


Abstract
Aim: The aim of this study was to evaluate the detection rate of bone metastases and the added value of 11C-acetate (ACE) positron-emission tomography/computed tomography (PET/CT) compared to bone scintigraphy (BS) in high-risk prostate cancer (PC). Materials and Methods: A total of 66 untreated patients with high-risk PC with ACE-PET/CT and planar BS findings within 3 months of each other were retrospectively enrolled. Findings were compared and verified with follow-up data after an average of 26 months. Results: The rate of detection of bone metastases was superior with ACE-PET/CT compared to BS (p<0.01). Agreement between the methods and between BS and follow-up was moderate (Cohen's kappa coefficient of 0.64 and 0.66, respectively). Agreement between ACE-PET/CT and follow-up was excellent (kappa coefficient of 0.95). Therapy was changed in 11% of patients due to ACE-PET/CT results. Conclusion: ACE-PET/CT performed better than planar BS in detection of bone metastases in high-risk PC. ACE-PET/CT findings influenced clinical management.
Prostate cancer (PC) is the second most common male cancer, affecting approximately 15% of men globally (1). Although many PCs remain clinically insignificant (2), aggressive subtypes require early detection and treatment. Predilection sites of metastatic spread in PC are pelvic lymph nodes (LNs) and bone (3).
PC staging depends on parameters such as clinical stage, prostate-specific antigen (PSA) level and Gleason score. Clinical pre-treatment nomograms are used to estimate the risk of pelvic LN involvement and distant metastasis (4). PC with >15% estimated risk of pelvic LN metastasis is clinically considered high-risk PC.
The most common positron-emission tomography (PET) radiotracers for staging and restaging of PC, 11C/18F-choline and 11C-acetate (ACE), reflect cell membrane synthesis. This implies increased uptake of both choline tracers and ACE into the cell membrane of tumour cells, making tumours and metastases detectable by PET/computed tomography (CT) (5). The mechanism of ACE uptake is via up-regulation of fatty acid synthase (6). Comparative studies of 18F-choline and ACE have showed equal diagnostic performance and accuracy in PC recurrence (7). Other promising PET tracers for PC staging are under development, such as 68Ga-labelled compounds that bind to prostate-specific membrane antigen (PSMA), and 18F-fluciclovine (FACBC) (8, 9).
The main clinical applications for ACE-PET/CT are primary staging and restaging of high-risk PC prior to radiotherapy (10-13). Long-term survival data on patients with PC relapse examined with 11C-choline PET/CT showed a 15-year PC-specific survival probability of 42% in PET-positive patients and 96% in PET-negative patients (14). No such long-term data exist for ACE-PET/CT.
Bone scintigraphy (BS) is a widely available standard method for detection of bone metastases in high-risk PC (15). However, pathological BS uptake can result from any condition with increased osteoblastic activity. In order to improve non-invasive N (lymph node) and M (distant metastasis) staging in PC, more accurate imaging methods are needed. For 11C-choline, which has been more extensively studied than ACE, a meta-analysis showed higher specificity for bone metastases with 11C-choline PET/CT compared to planar BS (16). This may also be true for ACE but more evidence is needed, since ACE reflects a completely different biochemical mechanism from that of 11C-choline, although they are similar in terms of cell membrane synthesis. A pilot study on eight BS-positive and ACE-PET/CT-positive patients showed promising results for ACE-PET/CT (17), but otherwise data are limited. Our hypothesis is that ACE-PET/CT should be a more accurate and specific method than BS, with the combination of functional information from ACE-PET with a diagnostic CT.
The aims of this study were to compare the detection rates of suspected bone metastases with ACE-PET/CT and BS in high-risk PC, to validate the results with follow-up data, and to evaluate the added value of ACE-PET/CT defined as change in patient management.
Materials and Methods
All consecutive patients with high-risk PC referred to the Department of Nuclear Medicine at Umea University Hospital, Sweden, during the inclusion period from May 2011 to November 2014, for primary staging with ACE-PET/CT and a 99mTc-hydroxymethylene diphosphonate (HDP) BS within 3 months according to clinical routine work-up, were included in this retrospective study. The patients were referred for ACE-PET/CT prior to radiotherapy with curative intent, therefore patients with known advanced disease were never examined. A total of 66 consecutive patients matched the inclusion criteria. Excluded patients were referred for suspected PC recurrence or did not have BS within the stipulated time range. Clinical data are shown in Table I. The study was approved by the Institutional Review Board (approval number 2013-154-31) and all participants had previously accepted to take part in the clinical routine work-up. The retrospective analyses were performed in accordance with the ethical standards of the Institutional Ethics Committee and with the 1964 Helsinki declaration and its later amendments.
The PET/CT examinations were carried out with a GE Discovery 690 PET/CT scanner (General Electric, Waukesha, WI, USA). The patients were injected with 1-[11C]-acetate (4.0 MBq/kg body weight) intravenously (i.v.), and were examined 10 min post-injection. The PET scan was performed in time-of-flight mode with an acquisition time of 2 min/bed position, from the proximal femur to the head. Data were reconstructed with the OSEM-based VuePoint HD (General Electric, Waukesha, WI, USA). The diagnostic CT covered the same part of the body with 50 cm field-of-view. The majority of the examinations (58/66) included a contrast-enhanced CT (Omnipaque 350 mg iodine/ml at a dose of 0.5 g iodine/kg). and the remaining were examined with a diagnostic CT without i.v. contrast, due to previous contrast reaction, recent contrast-enhanced CT or impaired renal function.
The BS images were acquired with an Infinia Hawkeye 4 gamma camera (General Electric) with whole-body anteroposterior and posteroanterior scans 2.5 h after i.v. injection of 550 MBq 99mTc-HDP, according to European Association of Nuclear Medicine guidelines (18).
Two physicians licensed in both radiology and nuclear medicine evaluated all ACE-PET/CT and BS studies, with simultaneous access to the referral texts. Focal lesions with ACE uptake visually exceeding the skeletal background were interpreted as metastases. The regions of interest (ROIs) were measured with the default delineation threshold of 42% with PET VCAR software (AW 4.5; General Electric) to determine the maximum standardized uptake value (SUVmax; g/ml). Suspected bone metastases from PC were characterized as focal uptakes visually exceeding skeletal background with or without sclerosis. Increased ACE uptake was considered the most suspected PET/CT characteristic unless some more likely explanation than PC bone metastases could be found, e.g. fracture without morphological signs of metastasis.
BS was visually evaluated as in clinical routine. BS uptakes that could be related to a history of previous trauma or degenerative changes were considered non-metastatic. Any other increased non-physiological BS uptakes were considered metastatic.
Clinical data of patients included in this study.
Agreement between imaging results by 11C-acetate-positronemission tomography/computed tomography and 99mTchydroxymethylene diphosphonate bone scintigraphy (BS) at patient level.
Pre-treatment consensus decision was made by the oncologist in discordant cases where patients were diagnosed with bone metastases or not after clinical consensus interpretation of biochemical parameters (PSA, blood count and alkaline phosphatase), clinical symptoms (localized skeletal pain) and existing imaging findings (ACE-PET/CT, BS, magnetic resonance imaging (MRI) or other modality). Since ACE-PET/CT findings influenced pre-treatment consensus decision, we chose not to compare our results with consensus to avoid circle evidence. Follow-up data (clinical evaluation, available imaging, biochemical parameters as above) were collected from the discordant cases, for comparison with ACE-PET/CT and BS results.
BS has in previous publications been outperformed by PET/CT (19, 20). Therefore, we chose not to use BS as the standard of reference. Instead we compared the detection rates of the two methods on a patient basis with the Fischer exact test.
Cohen's kappa coefficient was used to calculate the degree of agreement between ACE-PET/CT and BS, and to compare both methods with clinical follow-up after an average of 26 (range=16-41) months. All statistical analyses were executed in IBM SPSS Statistics 22 (IBM Corp., Armonk, NY, USA).
Results
ACE-PET/CT was significantly superior to planar BS in detecting suspected bone metastases in high-risk PC (p<0.01). Corresponding results in ACE-PET/CT and BS were seen in 58/66 patients (88%). Of these, positive findings were found in 9/58 and negative in 49/58 patients with both methods. The agreement between the methods was substantial, with Cohen's kappa coefficient of 0.64. In the 8/66 patients with non-corresponding findings, 3/8 were positive only in BS and 5/8 only in ACE-PET/CT. Table II presents the agreement between ACE-PET/CT and BS on a per-patient basis in more detail. An example of ACE-PET/CT-positive/BS-positive suspected bone metastases from PC is illustrated in Figure 1.
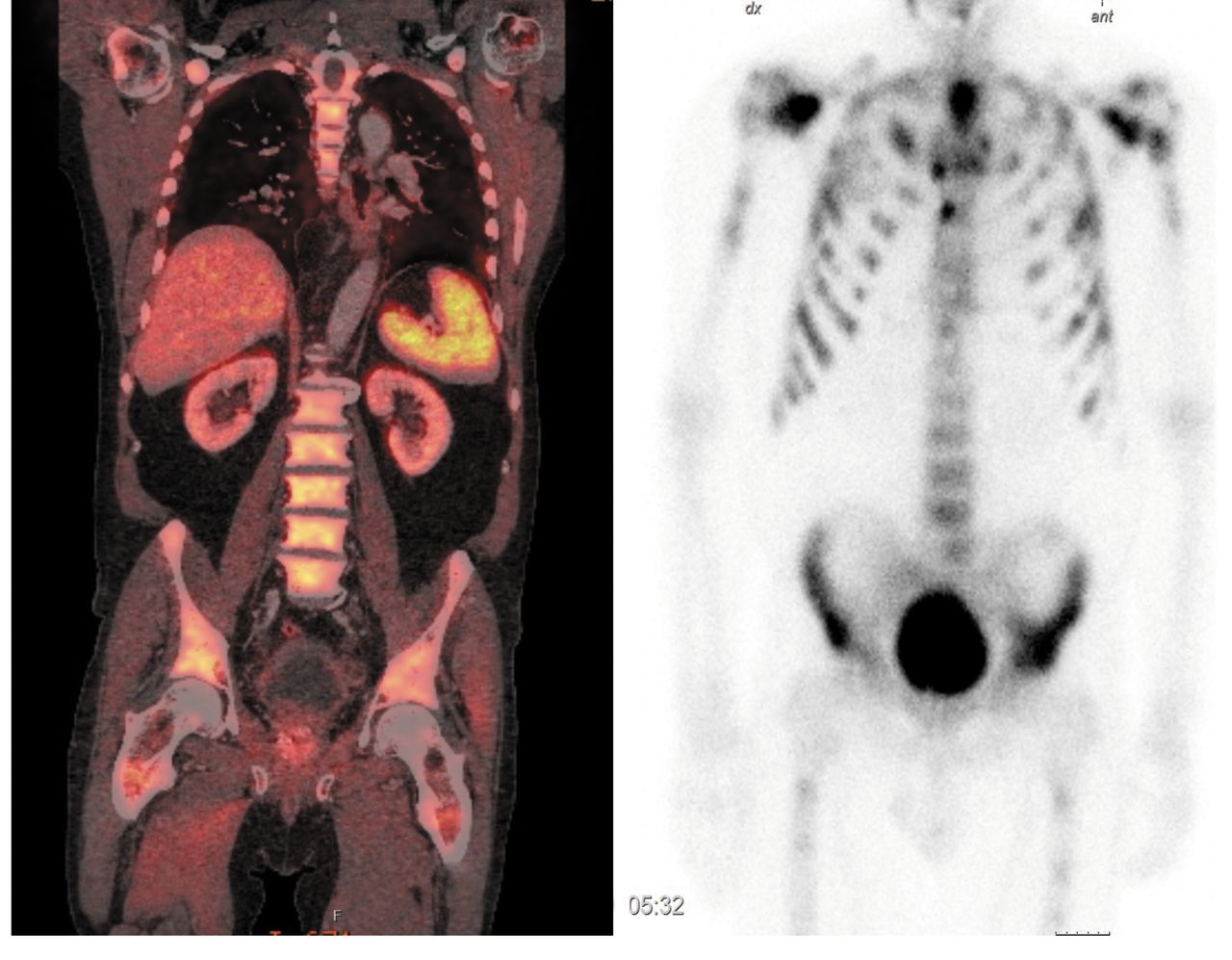
Generalized spread of bone metastases from prostate cancer as shown by increased 11C-acetate uptake in the vertebral column, pelvis, and proximal femur bilaterally in coronal fused 11C-acetate-positron-emission tomography/computed tomography (PET/CT) (left). Corresponding findings in anteroposterior planar 99mTc-hydroxymethylene diphosphonate bone scintigraphy are also shown (right). Please note that not all uptakes are shown, only an example from one 3.3 mm slice from the PET/CT.
Altogether 14/66 patients had ACE-PET/CT-positive findings suspicious of bone metastases. In 5/14 patients with ACE-PET/CT-positive findings, BS was negative. In three out of these five, partially matching sclerosis was found, and in two of these, suspected locoregional LN and extra-skeletal distant metastases were present, increasing the likelihood of bone metastasis. In one out of five, no sclerosis was found but locoregional and extra-skeletal distant metastases were suspected. In the remaining patient, there was no sclerosis and no other signs of metastasis.
Consensus decision resulted in suspected bone metastases in 4/5 ACE-PET/CT-positive/BS-negative patients. Follow-up at an average of 25 months (range=16-34 months) showed the interpretation was correct: four out of the five had bone metastases. One of the three patients with matching sclerosis had a 16-month imaging follow-up confirming the suspected bone metastases. The other two had no evident clinical progression of the in disease after treatment after 23 and 25 months of clinical follow-up. In the patient with no sclerosis but suspected locoregional and extraskeletal distant metastases, conventional imaging follow-up after 25 months showed no evident metastases but clinical symptoms supported the diagnosis of bone metastases. In the patient with no sclerosis and no other metastases, clinical follow-up for 34 months showed no sign of metastasis.
In 52/66 patients, ACE-PET/CT revealed no suspected bone metastases. Positive BS findings were seen in 3/52 of ACE-PET/CT-negative patients. Among these three patients, two had suspected locoregional LN metastases, increasing the likelihood of bone metastasis. In the remaining patients there were no other signs of metastasis but a solitary rib uptake on BS, which could be consistent with metastasis or rib fracture. Consensus decision resulted in suspected bone metastases in none of the three ACE-PET/CT-negative/BS-positive patients. Clinical follow-up for an average of 28 months (range=21-41 months) in these three patients showed no signs of metastasis, supporting the consensus decision was correct.
Added clinical value, defined as change in clinical management due to additional information from ACE-PET/CT, was found in 7/66 (11%) of the patients. In four out of these patients, previously undetected BS negative metastases were identified with ACE-PET/CT, and palliative treatment was offered after consensus decision. In three out of the seven patients, suspected metastases in BS were ruled out with ACE-PET/CT, and after consensus decision, curative treatment was offered.
ACE-PET/CT was significantly superior to planar BS in detecting suspected bone metastases in high-risk PC (p<0.01 with the Fischer exact test). Kappa values were 0.64 for ACE-PET/CT compared to BS, 0.95 for ACE-PET/CT compared to clinical follow-up and 0.66 for BS compared to clinical follow-up.
Discussion
BS is the current standard method for diagnosing bone metastases in PC (15). In our study, ACE-PET/CT gave a superior detection rate of suspected bone metastases in high-risk PC compared to planar BS. The follow-up data from the discordant cases showed ACE-PET/CT to be correct in the vast majority. The corresponding ACE-PET/CT and BS cases were considered true positive and true negative without follow-up. Consensus decision as well as follow-up data support the credibility of the ACE-PET/CT findings. Our results are in line with previous publications, such as the meta-analysis of BS, MRI and 11C-choline-PET/CT by Shen et al., which concluded that BS was the least specific and least sensitive modality (16). Another study showed better specificity but lower sensitivity for detection of bone metastases from PC with 11C-choline-PET/CT compared to BS (19). Whole-body MRI with diffusion-weighted imaging and [18F] fluoride-PET/CT have also proved superior to BS in high-risk PC (20), suggesting that more appropriate methods are available.
In our study, ACE-PET/CT gave added value in high-risk PC, with a change of clinical management in 11%. This is a surprisingly high number considering the built-in selection of patients, where those with unequivocal bone metastases in BS were excluded and only patients with a negative or inconclusive BS were referred for ACE-PET/CT according to clinical praxis. Despite this, we found positive findings in a cohort with low pre-test probability of bone metastases, indicating that ACE-PET/CT is more sensitive than expected. Patients can benefit from this both in terms of being offered more accurate, possibly curative, treatment options and in terms of avoiding side-effects and decline in quality of life from unnecessary or unhelpful therapy.
A built-in logistic advantage of PET/CT in PC imaging is to obtain all the N and M staging information in one examination, thereby improving patient comfort. Our results support that ACE-PET/CT might be a method of choice for both N and M staging in high-risk PC. In addition to metabolic functional information, PET/CT should preferably include a contrast-enhanced CT. We perform ACE-PET/CT with contrast-enhanced CT mainly to improve LN imaging but also because other visceral thoracic and abdominal processes are better depicted with i.v. contrast. Characterization of lesions should be carried out using the combined information from PET and diagnostic CT data. A clear methodological strength of our study is the hybrid imaging–hybrid reporting approach, whereby both PET and CT are performed at their best and then reported in a standardized manner by two experienced physicians, licensed in both radiology and nuclear medicine.
Another strength is the relative homogeneity of the group of study participants fulfilling the inclusion criteria. Most studies on ACE-PET/CT are in the recurrent setting. Our study adds useful information regarding primary staging of previously untreated PC.
One limitation of the study is its retrospective design. Our choice of endpoint parameter, the detection rate of ACE-PET/CT compared to BS, can be discussed. The ideal endpoint would be progression-free survival data; future studies will provide this information. Second best would be histopathological confirmation, which could not be obtained in this study. Confirmation of PET/CT findings with clinical follow-up data and consensus, best valuable comparator, instead of histopathology has been used in other comparative imaging studies in PC and is regarded as an established procedure for validation (21, 22). We chose not to verify our results with pre-treatment consensus in order to avoid circle evidence, since both ACE-PET/CT and BS results contributed to the final conclusion.
The 3-month time range allowed between BS and ACE-PET/CT adds some uncertainty since it cannot be excluded that positive findings may have developed between the examinations. However, as in other retrospective studies, we found this time range reasonable since the growth rate of PC metastases is relatively slow (22).
In conclusion, ACE-PET/CT gave a superior detection rate of bone metastases compared to planar BS in primary staging of high-risk PC. Follow-up data support the accuracy of ACE-PET/CT. ACE-PET/CT had a notable impact on clinical management. Long-term prospective studies are needed to confirm the present data and to evaluate the impact of ACE-PET/CT findings on progression-free survival.
Acknowledgements
This study was supported by the Umea University, Umea, Sweden Vasterbotten County Council (ALF) and Cancer Research Foundation Norrland.
The Authors thank Hans Stenlund who provided assistance in the statistical analyses.
Footnotes
This article is freely accessible online.
- Received October 12, 2016.
- Revision received October 26, 2016.
- Accepted November 1, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.