


Abstract
Background: The aim of the present study was to clarify the outcome of living donor liver transplantation (LDLT) in patients with hepatocellular carcinoma (HCC) within Milan criteria. Patients and Methods: The study comprised of 197 adult patients. One hundred twenty-nine patients were within Milan criteria. The overall and recurrence-free survival rates after the LDLT were calculated. Results: The 1-, 5- and 10-year overall survival rates were 94.5%, 89.9% and 88.6%, respectively. The 1-, 5- and 10-year recurrence-free survival rates were 100%, 97.0% and 94.0%, respectively. Four patients had HCC recurrence. The mean neutrophil to lymphocyte ratio (NLR) (6.75 vs. 2.75, p=0.002) or alpha-fetoprotein (AFP) (3,239 vs. 197, p<0.001) of these four recipients was significantly higher compared to that of 125 recipients without HCC recurrence. Conclusion: The outcome of LDLT for patients with HCC within Milan criteria was outstanding. Careful follow-up after LDLT is necessary for patients with high NLR or AFP.
Hepatocellular carcinoma (HCC) is the fifth most common neoplasm worldwide and the third most common cause of cancer-related death. Its incidence is increasing because of the dissemination of hepatitis B and C virus infection. Liver transplantation (LT), which offers the theoretical advantage of removing both the tumor and the organ at risk of developing future malignancy, is an established therapy for HCC in patients with liver cirrhosis (1, 2). In Asian countries, religious, cultural and political ideologies have created significant obstacles to the transplantation of cadaver organs. Organ shortages have forced patients with HCC to endure long waiting periods that are associated with tumor development. Thus, living donor LT (LDLT) is a choice for treating such patients after various treatments, such as radiofrequency ablation (RFA), transarterial chemoembolization (TACE), with/without hepatic resection (3).
The Milan criteria (MC) have significantly improved the outcome of LT for HCC (4) and have become the gold standard for achieving favorable outcome after LT for HCC. We have reported expanded criteria used because the favorable outcomes have raised the question of whether selection criteria might be expanded (5, 6). Since Japanese national insurance started to cover LDLT for HCC within the MC in 2004, the number of LDLT patients within the MC is increasing. Poor recipient status, partial hepatic graft use, or uncontrollable infection due to immunosuppression in LDLT can cause patient death without HCC recurrence in contrast to other treatment modalities for HCC (7). Thus, it is important to investigate current outcomes of LDLT for patients within the MC.
The aim of the present study was to clarify the outcomes for HCC recurrence and mortality after LDLT in patients who met the MC.
Patients and Methods
Patients. One hundred and ninety-seven adult patients underwent LDLT for end-stage liver disease with HCC at the Kyushu University Hospital between April 1999 and March 2015. Pre-transplant imaging study revealed that 129 patients were within the MC and 68 were not. Among 129 patients within the MC, 19 recipients underwent LDLT for indications other than HCC but were included in the study as HCC was found on explant pathology. Among 197 patients, no patient was excluded from the study. One hundred and twenty-seven patients underwent pre-transplant treatment for HCC, such as RFA, TACE, microwave coagulation therapy, with/without hepatic resection depending on the patient's liver function and tumor status. Graft types included left lobe with caudate lobe graft (LL+C; n=118), right lobe graft without the middle hepatic vein (n=72), posterior segment graft (n=6), and dual graft (n=1). The etiology of liver cirrhosis was hepatitis C (n=137), hepatitis B (n=34), cryptogenic (n=9), alcohol abuse (n=7), autoimmune hepatitis (n=4), primary biliary cirrhosis (n=4), non-alcoholic steatohepatitis (n=2) (Table I). Our selection criteria for performing LDLT for patients with HCC were as follows: (i) no modality except LDLT available for cure of HCC; (ii) no extrahepatic metastases; and (iii) no major vascular infiltration (5). There were no restrictions on tumor size, number of nodules, or pre-transplant treatment. Since we proposed our own criteria (5), we did not perform LDLT for patients with HCC with both tumor size exceeding 5 cm and des-γ-carboxy prothrombin (DCP) level exceeding 300 mAU/ml.
Characteristics of patients and donors (n=197) in this study.
Pre-transplant imaging was used to estimate the maximum tumor size and number of nodules. Alpha-fetoprotein (AFP), DCP and the neutrophil to lymphocyte ratio (NLR) were measured just prior to LDLT. The histological grades obtained from the explanted livers were used for determining tumor differentiation and the presence of vascular invasion.
Donor and graft selection. Donors were selected from candidates who hoped to be living donors (6, 8). Donors were required to be up to/including a third degree blood relative of the recipients, or spouses, and to be between 20 and 65 years of age. For a any other donor, individual approval was obtained from the Ethics Committee of the Kyushu University Hospital. Good Samaritan donations were not used.
Eligible donors proceeded to the imaging studies, including chest and abdominal X-rays and 3-mm-slice computed tomography (CT) for graft volumetric analysis. Three-dimensional CT was introduced for volumetric analysis and delineation of vascular anatomy. The standard liver weight (SLW) of recipients was calculated according to the formula of Urata et al. (9). Graft weight (GW) was predicted by CT volumetric analysis. Our decision about graft type for recipients was based on the preoperatively predicted GW to SLW ratio. LL+C graft was used when the preoperatively predicted GW to SLW ratio was ≥35%. When the GW to SLW ratio with LL+C graft was <35% and remnant donor liver volume after right lobectomy was ≥35%, right lobe graft was used. Posterior segment graft was considered when the donor's vascular anatomy was suitable for taking a posterior segment (10).
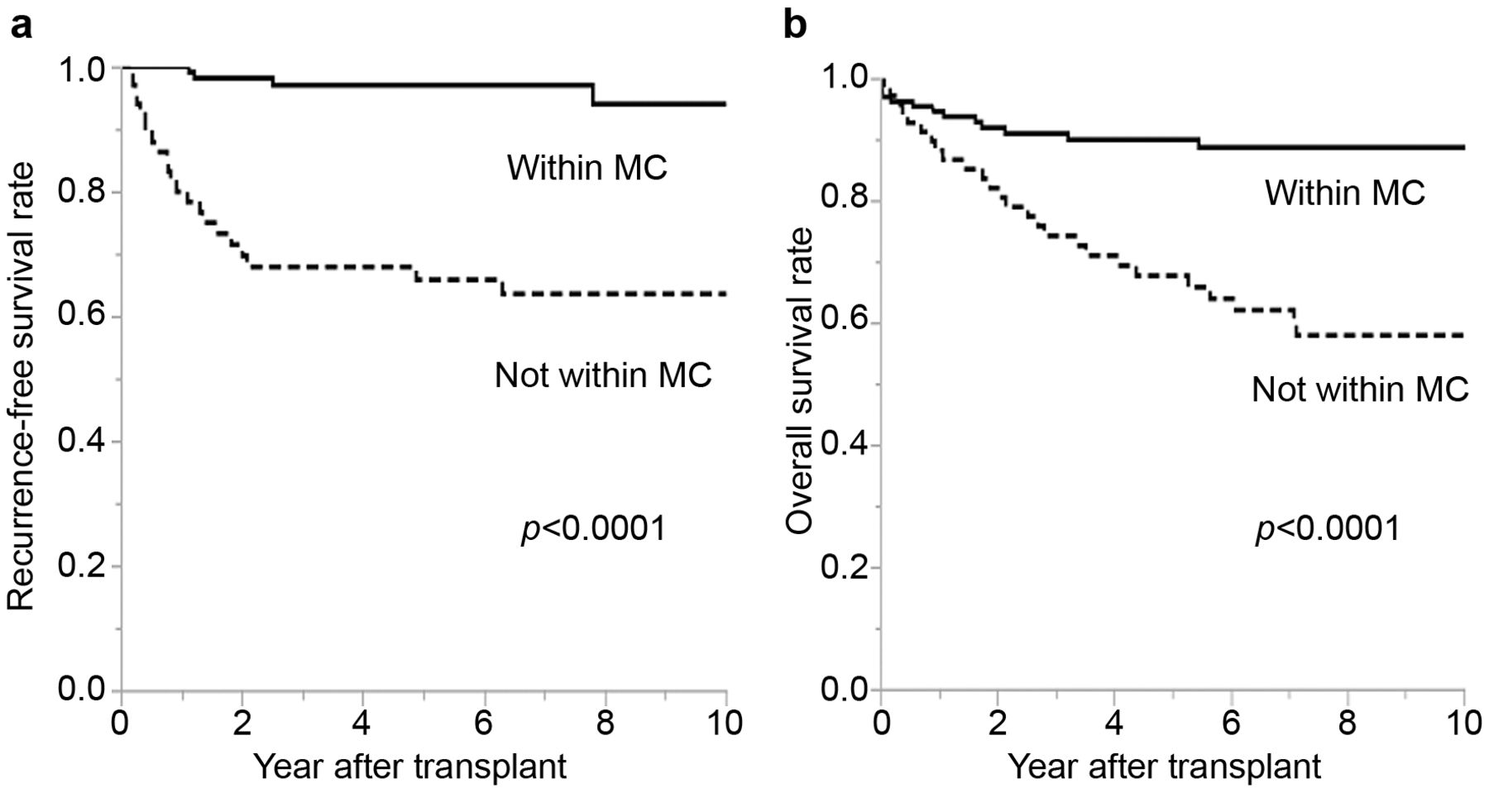
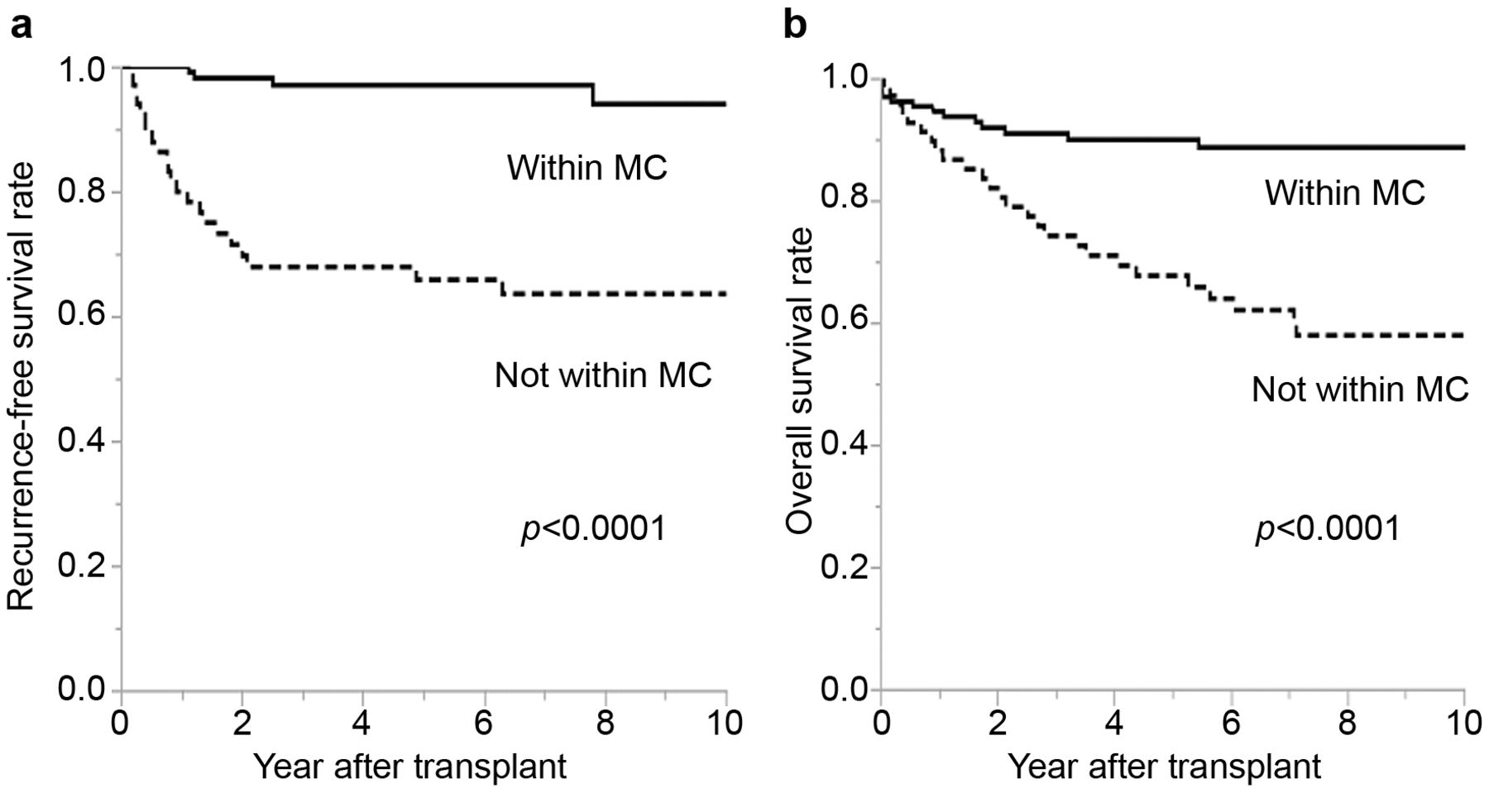
Recurrence-free survival and overall survival after LDLT: living donor liver transplantation for hepatocellular carcinoma. Recurrence-free (a) and overall (b) survival of transplant recipients divided according to whether they were within or not within Milan criteria (MC).
Postoperative management. The graft retrieval technique, recipient surgery and perioperative management of the recipients, including immunosuppression regimens have been described previously (11). Immunosuppression was initiated using a protocol based on either tacrolimus (Prograf; Astellas Pharma Inc., Tokyo, Japan) or cyclosporine A (Neoral; Novartis Pharma K.K., Tokyo, Japan) with steroid with/without mycophenolate mofetil (MMF; Chugai Pharmaceutical Co. Ltd., Tokyo, Japan). Tacrolimus was used for 100 recipients, and cyclosporine for 91 recipients. Six recipients did not receive calcineurin inhibitor due to poor postoperative course. A target trough level of tacrolimus was set at 10 ng/ml for 3 months after LDLT, followed by 5-10 ng/ml thereafter. A target trough level of cyclosporine A was set at 250 ng/ml for 3 months after LDLT, followed by 150-200 ng/ml thereafter. Methylprednisolone was initiated on the day of LDLT, tapered and converted to prednisolone 7 days after LDLT. Prednisolone treatment was tapered and discontinued 6 months after LDLT. MMF was used for 177 recipients and was started at 1-2 g/day on the day after LDLT, tapered and discontinued until 6 months after LDLT. A trough level was not measured for MMF.
All patients had monthly follow-ups, and the median follow-up period was 2,231 days, with 782 days and 3448 days as the 25th and 75th percentiles, respectively.
Post-LDLT tumor recurrence. HCC recurrence after LDLT was set as the primary end-point. Tumor recurrence was defined when any imaging studies, such as chest or abdominal CT scan, or bone scintigraphy revealed recurrence of HCC. Recurrence-free survival was defined as the time period between LDLT and tumor recurrence. Recipient mortality after the LDLT was set as the secondary end-point. Overall survival was defined as the time period between LDLT and recipient death.
Statistical analysis. Recurrence-free and overall survival rates were calculated by the Kaplan–Meier product-limited method. Data are expressed as means. All statistical analyses were performed using JMP 9.0 software (SAS, Inc., Cary, NC, USA). A p-value of <0.05 was considered significant.
Results
The characteristics of the present patients and donors are shown in Table I. More female patients were included within the MC. Patients within the MC had higher model for end-stage liver disease (MELD) score. Simultaneous splenectomy was performed more frequently in patients within the MC. Right lobe or posterior graft was used more frequently in recipients within the MC. The pre-transplant AFP or DCP level was lower in patients within the MC, whereas the pre-transplant NLR was not different between the two groups. Pre-transplant treatment for HCC was more frequently performed in patients not within MC. Microvascular invasion on explant pathology was more frequently revealed in patients not within MC as was poor pathological tumor differentiation. Pathological examination revealed 39 livers (30.2%) were not within MC in patients defined as within the MC by pre-transplant imaging, while in contrast, nine livers (13.2%) were within the MC in patients not within MC pre-transplant.
Characteristics of four patients within Milan criteria who had hepatocellular carcinoma recurrence after living donor liver transplantation (LDLT).
The 1-, 5-, and 10-year recurrence-free survival rates for patients within MC were 100%, 97.0% and 94.0%, respectively. In contrast, those in patients not within MC were 79.9%, 65.8% and 63.5%, respectively (p<0.0001, Figure 1a).
Four out of the 129 patients within MC had HCC recurrence after LDLT. Detail id data of these four patients are shown in Table II. Patient 1 had HCC recurrence 7.8 years after LDLT due to uncontrollable hepatitis C virus (HCV) recurrence. Therefore, this recurrence was believed to be de novo HCC. Patients 2 and 3 had high pre-transplant NLR. Furthermore, patient 4 had high pre-transplant AFP and DCP levels. The mean NLR of these four patients was significantly higher compared to that of 125 patients without HCC recurrence (6.75 vs. 2.75, p=0.002). Additionally, the mean AFP level of these four patients was higher compared to that of 125 patients without HCC recurrence (3,239 vs. 197 ng/ml, p<0.001). Other variables, including DCP, were not statistically different between the group with HCC recurrence and that with no recurrence.
The 1-, 5-, and 10-year overall survival rates for the patients within MC were 94.5%, 89.9% and 88.6%, respectively. In contrast, those for the patients not within MC were 88.1%, 67.6% and 57.8%, respectively (p<0.0001, Figure 1b).
Characteristics of 13 recipients within Milan criteria who died after living donor liver transplantation (LDLT).
Thirteen out of the 129 patients within MC died within 10 years after LDLT. Causes of death were HCV recurrence (n=3), cerebral hemorrhage (n=2), hepatic graft failure (n=2), accident (n=2), HCC recurrence (n=1), sepsis (n=1), blood loss during LDLT (n=1), and sudden death of unknown origin (n=1) (Table III).
Discussion
LT is an effective treatment for HCC when disease is defined by the widely accepted MC (12). Transplantation for patients within MC generally leads to a 5-year overall survival rate of 70 to 80% and a recurrence rate of around 10% (13). In other words, 10% of patients even within MC have HCC recurrence and 20% of patients would die within 5 years after LT. It is important to consider the ethical aspects of transplanting using living donors. Donor safety is the paramount concern in any donor surgery in LDLT. The risk to the donor must balance the benefit to the donor in terms of survival of the recipient (14). The final goal of LDLT is to achieve patient survival as long as possible.
It is of great interest that only one patient among 129 patients within MC died due to HCC recurrence after LDLT in the present study. This patient underwent microwave coagulation therapy, TACE and radiation for HCC and had high AFP and DCP levels before LDLT. Multiple lung metastases were revealed 1.2 years after LDLT. This means that the patient had micrometastases in the lung before LDLT. When patients within MC have extremely high levels of tumor markers, distant micrometastasis rather than poor tumor behavior of the original liver tumor might be suspected. The other three patients with recurrence are alive after successful surgical resection for liver, bone or lymph node metastasis. Similarly to a previous report, surgical resection is useful for recurrent HCC in order to improve the outcome, when resection is feasible (15).
It is well-known that systemic inflammation is strongly associated with patient prognosis. The NLR has recently emerged as a useful prognostic factor for recurrence of several gastroenterological malignancies. It has been demonstrated that a preoperatively elevated NLR is an adverse predictor of recurrence-free survival for patients undergoing hepatic resection for HCC (16). Furthermore, an elevated NLR significantly increases the risk of HCC recurrence after LT (6, 17). Pre-transplant NLR in two patients was elevated and the mean NLR of four patients who had HCC recurrence was significantly higher than that of 125 recipients without HCC recurrence. There are several possible mechanisms to explain the predictive role of preoperatively elevated NLR (18). Infiltration of proinflammatory macrophages, cytokines, and chemokines in the tumor microenvironment can boost tumor growth, invasion, and metastasis (19, 20). Furthermore, high expression of granulocyte colony-stimulating factor in tumor tissue and macrophage colony-stimulating factor in peritumoural tissue are associated with an increase in circulating neutrophils and poor prognosis (21). Halazun et al. showed that an elevated NLR is correlated with microvascular invasion and poorly differentiated tumor (22). The results of the present study were inconsistent with previous findings due to the small number of patients with recurrence. An elevated NLR in patients within MC could be a marker of distant metastasis, similarly to AFP and DCP. Several studies have suggested the benefit of adjuvant chemotherapy after LT for advanced HCC (23-25). Patients within MC with elevated NLR, AFP or DCP would be candidates for adjuvant chemotherapy after LT. Further study is needed because agents for chemotherapy for treating HCC are not well established.
HCV infection is the leading indication for LT worldwide. One patient in the present study had de novo HCC 7 years after LDLT and three patients died due to interferon treatment failure for HCV. After LT, HCV recurrence is universal among patients with viremia before LT (26) and is the leading cause of death in LT recipients. The standard care for the treatment of recurrent HCV after LT was peg-interferon with ribavirin, although with response rates of only 13 to 43% (27). In addition, interferon-based therapies can induce alloimmune graft injury, reducing patient survival (28). Recent advances of an interferon-free, direct-acting anti-viral (DAA) regimen seems to be able to change the fate of such patients. Such a multi-targeted DAA regimen resulted in a 97% sustained virological response rate for patients with HCV recurrence after LT (27).
In conclusion, the outcome of LDLT for patients with HCC within MC was outstanding. Careful follow-up after LDLT is necessary for patients with a high NLR or AFP level. An increase in NLR or AFP suggests distant micrometastasis before LDLT which might need adjuvant systemic chemotherapy.
Footnotes
Funding
This study was partly funded by Grant-in-aid (Grant 26506013) from the Ministry of Education, Science, and Culture in Japan.
Conflicts of Interest
The Authors declare no conflicts of interest.
- Received October 30, 2015.
- Revision received December 4, 2015.
- Accepted December 7, 2015.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.