


Abstract
Background/Aim: Evaluations of efficacy of treatment modality in analyses on patients with acute myeloid leukemia (AML) often combine chemotherapy and stem cell transplantation (SCT). To account for the effect of SCT and determine the impact of chemotherapy alone, the National Cancer Data Base from 1998-2011 was analyzed. Patients and Methods: Patients with AML from 1998-2011 aged 18-64 years were included. Chi-square analysis was used to assess the association between treatment and factors investigated. The Kaplan–Meier method was used to assess overall survival. Log-rank methods were used to determine factors significant for survival. Multivariable Cox regression analysis was used to determine the effect of chemotherapy alone, and both chemotherapy and SCT on survival while adjusting for other variables. Results: A total of 34,816 patients from the National Cancer Database were eligible for this study. Eighty-four percent of patients received chemotherapy alone, 8.3% no chemotherapy or SCT, and 7.5 % received both chemotherapy and SCT. Five-year survival for patients without chemotherapy without SCT was 12%, survival for the group treated with chemotherapy alone was 37.8% and for those receiving both chemotherapy and SCT was 44.1%. Treatment with chemotherapy only and chemotherapy plus SCT had a hazard ratio for death of 0.42 and 0.35 compared to no chemotherapy or SCT. Advanced age, male sex, Black race, diagnosis prior to 2004, multiple comorbidities, Medicare insurance, Medicaid insurance, no insurance, lower income and low education level, distance less than 30 miles from treatment Center, diagnosis and treatment at same facility, were independently associated with worse survival. Conclusion: Survival analysis of AML in the National Cancer Database showed multiple factors to be independently associated with survival. Outcomes based on treatment suggest an improved survival when utilizing chemotherapy and SCT as the primary treatment modality.
The American Cancer Society estimated there were approximately 20,830 new cases and 10,460 deaths from acute myeloid leukemia (AML) in 2015 (1). AML is generally a disease of older people and uncommon before the age of 45 years. In 2008, the World Health Organization revised the classification of AML for proper prognostication based on morphology, immunophenotyping, cytogenetic data and molecular studies (2, 3). The risk of dying for AML can be divided into high, intermediate and low risk (4-7). Per SEER data analysis, the 5-year survival of patients with AML has improved over recent decades (8). There are many risk factors associated with survival in patients with AML. Well-known risk factors that are associated with poor survival include advanced age, poor performance status, unfavorable prognostic abnormalities, as well as treatment intensity (9). Other factors that could affect survival include type of treatment as well as other patient characteristics, and socioeconomic factors.
Many studies have uncovered a positive correlation between uninsured and underinsured payer status with mortality from cancer (10-15). As healthcare reform in the United States continues to evolve, defining the impact of payer status on health outcomes remains challenging. In the wake of the Affordable Care Act, many expect the shift in insurance coverage across the United States to continue (16-20). The effect that this shift will have on survival of patients with cancer is uncertain.
The 5-year survival rates have increased from 6.3% in 1975 to 23.9% in 2007 per SEER data analysis. Overall survival rates for AML decrease with increasing age (21). The complete remission rate in older adults with AML rags between 40% and 60% (22-31). Older adults are more likely to have comorbidities and a poorer performance status, two factors associated with treatment-related morbidity and mortality, and which limit intensive treatments such as allogenic hematopoietic cell transplantation (9). The common factors on which initial treatment of AML is based are age, history of myelodysplasia, cytotoxic chemotherapy, and performance status. Standard induction regimes used for patients less than 60 years old include the backbone of cytarabine and anthracycline (9).
National Comprehensive Cancer Network (NCCN) guidelines recommend stem cell transplant (SCT) for intermediate- to poor-risk patients with AML who are less than 60 years old (9). The current study utilized a large dataset from the National Cancer Database (NCDB) to assess factors associated with improved survival for AML, adjusting for SCT, as well as the chemotherapy modality.
Materials and Methods
The NCDB is a hospital-based cancer registry that is jointly maintained by the American College of Surgeons and the American Cancer Society. The NCDB captures approximately 70% of all newly diagnosed cases of cancer in the United States (32). The database standardizes data elements for patient demographics, tumor characteristics including stage and site-specific variables, zip code-level socioeconomic factors, facility characteristics and insurance status as well as treatments status.
Patients diagnosed with AML from 1998-2011 and followed-up to the end of 2012 aged 18-64 years were included in the analysis. Age was divided into two sub-categories: 18-49 and 50-64. Race was aggregated into White, Black and Asian. Payer status was categorized as uninsured, private, Medicaid, Medicare (or other government insurance plan), or unknown. Income, or median household income at zip-code level, was grouped as <$30k, $30-34k, $35-45k, or ≥$46k. The percentage of adults in the patient's zip code who did not graduate from high school, as a measure of education, was grouped as ≥29%, 20-28.9%, 14-19.9%, and <14%. Zip-code-based level of income and education were determined using 2000 census data (32). Distance travelled, the distance from the patient's residential zip code to a medical center was grouped as <30 and ≥30 miles. Charlson Comorbidity Index, a score that indicates the overall health status of a patient, was defined as 0, 1, ≥2, or unknown (33). Facilities were classified by the NCDB into community facilities, comprehensive cancer centers and academic centers.
Among all patients, only 1.24% received autologous transplant and 6.32% received allogenic transplant. For simplicity, we combined the autologous and allogenic transplants in a common group of SCT. Treatment modality was grouped as no chemotherapy–no SCT, chemotherapy alone, and chemotherapy with SCT, which was based on whether patients received chemotherapy and SCT (either allogenic or autogenic).
Descriptive data were gathered and further subdivided by treatment modality for the following characteristics: sex, age, race, comorbidity score, payer status, income, education, and distance from treating facility and facility type. Chi-square analysis was used to test for differences among the treatment modalities for factors investigated in this study. Direct adjusted median overall survival, 2- and 5-year direct adjusted survival were estimated by using multivariate Cox regression. Statistical analyses were performed with statistical software SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Table I presents patients' characteristics of patients with AML included in this study. There were 34,816 patients diagnosed with AML aged 18-64 years from the NCDB. Fifty-one percent of patients were between 50 and 64 years old. Eight-four percent of patients received chemotherapy only. Only 7.55% of patients received chemotherapy as well as SCT, and 8.30% received neither chemotherapy nor SCT. The majority of patients were White (84.82%), with no comorbidities (54.50%), and private insurance (69.07%). For patients with AML under 65 years old, 30%, 16% and 14% of those with Medicare, Medicaid, and private payer status, respectively, had comorbidity (data not shown).
Table II presents the distribution of patient treatment modality by demographics, and socioeconomic as well as clinical characteristics of the patients with AML in this study. There were statistically significant associations between the treatment modality and all factors investigated in the study (all p<0.001). Patients aged 50-65 years (6.3%) and diagnosed prior to 2004 (6.1%) were less likely to receive both chemotherapy and SCT compared to younger (8.9%) and patients diagnosed after 2005 (8.8%). Black patients (3.3%) were less likely to receive chemotherapy and SCT than White patients (8.1%).
Of patients with comorbidities index 0, 1 and 2, 9.3%, 6.2% and 3.1% of patients received dual treatment. As income, level of education and distance from the treating facility increased, so did the rates of treatment with both chemotherapy and SCT. The majority of patients were treated at an academic center (n=18737) and 11% received both chemotherapy and SCT.
Multivariate analysis demonstrated that patients who received chemotherapy alone were 58% less likely to die than those receiving no chemotherapy and patients who received both chemotherapy and SCT were 65% less likely to die compared to the no-treatment group (Table III). The direct adjusted median overall survival for patients treated with chemotherapy with SCT, chemotherapy only and neither chemotherapy nor SCT were 32.3 months, 23.4 and 6.8, respectively.
The 2-year direct adjusted overall survival rates were 54.1%, 48.1% and 19.8% for patients treated with both chemotherapy and SCT, chemotherapy only, and neither chemotherapy nor SCT, respectively (Figure 1). Compared to no chemotherapy–no SCT, addition of chemotherapy improved 2-year direct adjusted overall survival rate by 27%, addition of SCT to chemotherapy improved this further by 6%. The 5-year direct adjusted overall survival rates were 44.11%, 37.8% and 12% for patients treated with both chemotherapy and SCT, chemotherapy only, and neither chemotherapy nor SCT, respectively.
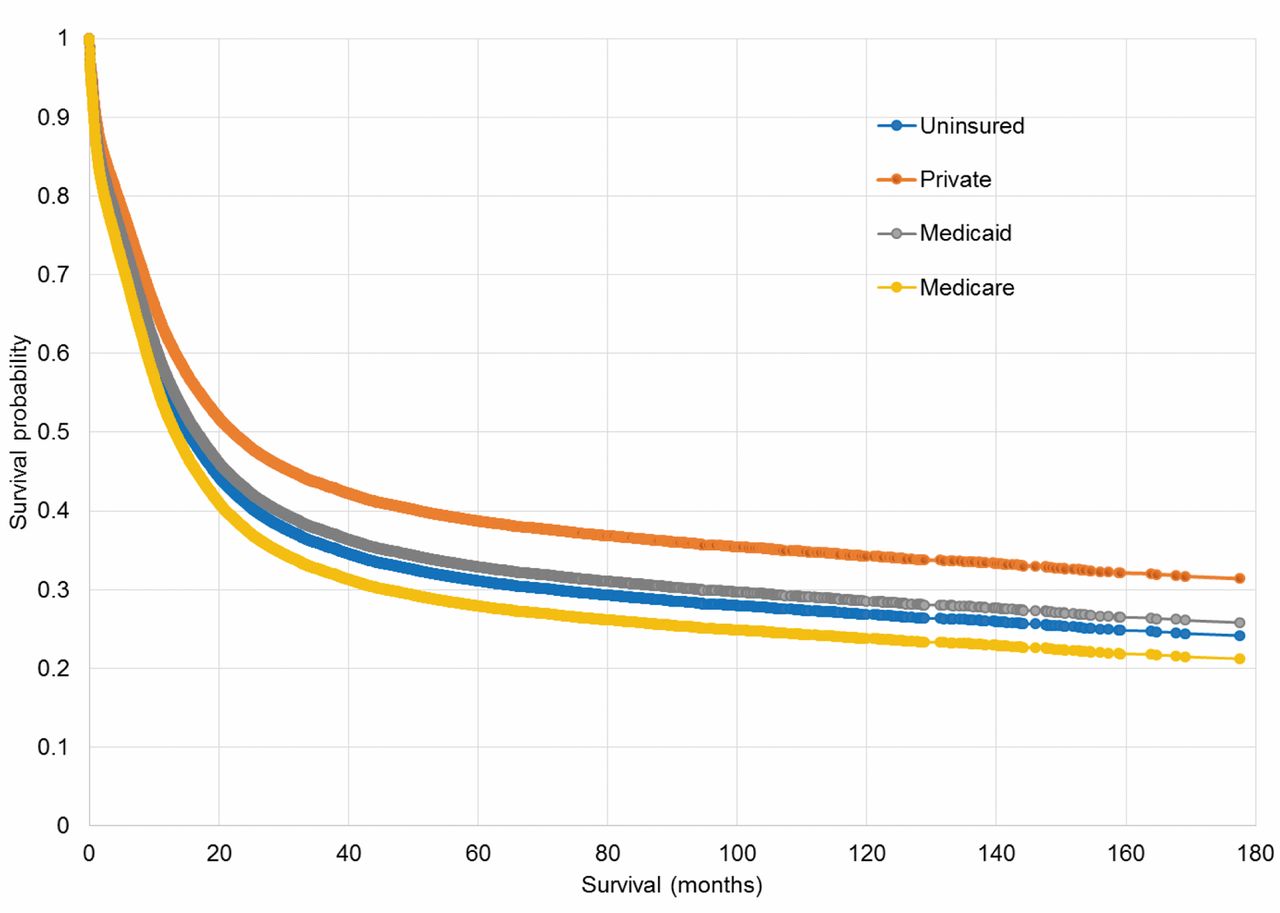
The 2-year, and 5-year direct adjusted overall survival were 48.7%, 37.8% and 42.9%, and 38.7%, 27.9% and 32.9%, respectively, for those patients with private, Medicare and Medicaid (Figure 2). Irrespective of treatment modality, patients with private insurance had a median overall survival of 22.14 months compared with those with Medicare (13.17 months), the uninsured (15.21 months), and those with Medicaid (16.23 months).
Increased age and comorbidities as well as lower income were also associated with increased risk of death. Significant disparities were seen with payer source, Medicaid, Medicare and the uninsured all demonstrated increased risk of death (all p-values <0.0001) when compared to patients with private insurance.
Discussion
Overall, our results showed an improved overall survival for patients treated with both chemotherapy and SCT when compared to chemotherapy only, which itself showed improve survival compared to no treatment. These results highlight the survival advantage of chemotherapy and SCT in eligible patients. Previous studies and NCCN guidelines recommend SCT for intermediate- to high-risk patients with AML who are less than 60 years of age (7, 9, 34, 35). Treatment of AML has been divided into induction chemotherapy and post remission therapy. Patients who do not receive post remission therapy may experience relapse, usually within 6-9 months. Although successful induction therapy clears the visible signs of leukemia in the marrow and restores hematopoiesis in patients with de novo AML, additional post remission therapy may be needed to reduce the residual abnormal cells to a level that can be contained by immune surveillance. Two international clinical trials and population-based study using Swedish data show better outcomes in patients with AML who received SCT in first remission (36, 37).
Receipt of SCT in addition to chemotherapy had a significant impact on mortality. We found that compared to patients who did not receive chemotherapy or SCT, patient who received chemotherapy were 58% less likely to die and those who received dual treatment were 65% less likely. Our finding is consistent with a previous study by Mitchell et al., who found that the risk of dying was 4.3% for patients who received SCT as compared to 8.8% for patients with leukemia who did not (38).
SCT leads to better survival in patients with AML but other factors might affect the ability of these patients to receive SCT. Few studies have attempted to investigate factors that may relate to access to SCT using population-based studies (38). Studies have shown that the Comorbidity Index is an independent predictor for early death in elderly patients with AML but not in those younger than 60 years. A higher Comorbidity Index score predicts shorter survival in adult patients with AML (33, 39, 40). Our findings are consistent with those studies. This might be due to patients being less likely to undergo SCT with higher comorbidities present.
Patients' characteristics: 1998-2011 (32).
Having private insurance coverage increased the chances a patient received SCT, as well as improving patient survival (38). Our results are consistent with a previous study which found that that Medicaid, self-pay and Health Maintenance Organization enrollees with leukemia were significantly less likely than those with private coverage to undergo SCT (38). Our findings are also consistent with previous studies on payer status and other cancer patient survival (10-12, 41-43). Although the mechanism by which payer status affects overall survival is not entirely clear, it could be mediated through differences in access to certain treatment types (44).
Patients' characteristics by treatment type: 1998-2011 (32).
Our data suggest a trend towards better survival in patients with higher family income. Hematopoietic SCT is an expensive procedure and the first-year estimated cost of allogenic SCT was in the range of $100,000 to 200,000 in 2012(45). According to an Agency for Health Care Research and Quality report, SCT generated the most rapid increase in total hospital costs from 2004 to 2007, with a growth rate of 84.9% and $1.3 billion spent in 2007(46). It was estimated that 25.6% of this increase was the result of an increase in the mean cost of hospital stay, and 59.3% was the result of an increase in the number of hospital days of stay. In the wake of the Affordable Care Act and its impact on insurance coverage, evaluating the effect of insurance status on health outcomes is urgently necessary. Our data suggest that SCT along with having private insurance was associated with improvement in survival compared to other payer status (Figure 1). These findings raise concerns about access to expensive cancer treatment for patients who lack insurance or have Medicaid coverage. With limited financial resources, the costs increase as the number of SCTs increases, and states may be forced to implement even more stringent eligibility criteria for expensive cancer treatment such as SCT. Private insurance plans offered on the state exchange markets may also adopt strategies designed to limit access to expensive cancer treatments.
There was a trend towards better survival outcomes in patients with higher education and longer travel to the treatment center, but this was not statistically significant, which was consistent with previous studies which did not show significant survival difference based on distance travelled to reach the treatment center (47-49).
Multivariate Cox regression.
Similar to findings from other studies, we observed that patients with higher age and higher Comorbidity Index had worse survival from AML (21, 22). Contrary to previous studies which demonstrated that men are more likely to undergo SCT than women (50, 51), we identified men were less likely to undergo SCT (7.2% vs. 7.9%). The current study further shows that female were 10% less likely to die compared to males. But one study by Mehta et al. found no significant difference in frequency of SCT based on gender (52). One study found that Hispanics had lower 1- and 3-year adjusted survival rates than Whites, but such disparities were not evident for Whites versus Blacks (53). As shown in previous studies, Whites were more likely to undergo SCT compared to Blacks and Asians (51, 54).
Despite efforts to account for as many confounding variables as possible while utilizing a large sample population, there are limitations to this study. Due to the limited number of variables we were able to apply in our analysis, there may still be a few important confounding variables for which we could not control. Education and income were collected by zip code rather than by patient or household. Utilizing individual or household income in the analysis would have strengthened the results. Information regarding cause of death was also not collected by the NCDB. Measuring treatment as well as other factors such as payer status effect on cause-specific survival might yield different results. In our study, we did not differentiate SCT into allogenic vs. autologous transplant. However, there were only 16% patients who received autologous transplant among all the SCTs. We do not expect a dramatic change in the finding if we separate autologous and allogenic transplants. In addition, for patients who received SCT, the date of transplant, age of patient at transplant, and length of chemotherapy before and after transplant were not investigated. The NCDB does not release detail data on certain variable such as type of private insurance, as well as changes over time of payer status for each patients. Furthermore, due to the retrospective nature of the study, selection bias, especially for chosen treatment modality, is an issue.

The 2-year and 5-year direct adjusted survival rates for patients with both chemotherapy and SCT, chemotherapy only and neither chemotherapy nor SCT.

The 2-year and 5-year direct adjusted survival rates for uninsured, patients with private insutance, Medicaid and Medicare.
Conclusion
Our study demonstrates that patients with AML treated by chemotherapy with SCT had a better survival compared to those treated with chemotherapy alone; and patients treated with chemotherapy alone had a better survival than those who received neither chemotherapy nor SCT. Advanced age, increased Comorbidity Index, lower income, lack of private insurance, and travelling <30 miles to get to the treatment center were significantly associated with worse overall survival.
Acknowledgements
The Authors wish to acknowledge the Commission on Cancer of the American College of Surgeons and the American Cancer Society for making public data available through the NCDB. The data used in this study were derived from a de-identified NCDB file. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytic or statistical methodology employed or the conclusions drawn from these data by the investigator.
Footnotes
This article is freely accessible online.
- Received December 29, 2015.
- Revision received March 3, 2016.
- Accepted March 11, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}