


Abstract
Background/Aim: Transanal endoscopic microsurgery (TEMS) is emerging as an alternative treatment for rectal cancer Stage I. There remains a risk of local recurrence. The Aim of the study was to study the effect of biomarkers in local recurrence for Stage I rectal cancer following TEMS plus or minus radiotherapy. Materials and Methods: This is a case control study where we compared 10 early rectal cancers that had recurred, against 19 cases with no recurrence, total 29 patients (age=28.25-86.87, mean age=67.92 years, SD=14.91, Male, N=18, Female, N=11). All patients underwent TEMS for radiological Stage I rectal cancer (yT1N0M0 or yT2N0M0) established with combination of magnetic resonance imaging (MRI) and endorectal ultrasound. We prospectively collected all data on tumour histology, morphological features, as well as follow-up parameters. Molecular analysis was performed to identify their status on BRAF, KRAS, p16 O6-methylguanine-DNA methyltransferase (MGMT) and β-catenin. Results: Out of 29 specimens analyzed, 19 were KRAS wild type (65.9%) and 10 mutant (34.5%). Recurrence of the tumour was noted in 10 cases (34.5%) from which 60% were pT1 (N=6) and 40% pT2 (N=4). There was a statistically significant association between KRAS mutant status and local recurrence (N=6, p=0.037). P16 expression greater than 5% (mean=10.8%, min=0, max=95) is linked with earlier recurrence within 11.70 months (N=7, p=0.004). Membranous β-catenin expression (N=12, 48%) was also related with KRAS mutant status (p=0.006) but not with survival (p>0.05). BRAF gene was found to be wild type in all cases tested (N=23). Conclusion: KRAS/p16/β-catenin could be used as a combined biomarker for prediction of local recurrence and stratification of the risk for further surgery.
The method of local excision, that has recently, gained wider acceptance, in early rectal cancer, is transanal endoscopic microsurgery (TEMS). TEMS generally offers advantages in operative access and oncological clearance over transanal resection (TAR), but recently a number of similar logic techniques with various rectal ports for endoscopic excision of rectal tumours has been invented. Those methods are collectively named transanal minimal-invasive surgery (TAMIS) and for oncological purposes they share the same features of local excision as TEMS (1-14).
TEMS is a minimally invasive technique that was introduced by Buess in the early 1980's (2). Through the new rectoscope with 3D binocular optic and the endoscopic instruments, it offers better access to proximal lesions with lower margin positivity and fragmentation and magnification of the operative field (2, 15). TEMS is a safe procedure that offers low complication rates and peri-operative morbidity (10.7%) (4). There have been multiple studies to suggest that TEMS is the operation of choice for rectal adenomas (1), retrorectal and submucosal rectal lesions (5). Furthermore, TEMS offers the advantage of not damaging the anorectal function (7).
TEMS is indicated as a curative treatment for malignant neoplasms that are histologically confirmed as pT1 sm1 carcinomas, whereas T1 sm2-3 and T2 lesions are still under question (8). A number of studies have shown that TEMS can have comparable results with radical surgery (1, 8, 12, 16) for rectal cancer.
There has been concern about oncologic outcomes following TEMS (17). Some studies support that there is potentially a higher risk of local recurrence rate with TEMS (8, 10, 18). Efforts have been made to classify risk with morphological and histological criteria with better patients' selection (1, 6-9); however, the risk stratification remains imperfect. Molecular biomarkers have been used in prognosis of colorectal cancer (CRC) in general and rectal cancer seems to follow the same genetic phenotype (19). So far, data in the literature, that link biomarkers and oncologic outcomes from TEMS, are limited.
Several biomarkers are being studied in CRC. Nevertheless, rectal cancer may have a specific profile of biomarkers, which is different to the rest of colonic cancer (20). Kohonen-Corish et al. (20) went through and analyzed a cohort of 381 rectal cancer specimens. The conclusion was that they identified a more aggressive subgroup arising from the KRAS-p16 pathway. This was explained by the fact that p16 deficiency and KRAS mutant status did promote carcinogenesis through the loss of oncogene-induced senescence. Therefore, p16 and KRAS could potentially be used as a prognostic biomarker in rectal cancer, which is against what is thought to be the case in sporadic colonic cancer.
We thus, aimed to identify whether any of the biomarkers KRAS, BRAF, p16, MGMT, β-catenin could be used as a prognostic factor to predict recurrence in early rectal cancer following local excision (TEMS).
Materials and Methods
Our institution performs TEMS for early rectal cancer after discussion at the Multi-Disciplinary Cancer meeting (MDT) according to UK national guidelines. All cases in this study have been operated by the same surgeon (senior author, SP). We prospectively collected data on histological parameters of the each lesion i.e. stage, differentiation, location, margins of resection and dysplasia where applicable. Preoperative staging of the tumours has been performed with magnetic resonance imaging (MRI) of the rectum and endorectal ultrasound (EUS), which are proven to have high diagnostic accuracy when combined (21-24). We have an established follow-up protocol for these patients with an intensive 5-year surveillance consisting of 6 monthly endoscopy, carcinoembryonic antigen (CEA), MRI scan and computed tomography (CT) scan for 3 years, which is altered to annual surveillance in years 4 and 5 (Table I).
We selected 10 patients who had recurrence after TEMS for early rectal cancer and we compared them in a case control study with 19 similar patients without recurrence. This was to assure we could compare the status of several biomarkers in non recurrent vs. recurrent lesions. Eighteen patients (62.1%) were male and 37.8% were female (N=11). Mean age at the stage of diagnosis, was 67.93 years (min=28.25, max=86.87). All the specimens were Stage I rectal cancer. Eighteen were pT1 (62.1%) and 11 pT2 (37.9%). There were no differences between the two groups.
Radiological staging has been performed both before and after radiotherapy. Neoadjuvant or adjuvant radiotherapy decision was based on fitness criteria, as well as patient choice. The option of further radical (completion) surgery has been offered in selected individualised cases as an option but was declined by the patients.
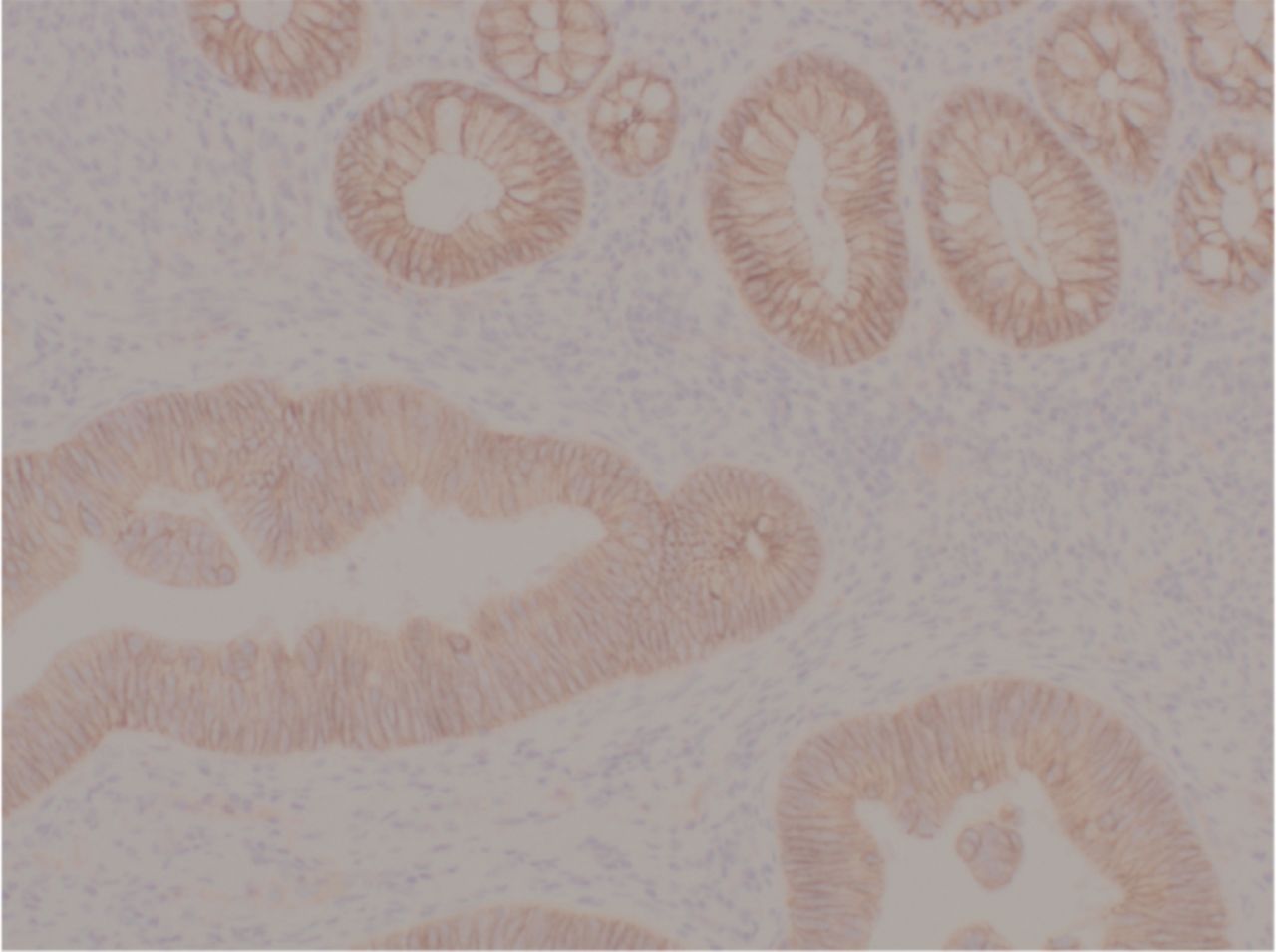
Biomarker analysis. All biomarkers were assessed on formalin-fixed, paraffin -embedded (FFPE) samples. Beta-catenin, mismatch repairs (MMRs), O6-methylguanine-DNA methyltransferase (MGMT) and p16 assays were performed using immuno-histochemistry (IHC). Four-μM sections of the tumour were cut on to coated slides and IHC was performed using standardised protocols for each antibody. The final step was visualisation of antigen-antibody complexes by the addition of the chromogen, diaminobenzidine. The slides were then assessed (by SDC and JM) and scored for percentage of positive tumour cells and protein location (Figures 1, 2, 3, 4 and 5).
KRAS mutation analysis was performed on the same tumour samples. Haematoxylin and eosin (H&E) stained sections of the tumour were assessed and marked for tumour content and the tumour was then macrodissected using serial, unstained section from the non-tumour components, allowing for enrichment of tumour cells. DNA was then extracted from these samples using standardised protocols and quantified by Qubit analysis. Polymerase chain reaction (PCR) using primers either side of the regions of interest, codons 12 and 13 and codon 61, was performed. After immobilisation of the resulting amplicons, single stranded DNA was prepared and the sequencing primer for each region was annealed. The samples were then analysed on a Qiagen Q24 pyrosequencer©, using the appropriate software (PyroMark Q24 software, version 2.07). The mutation status of each tumour was reported according to standard protocols (by SDC and JM).
Appropriate positive and negative controls were included for all assays. Photos have been obtained by JM with the relevant permission of Advanced Diagnostics Laboratory (King's Hospital NH Foundation Trust, London, Denmark Hill, UK).
Statistical analysis. Statistical analysis of our results was performed using IBM SPSS for Macintosh version 22 (IBM Corp., Armonk, NY, USA). We have performed bivariate correlations (Pearson's and Spearman's rho, as well as Chi-square associations) to identify any potential links between follow-up parameters and KRAS, BRAF, p16, β-catenin or MGMT.
Results
The mean overall follow-up period was 32.83 months (SD=23.02, min=12.96, max=126.9). From 29 patients, 19 did not have recurrence (65.5%), whereas 10 did have local recurrence of the rectal lesion (34.5%). The mean recurrence time was 13.04 months (min=4.11, max=42.28) (Table I).
From 29 patients, 79.3% (N=23) did not require further surgery, whereas 21.6% did (N=6). Twenty-five patients warranted TEMS procedure once (86%), whereas 1 patient required TEMS procedure twice (3.4%), 1 three times (3.4%) and 2 four times (6.8%). Decision to proceed with multiple TEMS was based on the fact that patients were unfit for radical surgery. Three patients (10.3%) received neoadjuvant radiotherapy (N=1 was pT1 and N=2 pT2), whereas 89.7% (N=26) did not receive. N=9 received further course of radiotherapy, based on the histology findings of unsuspected cancer and individualized decision to proceed with radiotherapy was made by the Multidisciplinary Team Meeting. Patients underwent short course radiotherapy; the regimen was 45-50Gy according to the local guidelines. All patients who had repeat TEMS surgery were elderly or unfit for major surgery and, therefore, the procedure was palliative (Table I).
Patients' characteristics, specimens' morphology, biomarkers' profile.
All the 29 specimens were Stage I out of which 62.1% were pT1N0 (N=18) and 37.9% were pT2N0 (N=11). This is based on radiological criteria. Completion of staging was performed with the rest of preoperative work up, including EUS, clinical assessment, CT abdomen-pelvis-thorax (TAP) and MRI of the pelvis and rectum. Almost one third (31.0%) did not have confirmed clear resection margins (N=9), whereas in the rest 69% (N=20), the margins were confirmed to be clear. The remaining tumours had margins obscured by the energy device artefact (Harmonic Ace and electro cautery) and were declared uncertain. There were no positive margins. Nineteen lesions (65.5%) were located in the lower rectum, 20.7% (N=6) in the mid rectum and 13.4% (N=4) in the upper rectum. Two (6.9%) were poorly differentiated adenocarcinomas, whereas 62.1% (N=18) were moderate differentiated and 31% (N=9) were well differentiated. The mean circumference of the tumour was 40.80% (min= 20%, max=75%). Greater than 33% circumference was found to be linked with mutant KRAS (p=0.00) (Table II).

Beta-catenin membranous. Original photo from KCH lab (J. Moorhead).

Beta-catenin membranous and nuclear. Original photo from KCH lab (J. Moorhead).
Nineteen of the specimens were KRAS wild type (65.5%) whereas 34.5% (N=10) were KRAS mutant (codon 12, 13 or 61). From the available BRAF results, 23 of the specimens were analysed and none was found to be positive for V600E mutation (wild type). From the MGMT point of view, 91% (N=23) were positive (preserved), whereas 8% (N=2) were negative (non-preserved). Four patients did not have available MGMT status (Table II).
From 29 specimens, 25 had available β-catenin status. Almost half (48%) were found to express membranous (m) status of β-catenin (N=12) (Figure 1), whereas 28% was found to express membranous and 30% nucleus (n) (N=7) (Figure 2), 10.3% m+50% n (N=3) and 10.3% only nucleus (N=3). All KRAS mutant tumours were linked with membranous β-catenin (N=8, p=0.009), whereas wild-type KRAS were spread between β-catenin m (N=3, 23.1%), m+30%n (N=7, 53.8%), m+50%n (N=3, 15.2%) and 100%n (N=1, 7.6%). Also membranous β-catenin was linked with more circumferential configuration of the tumour (p=0.028) but not with survival (p>0.05) (Figure 6).

P16 expression. Original photo from KCH lab (J. Moorhead).

P16 expression (higher %). Original photo from KCH lab (J. Moorhead).

P16 expression. Original photo from KCH lab (J. Moorhead).

Circumference vs. β-catenin expression.

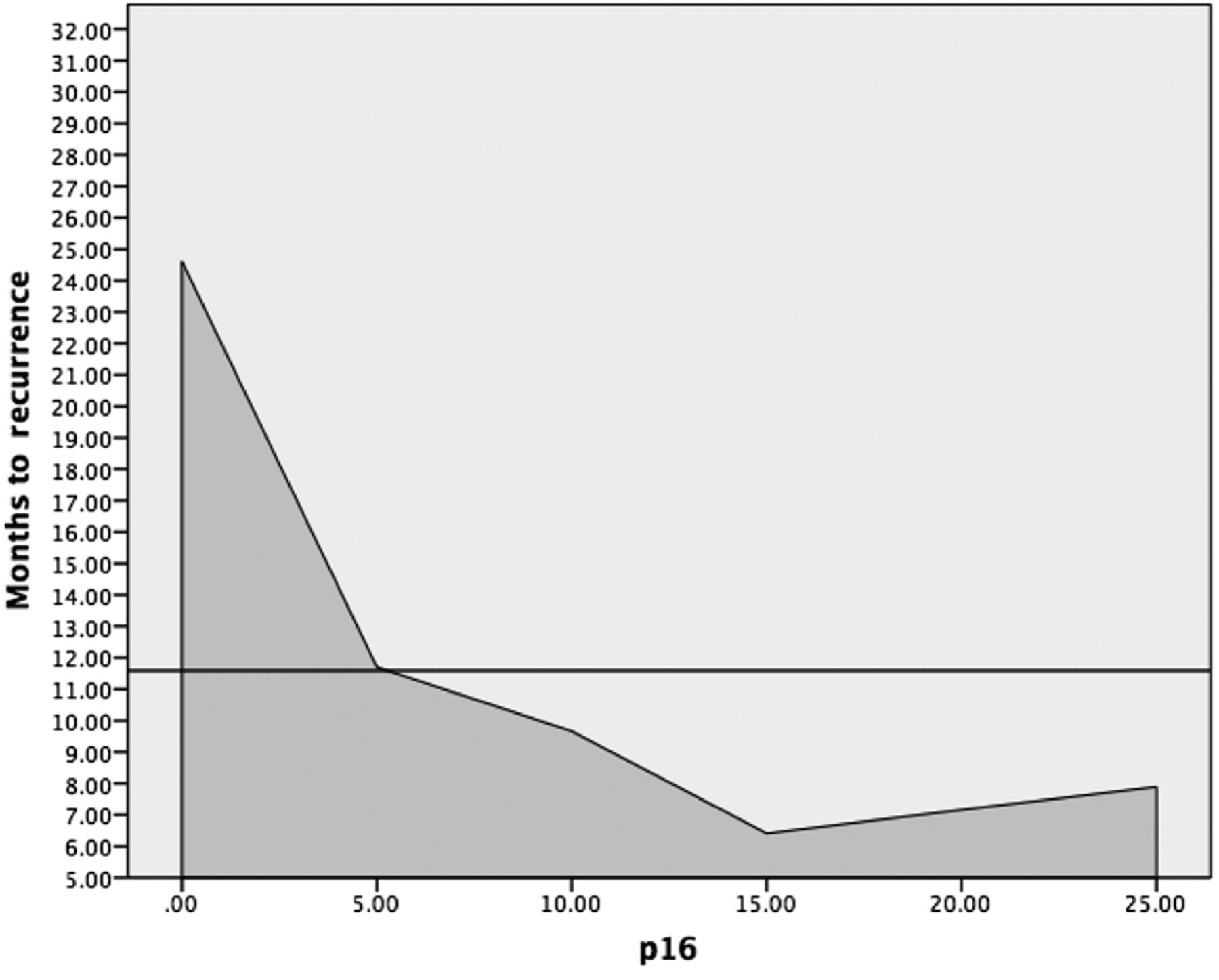
P16 in relationship with time of recurrence.
From our primary analysis, there was an association between mutant KRAS and local recurrence (p=0.037). From 10 specimens, which recurred, 60% were mutant for KRAS (N=6) and 40% wild type (N=4). Also, from 19 specimens with no recurrence, 79% (N=15) were wild type and 21% (N=4) KRAS mutant (Table III). There was no association between recurrence and p16 or β-catenin or MGMT status (p>0.05). Furthermore, local recurrence was not found to be associated with MRI pT stage, (p>0.05) or other morphological features of the tumour, including height, location, circumference and orientation (p>0.05). Local recurrence was not found to be associated with histological features of the specimens, i.e. pT stage, clear margins, dysplasia or differentiation (p>0.05). Moreover, there was no association between recurrence and neoadjuvant radiotherapy (p=0.123) (Table II).
The overall mass was calculated from the dimensions documented on the histology report (size 1 in mm × size 2 in mm × size 3 in mm). The overall mean mass of the specimens was 13,229.967 mm3 min=0.00 mm3, max=159,250.00 mm3, SD=28,706.9. The mean mass of the tumours that recurred was 25,776 mm3 (min=3,200 mm3 max=159,250 mm3, SD=47,375) compared to 6,626 mm3 (min=00 mm3, max=17,940 mm3, SD=5,121) for those that did not recur. There was a statistical significant relationship between the mass and recurrence of the lesions (p=0.028).
KRAS was found to be associated with β-catenin status (p=0.009) and, more specifically, mutant KRAS tends to be linked with membranous β-catenin (N=12, 41.9%). Also, KRAS mutant status is associated with the increased number of total TEMS (p=0.02). All wild-type KRAS (N=19) specimens have undergone a single operation, whereas 11.1% (N=1) of mutant had times 2 TEMS, 11.1% (N=1) times 3 and 22.2% (N=2) times 4. What is more, cancer-related death was noted in 6.9% (N=2) and was linked with KRAS mutant status (p=0.045). Discovery of unsuspected cancer was noted in 41.3% (N=12) and linked with mutant KRAS (N=7, p=0.023). However, there was no link between KRAS and dysplasia or differentiation of the specimen or clear margins or mass or pT stage or orientation of the specimen (p>0.05 for all associations, Table II).
Mean p16 expression was 10.8% (min=0.0%, max=75%). P16 expression more than 5% was linked with recurrence within the first 11.70 months (N=7, p=0.04) (Figure 7), though no other histological, morphological or phenotype association was identified (p>0.05) (Table II) (Figures 3, 4 and 5). Finally, MGMT status was found preserved in 92.0% (N=23) and non-preserved (negative) in 8.0% (N=2). All patients with MGMT negative results were aged above 80 years at the time of diagnosis (p=0.024) and pT2 (p=0.030). There was no other association noted between MGMT and morphological, histological or follow-up parameters (p>0.05) (Table II).
Discussion
There has long been an effort to link molecular biomarkers with prognosis in colorectal cancer but it still remains a poorly understood field. From our data, there seems to be a link between mutant KRAS and the risk of local recurrence of early rectal cancer after endoscopic local excision surgery TEMS. This is a previously unreported finding. We discuss here whether there may be a sound biological basis of this finding.
Significant associations.
KRAS and local recurrence.
Kirstein rat sarcoma viral sarcoma oncogene (KRAS), is a proto-oncogene involved in cellular response to extracellular stimuli, i.e. mitogen-activated protein kinase (MAPK) and phosphoinositide-3-kinase/v-akt murine thymoma viral oncogene pathways (PI3K/AKT) (25, 26). Therefore, KRAS mutations can potentially lead to activation of downstream signaling pathways, i.e. MAPK and PI3K/AKT. The latter is thought to lead to a higher resistance to anti-epidermal growth factor receptor (EGFR) inhibitors and, hence, this could be the etiology for increased resistance to anti-EGFR chemotherapy agents (27, 28).
KRAS mutations in codons 12, 13 and 61 are the most popular and tend to occur in 30-40% of CRCs. However, there have been noted 85 different KRAS mutations, many of which refer to a specific cancer pathway (8, 29).
So far, the prognostic and predictive value of KRAS gene in CRC has been debated, though it still remains controversial. There have been studies, which mainly support KRAS predictive value in response to anti-EGFR chemotherapy agents (27). More specifically, wild type KRAS is thought to be linked with better response to anti-EGFR agents, i.e. cetuximab, and this could be attributed to the relevant molecular mechanism described in the previous paragraph (28). Nevertheless, there are emerging data that KRAS predictive value in response to anti-EGFR inhibitors is controversial when BRAF gene appears to be mutant (V600E mutation) (30-32).
On the contrary, the prognostic value of KRAS in CRC remains equivocal. Most of the studies are inconclusive (29, 33) but there are some that associate KRAS mutant status with poorer prognosis (34).
Our study concludes that mutant KRAS may create a higher risk of local recurrence of early rectal cancer following TEMS. In our data, there is no association between local recurrence and pT stage or any other histopathological features (p>0.05); however, we need to keep in mind this is a small study not powered enough to test all possible factors. A recent study (35) supports that the frequency of KRAS mutant colorectal carcinomas is 35-40%, where in our case is 34.5%.
KRAS is also linked with some morphological features of the tumors and this can support its impact on the recurrence (35). Given the fact that a change in the genotype can directly reflect on the tumor phenotype, we can support that KRAS is linked with more circumferential configuration (p=0.000) and height of the lesion (p=0.030), as well as bigger mass (p=0.029).
BRAF V600E seems to be another valid prognostic biomarker in CRC. There is a link between BRAF V600E status and worse prognosis (36, 37) and BRAF V600E and more advanced cancer, being mostly present in right-sided tumours (38, 39). As discussed before, BRAF V600E has been found to interfere with KRAS occasionally. There are studies supporting that mutant BRAF status can affect response to anti-EGFR chemotherapy agents even in the presence of wild type KRAS (40, 41). All our specimens were BRAF wild type, where tested, and this could be explained by both the location, as well as earlier stage.
Another interesting finding in our data, is that p16 and MGMT are associated with older age (p=0.01 and p=0.024, respectively). Methylation of CpG islands (CpG island methylator phenotype (CIMP) and, specifically, O6-methylguanine-DNA methyltransferase (MGMT) gene promoter methylation) has been studied extensively in CRC (42, 43) and seems to have a recognized impact on the carcinogenesis pathway, though there is no consensus about its prognostic value (44). Loss of MGMT expression is found in 30-40% of metastatic CRC and results in the inability of the alkyl base to be removed from the methylated guanine and, hence, preservation of the DNA is not achieved (44).
With regards to the prognostic value of p16, there are studies correlating the methylation of p16 promoter with several clinicopathological features of CRC (45), i.e. TNM stage (p=0.006), lymph node metastasis (p=0.002), histologic grade (p<0.001), Dukes stage (p=0.002), tumour size (p=0.041) and location (p<0.001) Also, another study (46) shows that p16 methylation is found more in the serum of metastatic CRC patients. On our study, there is a link between p16 expression >5% and recurrence within 11.5 months (p=0.04). Furthermore, a recent cohort study (47) concludes that patients with advanced CRC, p16, human mutL homolog 1 (hMLH1) and MGMT methylation are associated with higher risk of recurrence, compared to patients with preserved unmethylated promoters.
Another interesting recent study (48) concludes that approximately 70% of KRAS-positive tumors are thought to have a CIMP characterized by aberrant methylation of the DNA of multiple genes, including p14, p15, p16. Therefore, this could be used as a link between KRAS status and p16 expression, especially in different stages of the cancer pathway.
In terms of the β-catenin significance, there seems to be a link between KRAS mutant status and membranous β-catenin (N=8, p=0.09). This is fairly interesting as it connects two different pathways of the carcinogenesis pathway together. Beta-catenin seems to belong to a different signalling pathway (wnt/β-catenin) and its significance in CRC remains equivocal. Beta-catenin is a pivotal molecule involved in intercellular adhesion and some other oncogenic and developmental processes (49). The same study links the up-regulation of β-catenin with the confrontation of tumour cells in the host microenvironment, whilst in metastatic process. However, its role in CRC remains unclear. In our study, membranous β-catenin is linked with higher circumference of the tumor (p=0.028, Figure 6). This supports again a joint role with mutant KRAS status as the latter is linked with higher circumference as well. An interesting study (50) in lung cancer concludes that combinational activation of KRAS and wnt/β-catenin pathway leads to a significant increase on the lung tumour formation and, therefore, worse prognosis effect.
With regards to the decision for further neoadjuvant radiotherapy, no relationship was identified between the decision for neoadjuvant radiotherapy and our potential biomarkers, i.e. KRAS, BRAF, MGMT, β-catenin and p16 (p>0.05 for all associations).
On the other hand, we still recognize some limitations of our study, mainly due to small sample size of our cohort. Nevertheless, as recurrence early rectal cancer after local excision is rare, with average numbers around 10%, it is not easy to form a much larger study than this. However, we consider our findings adequate to propose that KRAS, p16 expression and β-catenin status should be looked further as a potential combined biomarker system to assess the risk of local recurrence. Mutant KRAS was found to be more associated with local recurrence and with unsuspected cancer in the specimen (p=0.023) (when the initial tumor was thought dysplastic). Membranous β-catenin tends to be linked with mutant KRAS as well. P16 expression is associated with earlier recurrence, something that could re-direct the focus of the 5-year postoperative surveillance protocol if confirmed.
In conclusion, the biomarkers KRAS/p16/β-catenin could be used as a combined biomarker for prediction of local recurrence and stratification of the risk for further surgery. Further research based on multicentre cohort samples, should be conducted to confirm these findings, and improve our understanding on the actual effect of those biomarkers in the recurrence of early rectal cancer, after local excision.
Footnotes
This article is freely accessible online.
Funding
Internal (Departmental) funding was used to support this project, Part of MD(Res) Thesis at King's College London.
Conflicts of Interest
The Authors declare no conflict of interest.
- Received August 11, 2016.
- Revision received August 24, 2016.
- Accepted August 26, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Role of KRAS in Endometrial Cancer: A Mini-Review
- Radiotherapy May Offer a Recurrence and Survival Benefit in Rectal Cancers Treated Surgically with Transanal Endoscopic Microsurgery: A Systematic Review and Meta-analysis
- KRAS Mutant Status May Be Associated with Distant Recurrence in Early-stage Rectal Cancer