19%) from the 31-40 Gy group, 17 patients (36%) from the 41-46 Gy group and 11 patients (31%) from the 47-52 Gy group, respectively. The 6-month survival rates of these patients were 0%, 18% and 18%, respectively, and the 1-year survival rates were 0%, 13% and 10%, respectively.
Discussion
Many patients with locally advanced lung cancer present with poor overall health and will likely not tolerate an aggressive treatment approach such as 60-70 Gy of RT plus concurrent chemotherapy. Instead of cure of the malignant disease, the main indication of RT is the control or prevention of debilitating symptoms including pain, dyspnea and bleeding (13, 14). For these patients, several dose-fractionation regimens are available. The most appropriate dose needs to be further defined. One important question is whether one can achieve better symptom control with higher doses of RT compared to lower doses. In their systematic review, Fairchild et al. concluded that lower-dose RT was comparable to higher-dose RT with respect to symptom control but inferior with respect to the total symptom score (4). Any improvement with respect to the total symptom score was found in 65.4% (216/330) of patients after lower-dose RT and 77.1% (243/315) of patients after higher-dose RT, respectively (p=0.003). In the practice guideline of Rodrigues et al., higher-dose RT defined as 10×3 Gy or greater was associated with modest improvements in total symptom score (3).
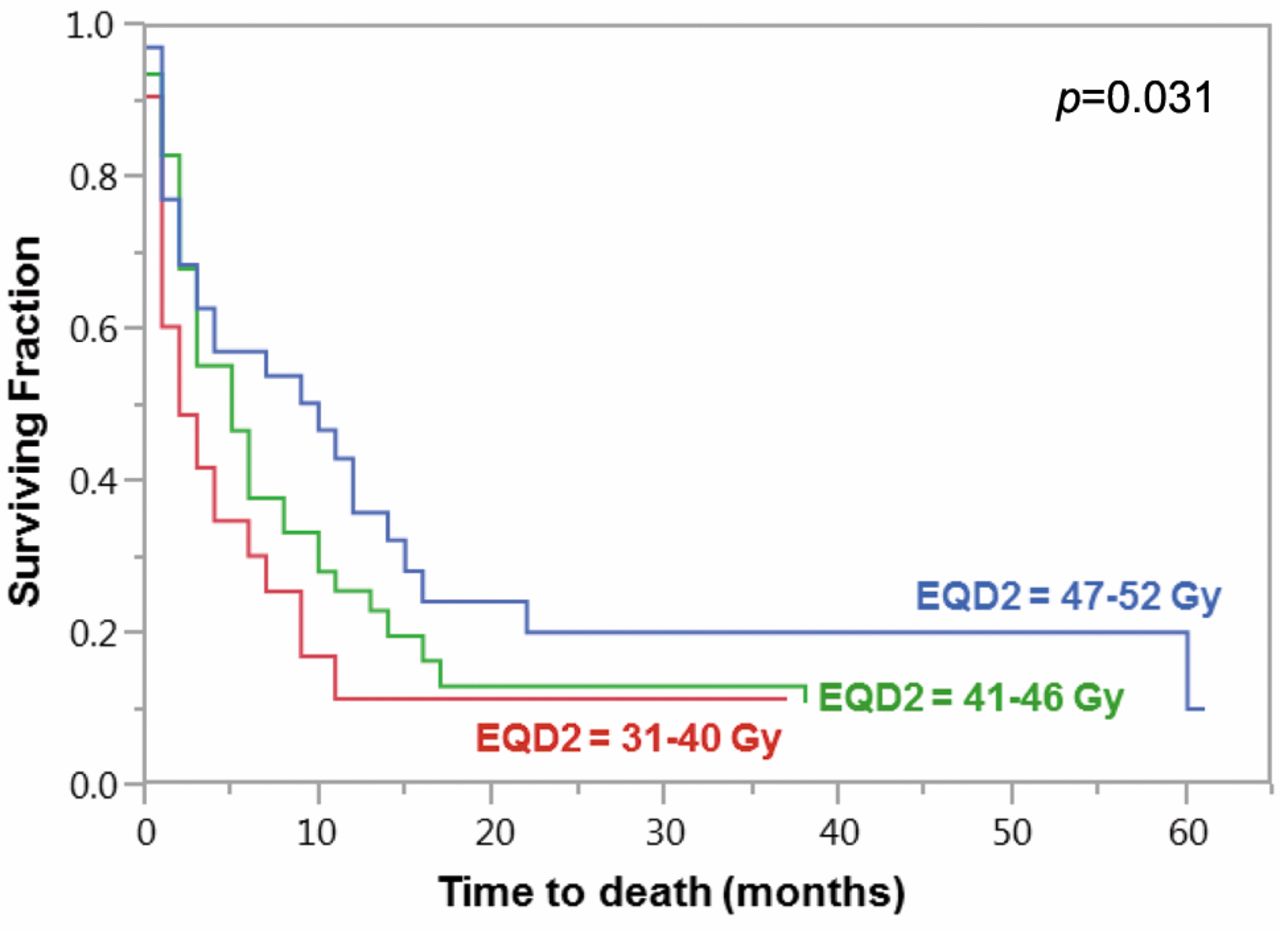
Kaplan-Meier curves of the dose groups 31-40 Gy, 41-46 Gy and 47-52 Gy.
Besides symptom control, survival is another important end-point in the palliative RT of locally advanced lung cancer. Three trials demonstrated that higher doses of RT improve survival in patients irradiated with palliative intention for locally advanced lung cancer (7, 9, 11). In the randomized trial of the Medical Research Council Lung Cancer Working Party (United Kingdom), 13×3 Gy (EQD2: 42.3 Gy) resulted in significantly better survival than 2×8.5 Gy (EQD2: 26.2 Gy) (11). Median survival times were 9 months and 7 months, respectively (p<0.05). In a randomized trial from Canada, 5×4 Gy (EQD2: 23.3 Gy) led to longer median survival than 1x10 Gy (EQD2: 16.7 Gy), 6.0 vs. 4.2 months, p=0.031) (9). In another trial from the Netherlands, survival after 10×3 Gy (EQD2: 32.5 Gy) was significantly better than after 2×8 Gy (EQD2: 24.0 Gy). One-year survival rates were 20% and 11%, respectively (p=0.03) (7). In contrast, some trials did not find a significant improvement of survival with the administration of higher-dose RT rather than lower-dose RT. The randomized trial of Jeremic et al. compared 13×3 Gy (EQD2: 42.3 Gy) to 2x8 Gy (EQD2: 24.0 Gy) and 1×10 Gy (EQD2: 16.7 Gy). RT in the lower-dose group was supplemented by upfront platinum-based chemotherapy (5). Median survival times were 7.1 and 8.1 months, respectively (p=0.40). In the trial of Erridge et al., median survival times were 23 weeks after 1×10 Gy (EQD2: 16.7 Gy) and 28 weeks after 10×3 Gy (EQD2: 32.5 Gy), respectively (p=0.20) (6). In the three-arm trial of Sundstrøm et al., median survival times after 2×8.5 Gy (EQD2: 26.2 Gy), after 15×2.8 Gy (EQD2: 44.8 Gy) and 25×2 Gy (EQD2: 50 Gy) were 8.2, 7.0 and 6.8 months, respectively (p>0.05) (8). In an additional randomized trial from Poland, 2×8 Gy (EQD2: 24.0 Gy) resulted in a longer median survival time than 5×4 Gy (EQD2: 23.3 Gy), 8.0 vs. 5.3 months (p=0.016) (15).

Kaplan-Meier curves of the patients with and those without completion of RT as planned.
Due to these contradictory results regarding impact of the RT dose on survival, we performed an additional study that compared three dose levels and additionally investigated the importance of completing the planned RT program. The results of this study strongly suggested a dose-effect relationship. The group of patients who received the highest doses (EQD2: 47-52 Gy) had the best survival, followed by the intermediate dose group (EQD2: 41-46 Gy) and the lower-dose group (EQD2: 31-40 Gy). When compared to most previous studies, the EQD2s administered in the present study were higher (6, 7, 9, 11). This may explain why 36% of the patients in the intermediate dose group and 31% of the patients in the higher dose group did not receive the complete planned doses. Of these patients, only 18% survived for one year or longer. In comparison, 48% of the patients who received the complete planned RT dose in the higher-dose group survived for at least one year. This finding demonstrates that it is very important to select patients for higher-dose RT, who are more likely to receive the complete planned treatment, preferably those patients with a more favorable performance status and comparatively little comorbidity.
When selected for higher-dose RT, these patients require close monitoring during the course of RT and timely supportive care to treat any radiation-induced toxicity as soon as possible. One main objective is to avoid premature discontinuation of RT. Also interruptions of the RT course may have a negative impact on the patients' outcomes such as survival (16). Selected patients may also be considered for the addition of concurrent or sequential chemotherapy or modern targeted therapies (17-19). However, these additional systemic treatments must be adapted to the patient's palliative situation, where the intention of the treatment is generally symptom relief and not cure. The main limitation of this study was the retrospective nature of the analysis that may have introduced uncontrolled biases. However, the findings are consistent with those of other investigators and may supplement their findings with a greater range of doses analyzed (7, 9, 11).
In conclusion, the present study suggested that higher RT doses used for the treatment of locally advanced lung cancer resulted in significantly better survival than lower doses. The favorable results of higher doses were impaired when the planned treatment could not be completed. Thus, proper patient selection before RT, close monitoring, and timely supportive care during RT are mandatory.
Footnotes
Conflicts of Interest
On behalf of all Authors, the corresponding Author states that there are no conflicts of interest related to this study.
- Received January 20, 2016.
- Revision received February 24, 2016.
- Accepted February 25, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Feasibility and safety of shortened hypofractionated high dose palliative lung radiotherapy - A retrospective planning study
- How Should Palliative Thoracic Radiotherapy Be Fractionated for Octogenarians with Lung Cancer?
- Validation of a Score Developed to Estimate the 6-month Survival of Patients Treated with Palliative Local Radiotherapy for Advanced Lung Cancer