


Abstract
Background: Simultaneous presentation of pregnancy and chronic myeloid leukemia (CML) is rare. Tyrosine kinase inhibitors (TKIs) are rarely used in pregnancy. There is almost no information on the effect of recently developed TKIs on the fetus. Case Report: A 22-year-old woman became pregnant while using radotinib, a novel TKI for CML. She was concerned about the possible teratogenic effect of radotinib; hence the first pregnancy was terminated. The patient underwent full-term delivery at the second pregnancy. The infant had facial deformity and congenital laryngomalacia. Conclusion: We witnessed structural abnormality when the patient used radotinib during the first trimester of pregnancy. When radotinib is prescribed for women of childbearing age, thorough education about contraception is necessary.
Chronic myeloid leukemia (CML) often occurs in elderly patients (1). Simultaneous presentation of pregnancy and CML is rare (2). Because of their excellent therapeutic effect, tyrosine kinase inhibitors (TKIs) have been used as standard treatment for CML (3). However, there is controversy regarding the effectiveness of TKIs and uncertainty about the effects on the fetus due to the lack of reports of their use during pregnancy. Although imatinib is a TKI that has been used since 1998, little information is available about its effect on the fetus during pregnancy. Radotinib, a novel TKI, is a drug used for CML. It is under preclinical trial. Here we report a case of a woman pregnant twice while taking raditinib who gave birth to a baby with congenital malformation.
Case Report
A 19-year-old patient, gravida 1 para 0, was referred for amenorrhea for 7 weeks 6 days. The patient had been diagnosed with CML 1 year earlier and had been taking 200 mg radotinib twice daily orally for 1 year. Six months before referral, in chronic phase, a complete cytogenic response was achieved. Normally, the patient had regular menstruation. The result of urine human chorionic gonadotropin (HCG) test was positive and the ultrasound examination showed that G-sac was 1.26 cm. The fetal pole measured 2.4 mm (5 weeks 5 days of gestation). Fetal heart beat was 105 bpm/min. She was concerned about the teratogenic effect of radotinib; hence she decided to have a termination of pregnancy.
The patient visited the hospital again 3 years later at 22 years old for 11 weeks and 4 days of amenorrhea. Usually she had regular menstruation. The patient had been taking 300 mg of radotinib twice daily orally at that time but had stopped taking radotinib after a urine HCG test was confirmed to be positive 12 days prior to this consultation. Ultrasound examination revealed a single intrauterine pregnancy of 12 weeks and 3 days of gestation. It was conjecturable that she had taken radotinib until 10 weeks and 5 days of gestation. The patient chose to continue the pregnancy and stopped taking radotinib. Blood analysis revealed the following: white blood cell count of 5,490 cells/mm3, hemoglobin level of 9.4 g/dl, and platelet count of 64,000 cells/mm3. Her renal and liver functions were normal. The pregnant woman had regular antenatal checkups; there was nothing significant to report. She had a complete blood count every month. There was no medical opinion of CML deterioration.
At the 39th week and 6th day, the patient gave birth to a baby girl (3.330 kg) vaginally. The Apgar score of the infant was 8 at 1 min and 9 at 5 min. Examination revealed both low-set ears and absence of angle between the forehead and nose (Figure 1A). No other external deformation was found. However, while the patient was breastfeeding, cyanosis and around 70% of desaturation occurred in addition to cow-like crying of the infant. Chest x-ray revealed haziness on both lower lungs. Rib deformity was suspected (Figure 1B). Chest computed tomography showed atelectasis on both lower lungs (Figure 1C). The rib cage was found to be normal (Figure 1D). On echocardiogram, there was nothing significant to report. Laryngoscopy revealed laryngomalacia. The epiglottis was omega-shaped and arytenoid collapsed during inspiration. On placental pathological examination, there was increased intervillous fibrin deposition without any other abnormal findings. The infant's desaturation and atelectasis had improved by the time she was 10 days old. Therefore, she was released from the hospital. There were no other abnormal findings during the 3-month follow-up visit.
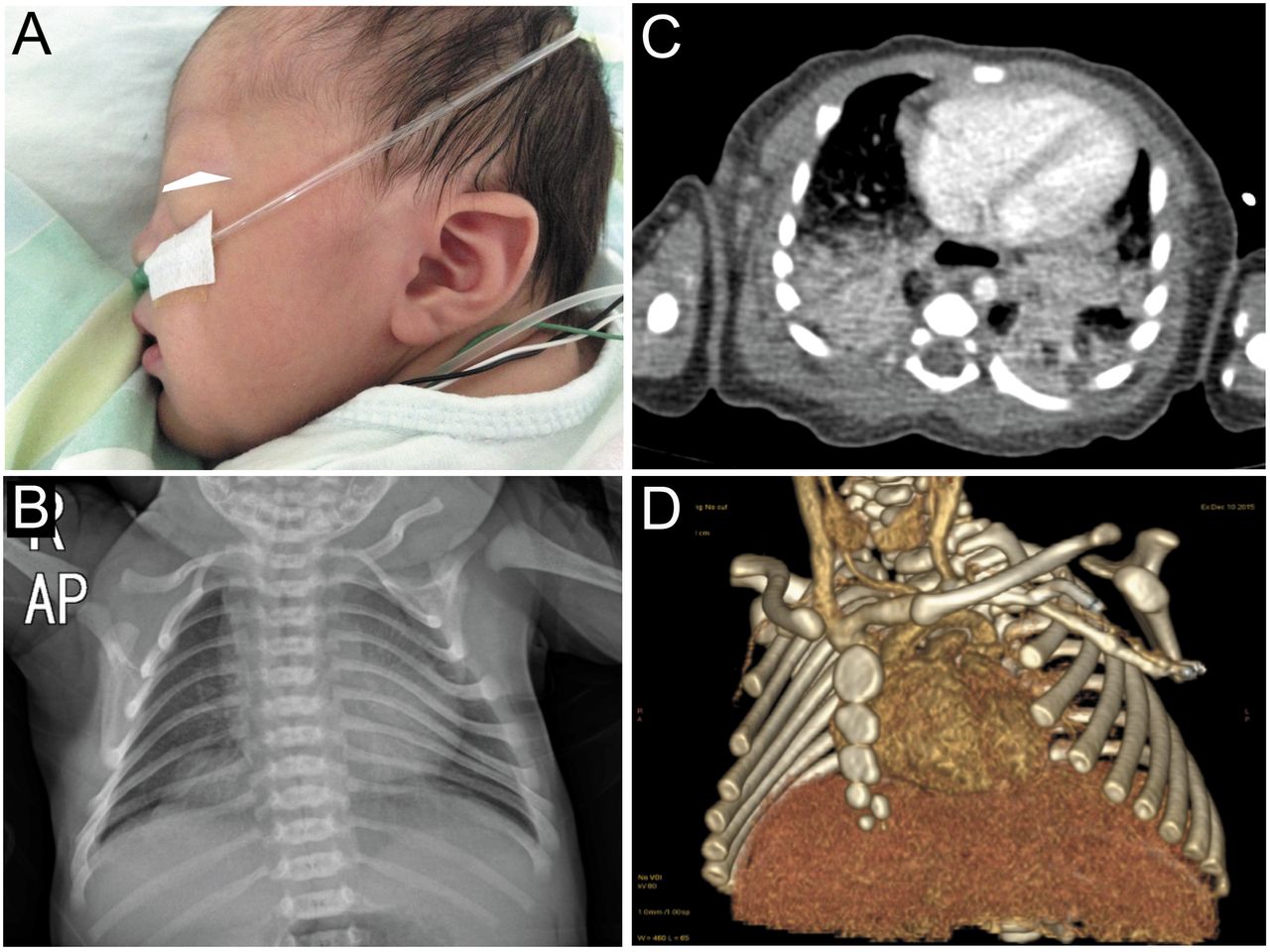
The infant born to a woman who became pregnant while taking radotinib. A: The infant had low-set ears and absence of angle between the forehead and nose. B: Chest X-ray showing haziness in the lower lung field. Rib deformity was suspected. C. Chest computed tomography showing atelectasis of both lungs. D: 3D Chest computed tomography showing the rib cage to be normal.
Discussion
CML comprises approximately 15% of adult leukemia (4). The occurrence rate ranges from 0.6 to two cases out of 100,000 (1). Men are more likely to develop CML (1). The median age at diagnosis is 64 years (1). CML in pregnancy is a rare condition (one in 100,000) (2). Since molecular-targeted therapy with TKIs has been used for treatment of CML, the cure rate of CML has been dramatically improved. Currently, TKIs are the standard treatment for CML (3). Nevertheless, imatinib can increase abortion, congenital malformation, such as exencephaly, encephalocele, and chemical bone hypoplasia in animal studies (5). Although the effect of TKIs on human fetal development remains unclear, several case reports have shown good outcomes. However, one study, in which imatinib treatment was performed, reported that 18 (14.4%) out of 125 pregnant women experienced spontaneous abortion, while babies born to 12 (9.6%) pregnant women had congenital malformation(6). Therefore, a potent teratogenic effect of TKIs should be carefully considered. In addition, newer TKIs, such as dasatinib and nilotinib, have been approved by the US and are available on the market. There are insufficient data about the effect of such medicines on fetal development. Accordingly, whether TKIs should be used during pregnancy is a difficult decision. The decision should be made by the patients, their families, obstetricians, and hematologists together after careful consideration depending on each patient's situation.
We witnessed structural abnormality when the patient used radotinib during the first trimester. To the best of our knowledge, this is the first report of an association between radotinib and pregnancy. Thus, TKIs, especially newer TKIs, should be avoided during pregnancy because their safety is not guaranteed. When it is used on women of childbearing age, thorough education about contraception is necessary.
- Received September 28, 2016.
- Revision received October 19, 2016.
- Accepted October 20, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
In this issue





{kind=link}
Related Articles
Cited By...
- No citing articles found.