


Abstract
The aim of this study was to assess the sensitivity and specificity of preoperative diagnosis by diffusion magnetic resonance imaging (D-MRI) for lymph node metastasis of colorectal cancer. The b-value represents the diffusion factor (measured in s/mm2) and the strength of the diffusion gradients. The b-value used in this study was 1,000 s/mm2. A total of 119 patients underwent D-MRI before resection of primary colorectal cancer (52 of the rectum, 67 of the colon) at our hospital between February 2005 and April 2006. Lymph node metastases judged by D-MRI were compared with postoperative pathological results. The form of lymph node metastasis was classified either as abundant or scarce type. The predictive values for lymph-node metastasis (sensitivity and specificity) by D-MRI were calculated from the result of this classification and lymph-node size. The study was divided into two periods: before the consensus meeting in January 2006, (n=79) (P-I), and after the adjustment of the criteria to improve the sensitivity and specificity based on the results of P-I (n=40) (P-II). Detection of lymph node metastasis using D-MRI in P-I had sensitivity of 61%, specificity of 73%, positive predictive value (PPV) of 55%, and negative predictive value (NPV) of 77%, while in P-II, these values improved to 79%, 95%, 94%, and 83%, respectively. Specificity and PPV for P-II were significantly higher than those for P-I (p<0.05). The diameter of lymph nodes judged to be metastatic on D-MRI (P-I vs. P-II: n=32 vs. 16) was 10.3±5.4 (3-28) vs. 9.1±3.0 (4-14) mm; 11.5±6.2 (4-28) vs. 9.2±3.1 (4-14) mm for truly positive nodes (n=18 vs. 15), and 6±3.8 (3-14) vs. 8 mm for false-positive nodes (n=14 vs. 1). On the other hand, lymph nodes judged negative by D-MRI (n=47 vs. 24) was 5.9±2.4 (3-16) vs. 5.7±2.8 (2-15) mm; 5.9±2.1 (3-16) vs. 5.3±2.1 (2-8) mm for truly negative (n=36 vs. 20), and 5.7±2.7 (3-12) vs. 7.8±4.9 (4-15) mm for false negative (n=11 vs. 4). As to the form of metastasis, all truly positive nodes were of the abundant type, and 6/11 (55%) in P-I and 1/4 (25%) in P-II false-negatives were of the scarce type. In conclusion, D-MRI seems useful for preoperative detection of metastatic lymph nodes in colorectal cancer, especially if the node is hyperintense and more than 9 mm in diameter.
Diffusion magnetic resonance imaging (D-MRI) detects water motion over small distances, and enables diagnosis of acute cerebrovascular incidents. Excellent tissue contrast in D-MRI based on molecular diffusion has potential to demonstrate malignant tumors (1-4). When anatomical orientation is difficult on D-MRI, fusion software overlay of D-MRI onto ordinary MR images can resolve the problem. Quantitative measurement of the apparent diffusion coefficient (ADC) values may also be valuable in distinguishing a malignancy from benign lesions (3, 5). Recently, the efficacy of D-MRI in detecting malignancy in the viscera has been reported (6-8), thereby prompting interest in the diagnosis of lymph node metastases by diffusion imaging. The aim of the present study was to assess the feasibility of preoperative diagnosis of lymph node metastasis from colorectal cancer by D-MRI.
Materials and Methods
Technical principles of D-MRI. Diffusion is the thermally induced motion of water molecules in biological tissues called Brownian motion (9). With the addition of motion probing gradient pulses, MRI by means of ADC measurement is currently the best imaging technique for in vivo quantification of the combined effects of capillary perfusion and diffusion. MRI performed prior to the commencement of treatment was performed on either a Philips Intera (Koninklijke Philips N.V., Best, the Netherlands) or a Siemens Avanto 1.5 T (Siemens Healthcare, Erlangen, Germany) MR system using a phased array body coil. T1-weighted sequences with and without fat suppression were obtained after intravenous gadolinium contrast injection and were reviewed in conjunction with the D-MRI images for lesion localization. One abdominal radiologist with more than 20 years of experience in abdominal and pelvic cavity MRI who were blind to the clinical and histopathological information interpreted each of the MRI images independently. Diffusion-weighted imaging can be performed using diffusion gradients on each side of the 180 pulse when using very fast, single-shot spin-echo echo-planar imaging sequences with different b-values. The b-value represents the diffusion factor (measured in s/mm2) and the strength of the diffusion gradients. The ideal b-value for lesion characterization is a trade-off between signal attenuation and perfusion contamination. This is generally possible using b-values of between 300 and 1,000 s/mm2 for lymph node imaging. Pure diffusion contrast is obtained using b-values above 1,000 s/mm2. However, imaging quality can be limited by signal loss that occurs at such b-values and higher. In this study, therefore, the b-value was set at 1,000 s/mm2. Recently, Kim et al. reported that prostate DWI performed at 3 T using high b-values was able to improve differentiation of tumors from benign tissue. DWI performed using a b-value of 1,000 s/mm2 was more sensitive and more accurate in predicting localized prostate cancer than DWI performed using a b-value of 2,000 s/mm2 (10). A relatively high b-value of 1,000 s/m2 may eliminate possible microvascular contamination of the computed apparent diffusion coefficient (ADC) values and may improve the detection of slow-moving water molecules or small diffusion distances, which are essential in the early response evaluations. The b-value of 1,000 was defined as an internationally accepted value.

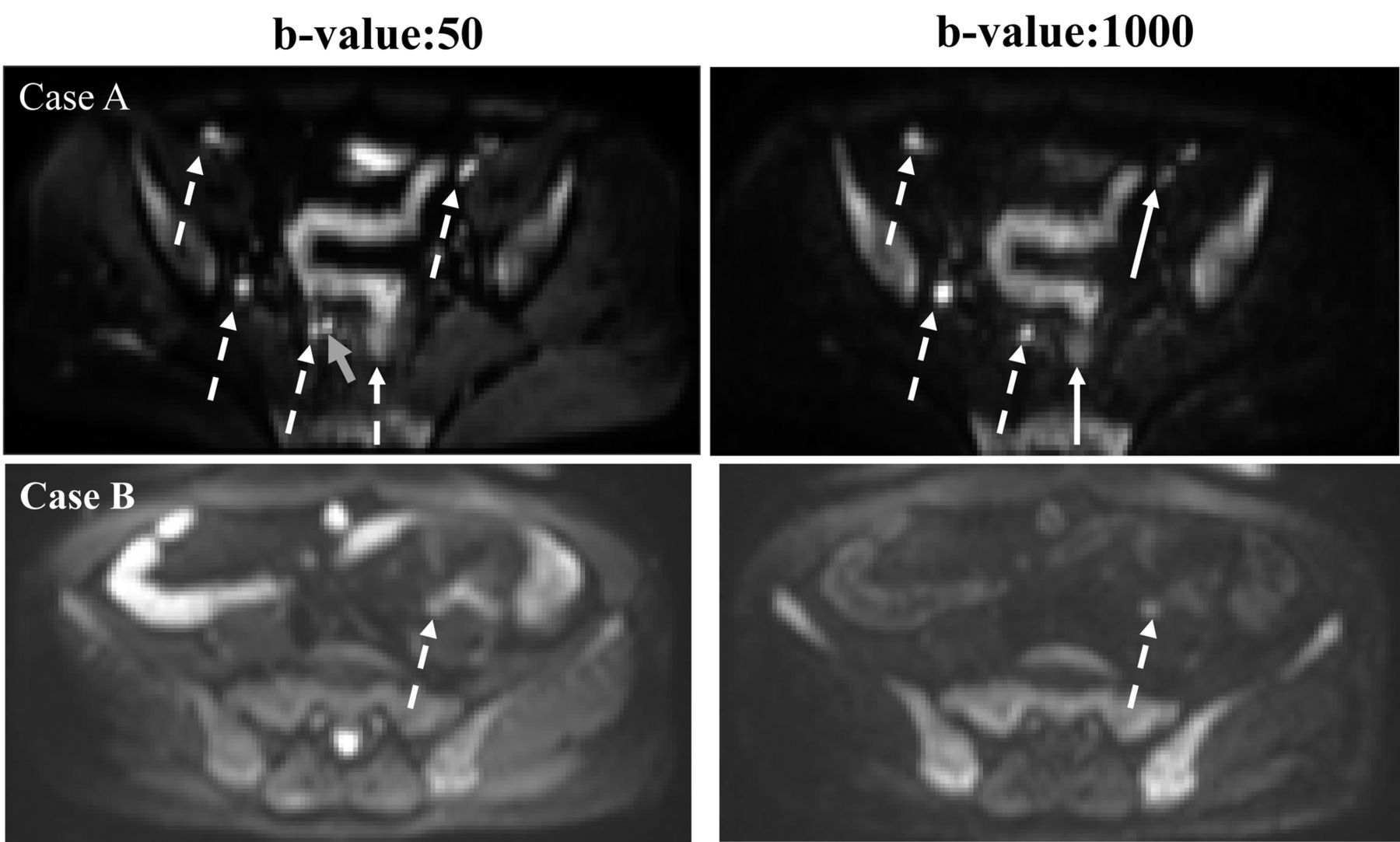
Example of positive lymph node metastasis by diffusion magnetic resonance imaging (D-MRI). Blue arrows: Hot spots are recognized at both b-values. White arrows: hot spot detected only at a low (50 s/mm2) b-value.
Patients and form of lymph node metastasis. A total of 119 patients who underwent D-MRI before resection of primary colorectal cancer (52 of the rectum, 67 of the colon) at Jikei University Hospital between February 2005 and April 2006 were studied. Two surgeons carried out an average operation and were evaluating the procedure. One special radiologist was evaluated in this study, and this evaluation was a routine procedure. Lymph node metastases were judged by D-MRI (Figure 1), and they were compared with the postoperative pathological results. The form of lymph node metastasis was classified as follows: abundant type, with cancerous glands (four or more) occupying the lymph node (Figure 2a); and scarce type, with a small number of cancerous glands (1-3 glands) at the edge of the lymph node (Figure 2b). Values for prediction of lymph node metastasis (sensitivity and specificity) by D-MRI were calculated from the result of this classification and lymph node size. In January 2006, a consensus conference was held in which colorectal surgeons, radiologists specialized in D-MRI, and pathologists discussed the initial 79 cases. After obtaining feedback from pathological findings, the study was continued. Therefore the study period was divided into two periods, Period I (from February 2005 and January 2006) and Period II (from February 2006 and April 2006). In Period II, ‘hot’ nodules of 10 mm or less were defined as positive. In Period I, 79 cases were enrolled: their median age was 58 years (range: 39-79 years), 49 cases had tumor in the rectum and 26 cases were female (34%). In Period II, 40 cases were enrolled: their median age was 61 years (range=43-77 years), 16 cases had tumor in the rectum and 16 cases were female (40%).
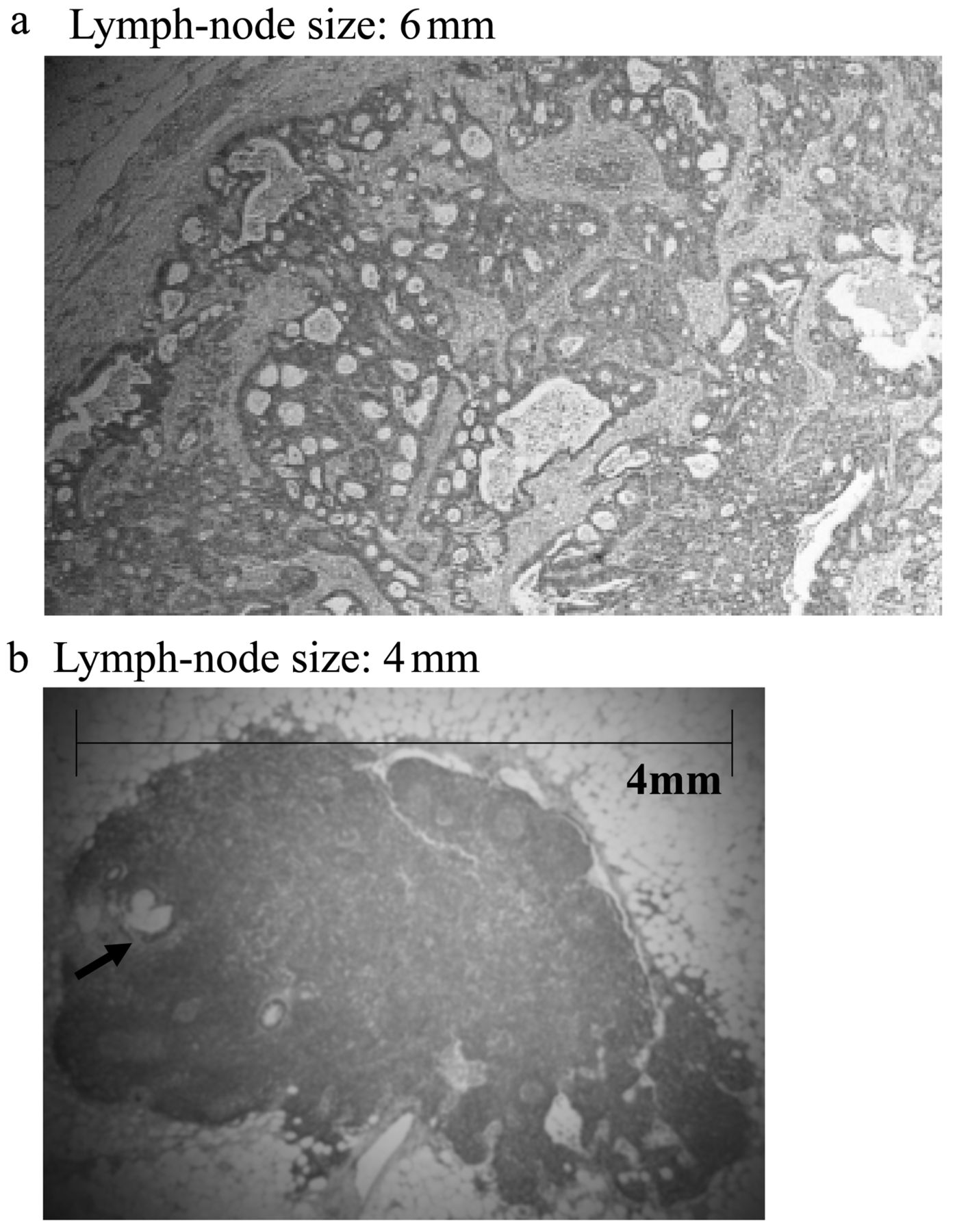
The form of lymph node metastasis. a: Abundant type: four or more cancerous glands occupy the lymph node. b: Scarce type: A small number of cancerous glands (three or fewer glands; arrow) occupy the lymph node.
Results
Sensitivity and specificity. The detection of lymph node metastases by D-MRI in Period I and II is listed in Table I and II. Specificity and positive predictive value for Period II were significantly higher than those for Period I (p<0.05).
Size and form of lymph node metastases. The diameter of lymph nodes interpreted as metastases by D-MRI (Period I, n=32; Period II, n=16) is listed in Table III. Although the diameter of lymph nodes found to be truly metastatic in Period II tended to be smaller than in Period I, no statistically significant difference was observed. Regarding the form of lymph node and accuracy, there were no truly positive cases for any of the scarce type metastases, all truly positive nodes were of the abundant type. The false-negative rate was reduced in Period II (Table IV).
Correlation between pathology and diffusion magnetic resonance imaging (D-MRI).
Sensitivity and specificity of diffusion magnetic resonance imaging in detecting metastases of colorectal cancer.
Discussion
The sensitivity for detection of lymph node metastasis of colorectal cancer by computed tomography (CT) in previous reports ranged between 22% and 84% (11-14). Recently, Filippone et al. reported that combined axial and MRI images using multi-detector row CT improved accuracy and sensitivity (80% and 90%, respectively) of detection of lymph node metastases (15). On the other hand, several reports described that positron-emission tomography (PET) for nodal metastases of colorectal cancer had low sensitivity, ranging between 29% and 37%, and high specificity, ranging between 83% and 96% (16-19). Sang et al. reported that in 31 patients with colorectal cancer, PET/CT had low sensitivity (43%) and high specificity (80%) for regional nodal metastases (20). To our knowledge, little is known about the utility of D-MRI for detection of lymph node metastasis. Koyama et al. reported preliminary data on lymph node metastases of uterine cervical carcinoma, and suggested that D-MRI was more sensitive than T2-weighted images, but has limitations in distinguishing lymph node metastasis from benign lymphadenopathy (5); this is probably because reactive nodes limited the motion of protonated molecules. However, in our experience with 40 patients in Period-II, D-MRI had high sensitivity (79%) and specificity (95%) for detection of regional nodal metastases. The use of size as the most important criterion for differentiation of benign and malignant lymph nodes has limitations: small metastases without an increase in lymph node size are frequently missed. Up to 21% of generally found nodes in all body compartments smaller than 10 mm have been found to represent metastases, while 40% of those larger than 10 mm must be considered benign (21, 22). This is mainly because metastases can be present in non-enlarged lymph nodes and not all enlarged nodes are malignant. Veit et al. described that changing the size criteria towards larger or smaller cut-off values does not solve the problem based on the influence on sensitivity and specificity because a low threshold for cut-off values would increase the sensitivity, but specificity would decrease for example (23, 24). D-MRI has overcome some of these limitations but is still constrained by current resolution limits for small nodal metastases. This has fueled the development of targeted techniques for nodal imaging and characterization, as outlined in this article. Nevertheless, we tried larger and smaller cut-off values. Firstly, detection of hot nodules of 10 mm or less was enforced. Even if a hot nodule was 10 mm or less, we applied strict criteria for nodal staging, i.e. judging positive for clearly hyperintense signals. As a result, we suggest that a hot nodule of 9 mm or more is clearly positive. Secondly, we attempted to detect metastatic lymph nodes 6 mm or less in scarce-type metastases. Regardless of this, we were unable to define a reasonable criterion of nodal staging. Since the high negative predictive value in Period-II was likely due to the low rate of scarce type metastases, it seems impossible to detect scarce type lymph nodes of 6 mm or less using the current D-MRI conditions. However, since the rate of scarce-type lymph node metastasis in colorectal cancer is very low (7/119: 6% in this study), detecting abundant scarce-type metastatic lymph nodes is clinically more important. We believe that the omission of regional lymph node dissection is guilt for patients with colonic cancer because the regional lymph node dissection is a completely safe technique. However, in rectal cancer, the occurrence of positive lymph nodes may indicate the need for neoadjuvant radiochemotherapy or the addition of lateral lymph node dissection.
The diameter of lymph nodes on diffusion magnetic resonance imaging (D-MRI).
Metastasis form according to pathology.
Conclusion
D-MRI seems useful for preoperative detection of metastatic lymph nodes in colorectal cancer, especially if the node is hyperintense and more than 9 mm in diameter.
- Received November 21, 2015.
- Revision received December 22, 2015.
- Accepted January 7, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.