


Abstract
Background: The aim of this phase II study was to evaluate the feasibility of a neoadjuvant chemotherapy regimen consisting of divided-dose docetaxel and cisplatin, with 5-fluorouracil (NAC-DCF), for treatment of patients with stage II/III squamous cell carcinoma of the esophagus (SCCE). Patients and Methods: The NAC-DCF regimen, consisting of 2-h infusion of docetaxel at 35 mg/m2 on days 1 and 8, 4-h infusion of cisplatin at 12 mg/m2 on days 1-5, and continuous infusion of 5-fluorouracil at 600 mg/m2 on days 1-5, was administered. We compared NAC-DCF with conventional NAC-CF. Results: The DCF group comprised of 45 patients, and the CF group comprised of 28 patients. The incidence of grade 3/4 neutropenia was significantly higher in the DCF group (56%) than in the CF group (0%). Grade 2/3 pathological response was attained in a significantly higher percentage of patients in the DCF group (40%) than in the CF group (11%) (p=0.0153). Conclusion: This DCF regimen led to a high frequency of pathological responses among patients with advanced SCCE.
Squamous cell carcinoma of the esophagus (SCCE) has a poor prognosis compared to that of other types of gastrointestinal cancers (1-4). The Japan Clinical Oncology Group (JCOG) 9907 study revealed that preoperative chemotherapy with cisplatin plus 5-fluorouracil (5-FU) (CF) is superior to postoperative chemotherapy among patients with clinical stage II/III SCCE (5). Therefore, in Japan, the current standard treatment for clinical stage II/III SCCE is a protocol involving neoadjuvant chemotherapy (NAC) with CF, followed by surgery.
However, patients who undergo the CF regimen seldom achieve a complete response, and their response rates (complete or partial) are less than 40%, that is unsatisfactory (5-7). In a subgroup analysis of the JCOG 9907 trial, the CF regimen was found to lack efficacy in patients with clinical stage III disease or T3 tumors (5). To improve the survival of patients with advanced SCCE, more-effective regimens are urgently needed.
NAC with docetaxel plus CF (DCF) is one of the most promising new regimens for treatment of advanced SCCE. The feasibility of a regimen involving NAC with DCF was recently reported in two clinical studies (7, 8) and a phase II study (9). In these previous studies, the clinical response rates ranged from 54% to 64%, and the pathological response rates (grade 2 or 3 according to the Japanese Classification of Esophageal Carcinoma) ranged from 26% to 63% (7-10). However, grade 3/4 neutropenia and febrile neutropenia (FN) were observed in 78-87% and 2-24% of the patients, respectively (7-9). Thus, although NAC-DCF is effective, it is associated with a significant incidence of high-grade acute toxicity (7-9).
In these previous studies of NAC–DCF, docetaxel was administered at a dose of 60-75 mg/m2 on day 1 (7-9, 11). This previous regimen comprised 3 or 4 weekly treatments with docetaxel. We hypothesized that two divided doses of docetaxel, on days 1 and 8, would be ideal to reduce the severity of toxicities, because weekly docetaxel is associated with minimal myelosuppression (12).
In addition, several previously reported studies of NAC–DCF involved high-dose cisplatin bolus regimens (8, 9, 11). During chemoradiotherapy (CRT) for unresectable advanced esophageal cancer, protracted low-dose cisplatin chemotherapy is associated with a relatively low incidence of high-grade acute toxicity (13, 14). Therefore, we hypothesized that a low-dose cisplatin regimen, as part of a NAC–DCF regimen for advanced SCCE, might be associated with lower toxicity.
In this study, we evaluated a protocol employing a NAC–DCF regimen involving divided-dose chemotherapy for patients with advanced SCCE to determine whether the modified regimen would result in good efficacy with reduced toxicities. We also compared the survival benefit of the modified regimen with that of conventional NAC with CF.
Patients and Methods
Eligibility criteria. This study was conducted according to a protocol reviewed and approved by the Ethical Committee on Human Research at Wakayama Medical University Hospital (Approval number 957). All patients gave their written informed consent before entry into the study. The study protocol was registered in the University Hospital Medical Information Network (UMIN000007408).
Patients were regarded as eligible if they met the following criteria: (i) pathologically confirmed SCCE; (ii) planned curative esophagectomy with 2- or 3-field lymph node dissection; (iii) clinical stage II, III, or IV (M1 lymph node) according to the International Union Against Cancer's TNM Classification of Malignant Tumors (7th ed.) (15); (iv) Eastern Cooperative Oncology Group performance status of 0-1; (v) age of 20 years or older; and (vi) normal function of major organs, as indicated by a leukocyte count of 3,000-12,000 mm3, neutrophil count of >1,500 mm3, platelet count of >100,000 mm3, hemoglobin of >8.0 g/dl, aspartate aminotransferase and alanine aminotransferase levels of <150 IU/l, and creatinine level of <1.5 mg/dl.
Chemotherapy. The DCF group consisted of 48 patients from a previously conducted phase I study of DCF chemotherapy for metastatic or unresectable SCCE (NCT00915850) (16). These patients were treated by means of the following DCF regimen: 2-h infusion of docetaxel at 35 mg/m2 on days 1 and 8, 4-h infusion of cisplatin at 12 mg/m2 on days 1-5, and continuous infusion of 5-FU at 600 mg/m2 on days 1-5 (DCF: 70/60/600). Dose modification was based on the worst toxicity in neutropenia observed during the previous course. For FN or grade 4 neutropenia, the docetaxel dose was reduced by 5 mg/m2 (30 mg/m2) in the subsequent cycle after recovery to grade 1.
The CF group consisted of 29 patients who did not agree to participate in the DCF study and who were treated by means of a NAC–CF regimen based on the results of the JCOG 9907 trial (5). The CF regimen was as follows: 4-h infusion of CDDP at 80 mg/m2 on day 1 and continuous infusion of 5-FU at 800 mg/m2 on days 1-5 (CF: 80/800).
The DCF and CF regimens were repeated every 3 weeks until toxicity became unacceptable, the patient refused treatment, or disease progression was observed, up to a maximum of two cycles.
Response and toxicity. We judged the antitumor effects of the treatment regimens in accordance with Response Evaluation Criteria in Solid Tumors (ver. 1.0) on the basis of enhanced computed tomographic scans conducted every 3 weeks (17). For safety assessment, we used the National Cancer Institute Common Toxicity Criteria (ver. 2.0) (18).
Surgery and pathological response. Surgery was carried out within 42 days of the last date of the second chemotherapy cycle. Traditional open right transthoracic esophageal resection or minimally invasive thoracoscopic esophageal resection with 2- or 3-field lymph node dissection were performed (4, 19). Postoperative complications were analyzed according to the Clavien-Dindo classification (20). Complications higher than grade II were regarded as clinically significant. Surgical specimens were evaluated pathologically and graded according to the proportion of tumor affected by degeneration or necrosis by means of the Japanese Classification of Esophageal Carcinoma (10).
End-point and statistical analysis. The primary endpoint was the pathological response rate (more than grade 2) (10), and the secondary endpoints were the curative resection rate (TNM R0 resection) (15), clinical response rate (complete or partial response) (17), postoperative complications, 2-year overall survival (OS), 2-year relapse-free survival (RFS), and treatment-related toxicity (18). The planned sample size of the phase II study was 45 patients, which is the number of patients necessary to confirm the null hypothesis that the 95% confidence interval of the pathological response rate (55%) would be less than 30% under conditions of an αerror of 0.05 and a β error of 0.2.
Survival curves were computed by means of the Kaplan–Meier method and were compared by means of the log-rank test; a value of p<0.05 was considered to indicate statistical significance. Quantitative results are expressed as medians and ranges. Statistical comparisons between the two groups were performed with χ2 statistics, and p<0.05 was considered to indicate statistical significance. The SPSS software program (ver. 15.0; SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
Results
Patients' characteristics. Between January 2008 and December 2012, a total of 48 patients were enrolled in this phase II study. Of these, 45 received DCF and underwent subsequent surgery (DCF group). The CF group comprised 29 patients who received CF. Of these, 28 patients underwent subsequent surgery (CF group) (Figure 1). There were no differences between the two groups in terms of male/female ratio, age, tumor site, or distribution of tumor stages (Table I).
Adverse events. The adverse events observed during chemotherapy are shown in Table II. Patients in the DCF group had a high incidence of hematological toxicity. On the other hand, among patients in the CF group, grade 3/4 toxicities were almost absent.
Clinical response to chemotherapy. In the DCF group, of 37 patients who had evaluable lesions, 16 (43%) patients had a complete or partial response. In the CF group, of 23 patients who had evaluable lesions, six (26%) patients had a complete or partial response (p>0.05, Table II).
Operative details and postoperative complications. In the DCF group, 45 patients underwent surgery, and curative resection (R0) was performed in 39 patients (87%). In the CF group, 28 patients underwent surgery, and curative resection was performed in 25 patients (89%). The curative resection rates in the two groups were similar. Eleven patients (24%) in the DCF group and eight patients (29%) in the CF group had grade II or higher postoperative complications, and there were no differences between the two groups (p>0.05, Table II). There was no in-hospital mortality in either group.

Treatment summary. DCF: Docetaxel + cisplatin + fluorouracil; CF: cisplatin + fluorouracil; CRT: chemoradiotherapy.
Pathological response to chemotherapy. In the DCF group, pathological complete response (grade 3) was achieved in eight (18%) patients. Grade 2 was seen in 10 (22%), giving an overall pathological response rate (grade 3 or 2) of 40%. In the CF group, 1 (4%) grade 3 and 2 (7%) grade 2 responses were observed, giving an overall response rate of 11%. The proportion of patients with an overall pathological response was significantly higher in the DCF group (p=0.0153, Table II).
Down-staging. To assess down-staging, we compared the clinical stage before chemotherapy with the pathological stage after chemotherapy. The rate of down-staging in the DCF group (40%, 18 patients) was significantly higher than that in the CF group (11%, 3 patients) (p=0.0153).
Second- and third-line therapies. No patients in the DCF group received postoperative adjuvant chemotherapy. In the CF group, 11 patients received adjuvant chemotherapy, either additional CF (n=2) or DCF (n=9). After relapse, sequential second- and third-line therapies were given to 21 patients in the DCF group: DCF (n=14), S-1 (n=6), and CRT (n=8), and additional pneumonectomy (n=2) (overlapping). Among the patients in the CF group, 12 patients received additional therapy: DCF (n=10), S-1 (n=4), CRT (n=4), and additional neck dissection (n=1) (overlapping).
Patients' characteristics.
Survival. The median follow-up in the DCF group was 37 months (range: 21-78 months), and that in the CF group was 48 months (range: 27-74 months). During the follow-up period, recurrence occurred in 25 patients (56%) in the DCF group and 17 patients (61%) in the CF group. The difference between the recurrence rates in the two groups was not significant. Local recurrences (including mediastinal lymph node) developed in 14 patients (31%) in the DCF group and 11 patients (39%) in the CF group. Distant metastases developed in 14 patients (31%) in the DCF group and 12 patients (43%) in the CF group.
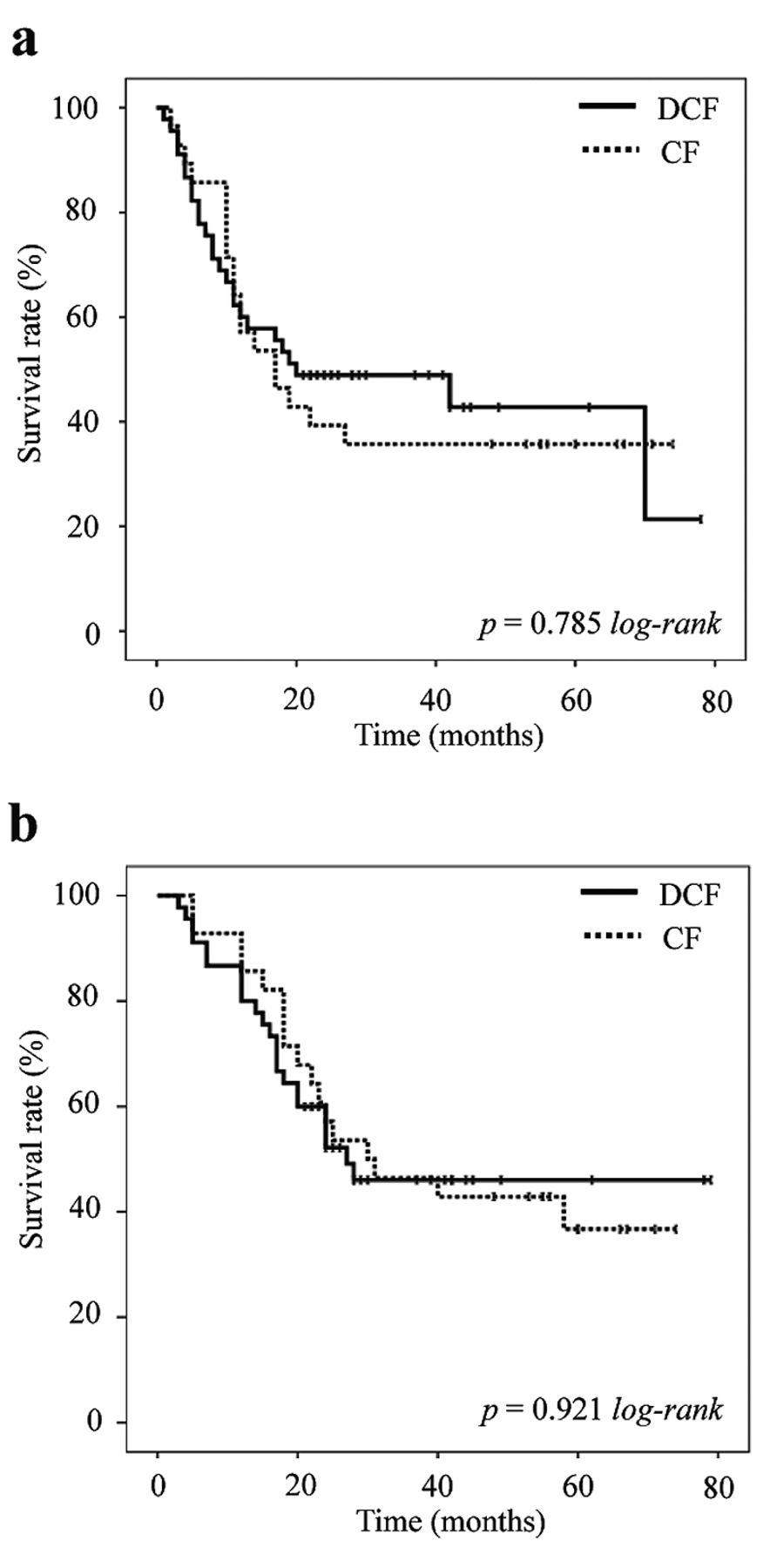
Survival analysis was conducted on all patients (Figure 2). There were no significant differences in the RFS and OS rates between the two groups.

Kaplan–Meier estimates of relapse-free survival (a) and overall survival (b). The 2-year relapse-free survival rate for patients in the docetaxel with cisplatin plus fluorouracil (DCF) group was 48.9% and that for patients in the cisplatin plus fluorouracil (CF) group was 39.3%. The 2-year overall survival rate for patients in the DCF group was 60.0% and that for patients in the CF group was 57.1%.
Discussion
This phase II study was designed to evaluate the safety and efficacy of modified DCF as NAC for patients with advanced SCCE, as well as to investigate whether modified DCF had better survival benefit than conventional CF. The novel aspect of our treatment regimen involved division of the docetaxel and cisplatin into two and five doses, respectively, to reduce the severity of toxicities. The clinical and pathological response rates to NAC with DCF were 43% and 40% respectively (Table III), and these rates were higher than the corresponding rates in the conventional CF group but did not exceed previously reported rates for conventional DCF regimens (7-9). The incidence of chemotherapy-related neutropenia was lower than previously reported incidences (7-9). These findings suggest that this modified DCF therapy is safe and efficacious as NAC for advanced SCCE.
Adverse events, clinical and pathological responses, operative details, and postoperative complications in patients treated with docetaxel with cisplatin plus fluorouracil (DCF) and those treated with cisplatin plus fluorouracil (CF).
The most frequent toxicity of DCF was myelosuppression, but the rate of grade 3/4 neutropenia was lower than the rates for previously reported DCF therapies (Table III) (7-9). In a previous study by Hara et al. of conventional DCF regimens, grade 3/4 neutropenia was observed in 83% of patients, whereas FN was seen in only 2.4% (9). The reason for the difference in the rates of FN between these two reports, despite the similar rates of grade 3/4 neutropenia, is not clear, but it may be related to differences in the condition of the patients and the prophylactic use of antibiotics in the other study (9). In this study, FN was observed in 20% of the patients. It should be noted that myelosuppression decreased rapidly (within 5 days) after administration of granulocyte colony-stimulating factor and did not necessarily delay surgery. Thus, careful monitoring for myelosuppression could ensure safe completion of the DCF regimen. In addition, DCF had no negative impact on postoperative complications as compared with CF.
Neoadjuvant chemotherapy with docetaxel with cisplatin plus fluorouracil (DCF) for patients with squamous cell carcinoma of the esophagus.
We found that NAC with DCF provided high clinical and pathological responses among patients with SCCE, and it resulted in disease down-staging in 40% of the patients. Compared with the patients who received NAC with CF, patients who received NAC with DCF had significantly better pathological response rates and disease down-staging rates. However, the survival benefit of DCF was not better than that of CF. In addition, the 2-year RFS rate was poorer than previously reported rates (7-9). There are several possible reasons for this difference. In this study, the use of dosages of docetaxel, cisplatin, and 5-FU were 70, 60, and 3,000 (mg/m2)/course, and two courses were administered. In one of the other studies, a maximum of three cycles of the DCF regimen were allowed (9). The doses used in our study were smaller than those in two of the previously reported DCF regimens (8, 9), and therefore, the strength of the chemotherapy might have been insufficient in our case.
This phase II trial has two limitations. Firstly, although there were no differences between the DCF and CF groups in terms of distribution of tumor stage, the tumor diameter was significantly larger in patients receiving DCF than in the patients receiving CF. More patients with local progressive tumors might have been included in the DCF group. The biased demographics in our study might be one of the reasons that our results failed to show a survival benefit for DCF.
The second limitation is that this study was not a randomized controlled trial. The patients receiving DCF were managed within the phase II trial, but the patients receiving CF were managed within clinical practice. Although no patients in the DCF group received postoperative adjuvant chemotherapy, 39% of patients in the CF group did receive it. Adjuvant chemotherapy might have prolonged survival in the CF group. A previous study of the differences between NAC with CF and NAC with DCF indicated that RFS and OS were significantly better in the DCF group than in the CF group (8). However, this previous report was a retrospective study, and thus, the survival rates in the each treatment groups varied at different periods. A phase III randomized controlled trial is needed to clarify the survival benefit of NAC with DCF. The JCOG recently launched a 3-arm randomized controlled trial to confirm the superiority of DCF and CRT with CF as preoperative therapy for locally advanced SCCE (11).
In conclusion, our results indicate that a divided-dose NAC–DCF regimen can be tolerable, safe, and efficacious for treatment of advanced SCCE. However, NAC with DCF was not efficacious for 60% of patients with SCCE, and the survival benefit was not better than that of conventional CF. We are currently searching for predictive molecular markers for pathological response and long survival in patients with SCCE receiving NAC with DCF.
Footnotes
Competing Interests
All Authors have nothing to declare.
- Received November 30, 2015.
- Revision received January 9, 2016.
- Accepted January 13, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}