


Abstract
Background/Aim: The rupture of hepatocellular carcinoma (HCC) is defined as a detrimental staging factor. The aim of the present study was to elucidate whether the prognosis of surgical patients with ruptured HCC was truly appalling. Patients and Methods: The data obtained from the medical records of 1,031 patients who underwent primary R0 hepatecomy for HCC between August 2003 and November 2014 at the Department of Surgery and Science, Kyushu University Hospital and its two affiliated hospitals, were retrospectively analyzed. Twenty-seven patients had ruptured HCC. Results: The recurrence-free and overall survival for patients with ruptured HCC were favorable. All 19 patients with ruptured HCC who experienced recurrence had intrahepatic recurrence, while only three had peritoneal recurrence. The multivariate risk factor analyses showed that rupture itself was not relevant to recurrence-free survival nor to overall patient survival. Conclusion: Rupture itself does not have much relevance to the outcome for patients who undergo hepatectomy.
Rupture of hepatocellular carcinoma (HCC) has lately become a rare event because of the advancement of screening for patients with risks for developing HCC (e.g. hepatitis B or C) (1). However, we still occasionally encounter patients with ruptured HCC in an emergency situation. Although bleeding from ruptured HCC can be controlled by transarterial embolization/chemoembolization (TAE/TACE) in most cases (2, 3), TAE/TACE rarely leads to complete tumor necrosis. We actively performed hepatectomy for ruptured HCC whenever a complete resection was achieved because it would lead to a better prognosis (4-9). Rupture itself has been considered a factor indicating worse prognosis and is defined as T4 in the staging system issued by the Liver Cancer Study Group of Japan (LCSGJ) (10), as well as the system issued by the Union for International Cancer Control (UICC) (11). Recently, Aoki et al. reported that rupture itself did not mean a worse prognosis, by analyzing 1,160 cases from a nationwide survey in Japan, and suggested that the current staging system should be reconsidered with regard to ruptured HCC (12). In our experience during the past decade, patients who underwent hepatectomy for ruptured HCC were able to tolerate the operation well, thanks to advancement in perioperative managements, diagnostic procedures and intervention techniques for patients with HCC, as other investigators reported (2, 13). Furthermore, contrary to our expectations, peritoneal recurrence was rarely found after complete resection of ruptured HCC. Therefore, we conducted a retrospective analysis of outcomes of hepatectomy for ruptured HCC that were performed at the Department of Surgery and Science, Kyushu University Hospital and its two affiliated hospitals during the past 12 years.
Patients and Methods
The data obtained from the medical records of 1,031 patients who underwent R0 hepatectomy as a primary curative therapy for HCC between August 2003 and November 2014 at the Department of Surgery and Science, Kyushu University, and its two affiliated hospitals were retrospectively analyzed. This study was approved by the Institutional Review Board of Kyushu University (no. 27-151). All resected specimens were pathologically diagnosed with HCC. The stage for each individual was determined clinically by preoperative imaging and operative findings. Indications for hepatectomy and surgical procedures were as previously reported (14, 15). The two current staging systems for HCC (LCSGJ and UICC) were used in the current analyses (Table I). Because classification of the stage IV A by LCSGJ consists not only of patients with ruptured HCC but also those with advanced HCC (multiple tumors with vascular invasion, any of which more than 2 cm), we divided this stage into advanced-stage IV A [stage IV A (A)] and ruptured stage IV A [stage IV A (R)] in order to clarify the impact of tumor rupture on patient outcomes. The numbers of patients in each stage were as follows: By LCSGJ: stage I, 201; stage II, 508; stage III, 246; stage IV A (A), 49; and stage IV A (R), 27; and by UICC: stage I, 646; stage II, 259; stage III A, 64; stage III B, 35; and stage III C, 27.

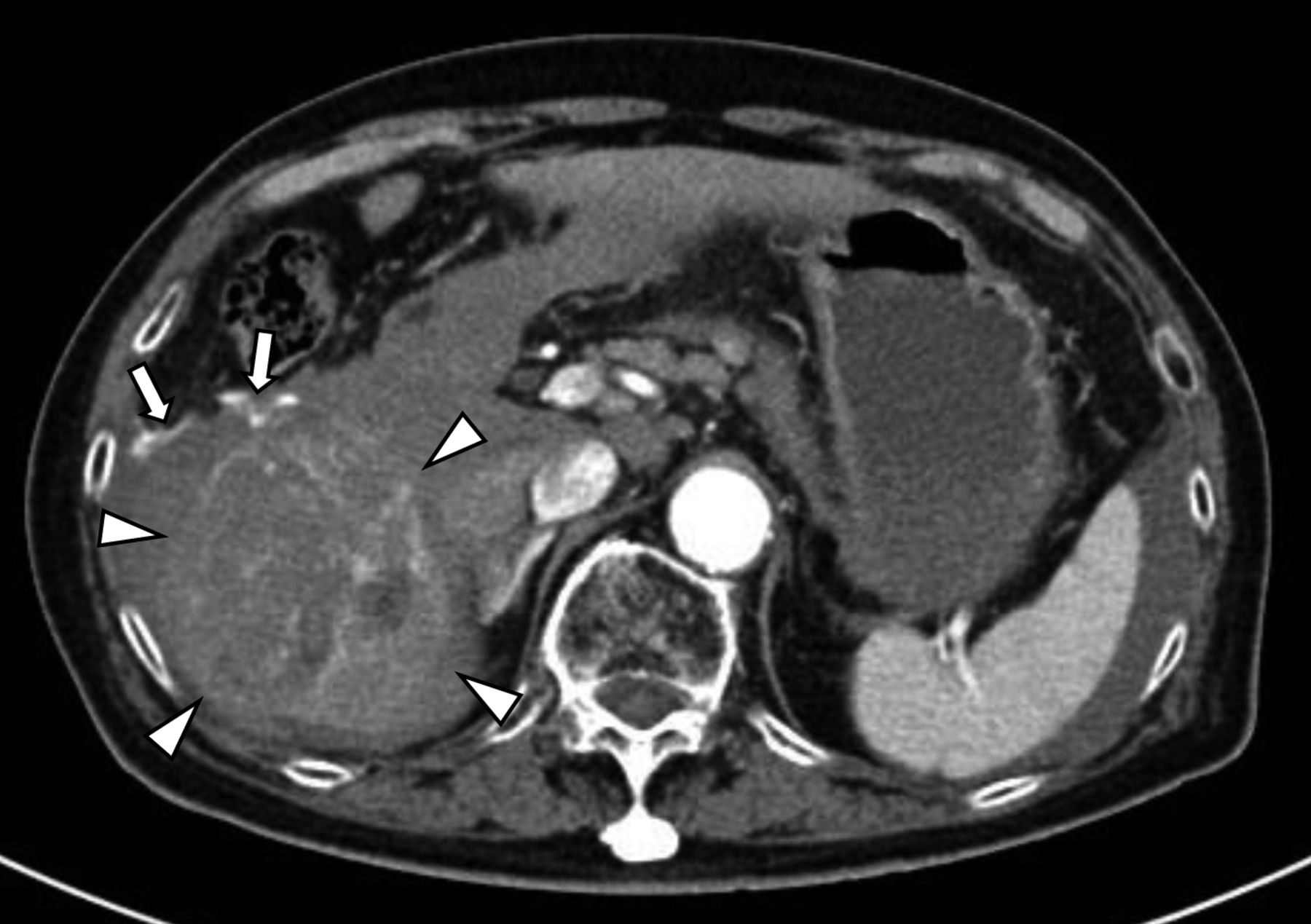
A representative computed tomographic image of ruptured hepatocellular carcinoma. Arrow heads indicate a contrast-enhanced hepatocellular carcinoma located in the lower portion of the right lateral sector of the liver. Arrows indicate extravasation of contrast medium.
The diagnosis of rupture was made when there was any extravasation of contrast media on contrast-enhanced computed tomography (CT) or angiography or hematoma around the liver (Figure 1). Thirteen out of 27 patients with ruptured HCC were admitted in a state of hypovolemic shock. Twenty-one out of the 27 patients were initially treated by TACE in order to control bleeding and stabilize their condition, thereafter they underwent staged hepatectomy. The median length of time between the TACE and surgury was 24 days (range=9-104 days). The other six patients underwent hepatectomy without TAE/TACE because of their stable condition on admission.
The patients were postoperatively followed-up by CT or magnetic resonance imaging (MRI) at intervals of approximately 3 months for detecting tumor recurrence. The intervals were modified according to the patient's condition. Dates of recurrence were defined as the date when a CT or an MRI image showed typical features of HCC. The censor date was set at November 30, 2014. Statistical analyses. Survival statistics were calculated by a Kaplan–Meier analysis and survival curves were compared using a log-rank test. Multivariate Cox regression tests were performed on variables found to be statistically significant by the univariate analyses. Proportions were compared using χ2 test. Statistical significance was defined as having a p-value, derived from a two-tailed test, of less than 0.05. All statistical analyses were performed using the NCSS 9 software package (16).
Results
Recurrence-free survival and overall survival according to the LCSGJ staging system. Figure 2 shows the recurrence-free and the overall survival according to the LCSGJ staging system. The median recurrence-free survival durations in stage I, II, III, IV A (A) and IV A (R) were 1,394, 933, 526, 196 and 433 days, respectively. The patients with stage IV A (R) HCC tended to experience better recurrence-free survival than did the patients with stage IV A (A) (p=0.078). The recurrence-free survival of patients with stage IV A (R) was comparable to that of those with stage III. The median overall survival durations in stage II, III, IV A (A) and IV A (R) were 3,977, 2,353, 868 and 1,563 days, respectively. The patients with stage IV A (R) HCC tended to experience better survival than those with stage IV A (A) (p=0.064). The overall survival of patients with stage IV A (R) was almost comparable to that of patients with stage III.
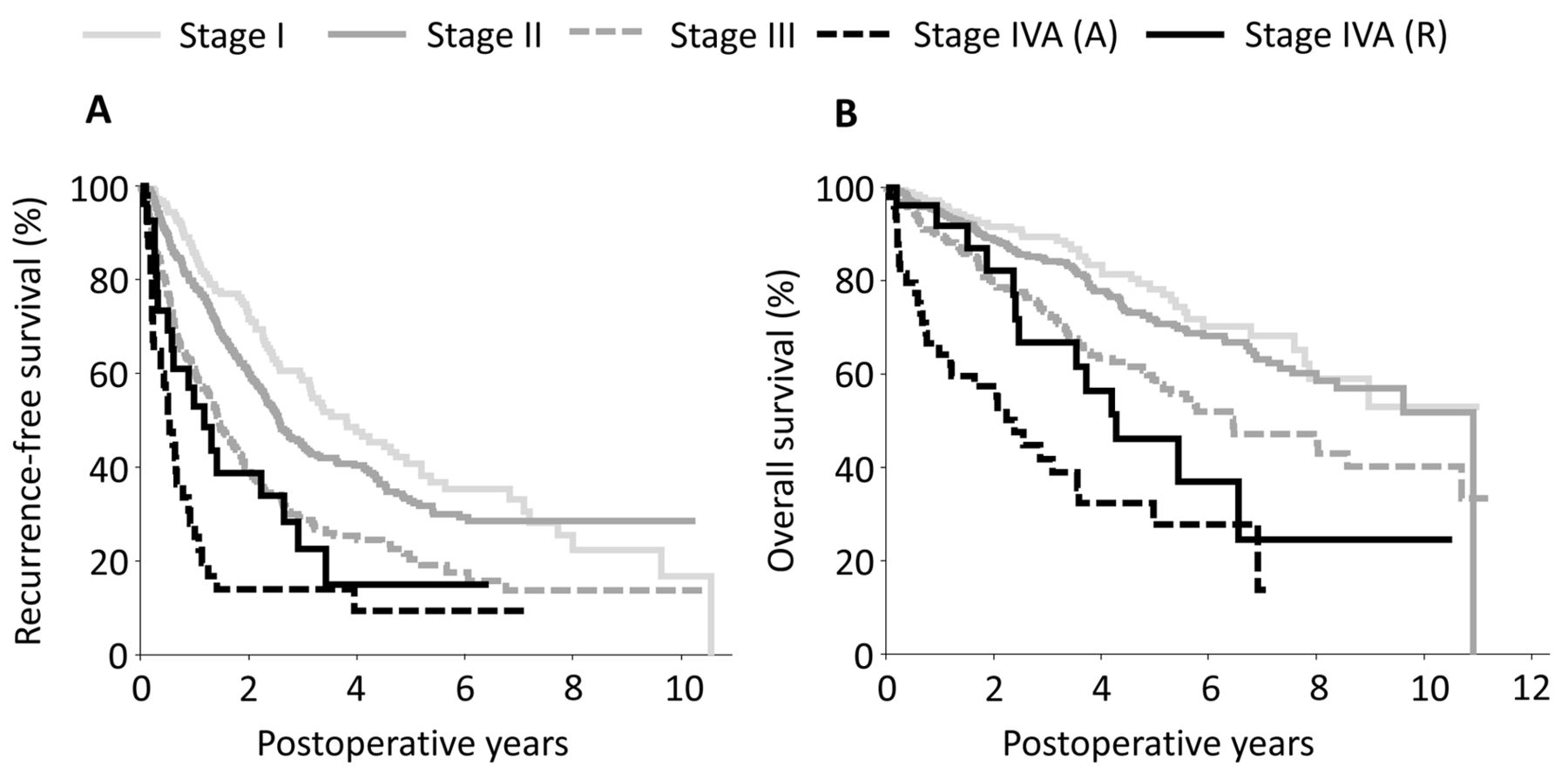
Recurrence-free (A) and overall (B) survival according to the staging system of the Liver Cancer Study Group of Japan (10).
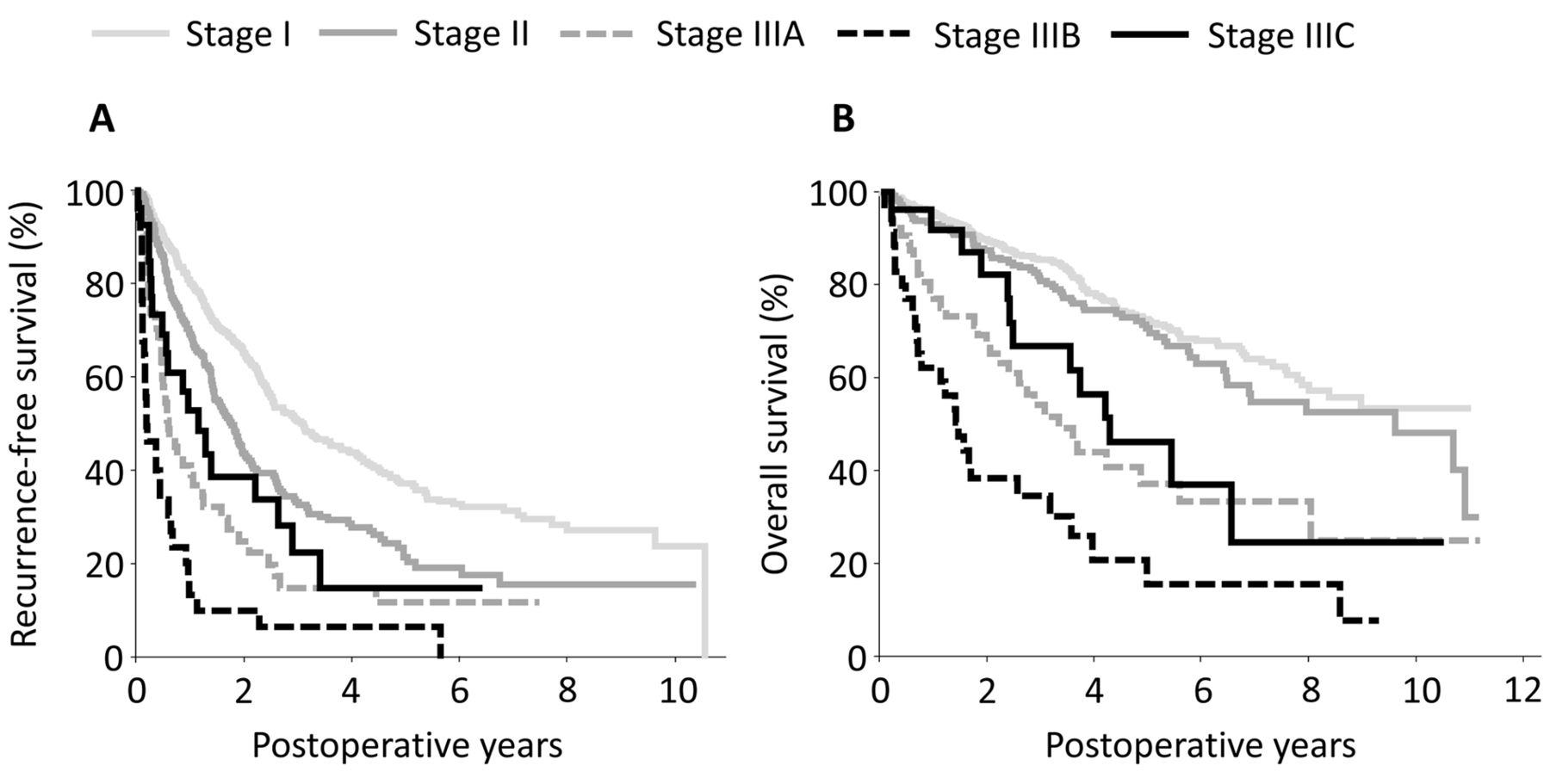
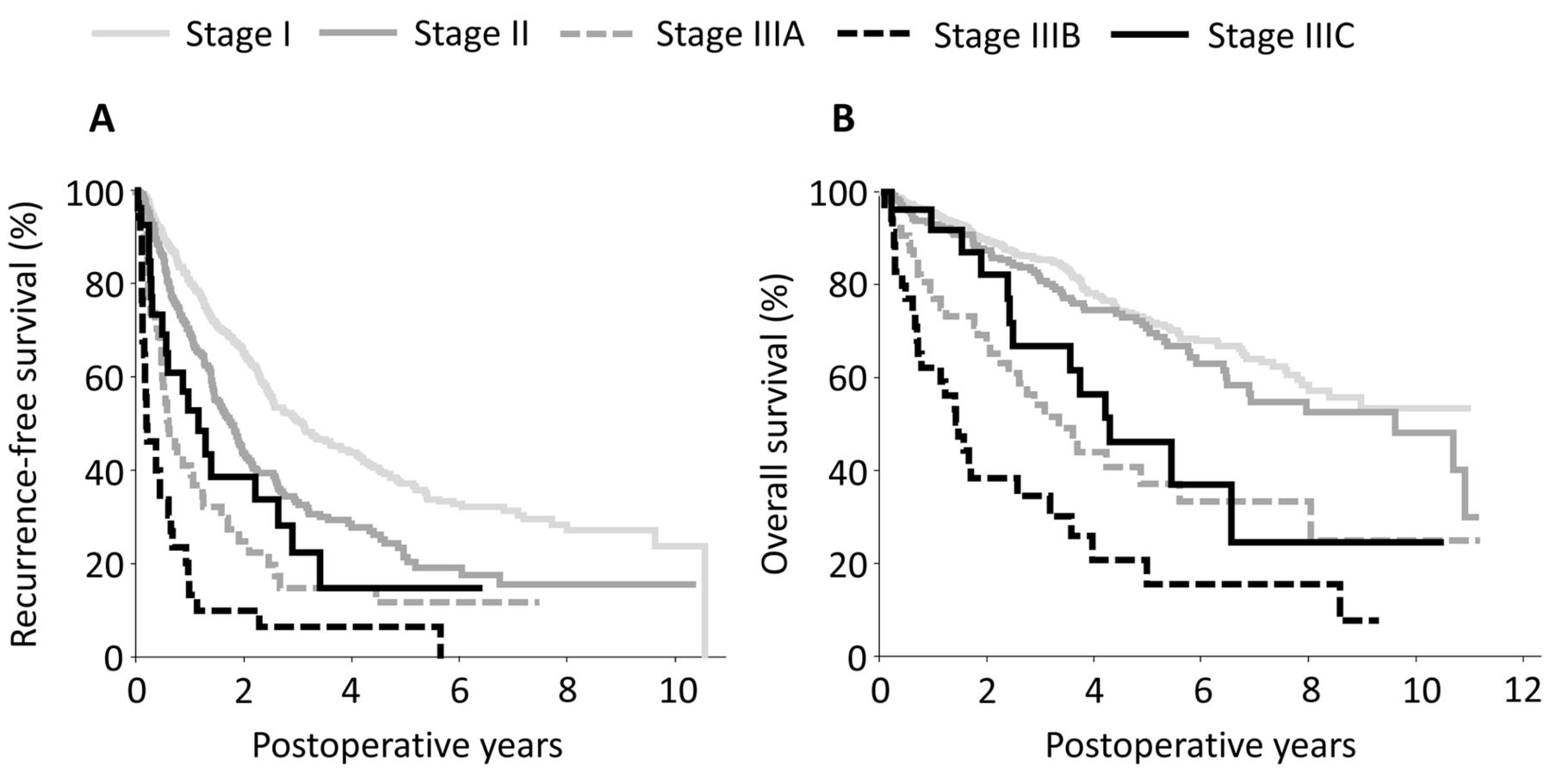
Recurrence-free (A) and overall (B) survival according to the staging system of the Union for International Cancer Control (11).
Recurrence-free survival and overall survival according to the UICC staging system. Figure 3 shows the recurrence-free and overall survival according to the UICC staging system. The median recurrence-free survival durations in stage I, II, III A, III B and III C were 1,141, 656, 231, 81 and 433 days, respectively. Patients with stage III C HCC experienced significantly better recurrence-free survival than those with stage III B (p<0.01). The recurrence-free survival of patients with stage III C was comparable to that of those with stage II or III A HCC. The median overall survival durations in stage II, III A, III B and III C were 3,503, 1,211, 531 and 1,563 days, respectively. Patients with stage III C HCC experienced significantly better patient survival than those with stage III B (p<0.01). The overall survival of patients with stage III C was comparable to that of those with stage III A.

Presumed stage without inclusion of rupture as a risk factor.
Presumed stages without the inclusion of rupture as a risk factor. In order to clarify HCC progression regardless of rupture, a presumed stage without taking rupture into consideration was applied to each patient. In LCSGJ staging, this resulted in 14, 12 and one patient being classified into stage II, III and IV A, respectively. In UICC staging, 14, 5, 7 and one patient were thus classified into stage I, II, III A and III B, respectively (Figure 4).
Risk factor analysis for tumor recurrence and patient death after curative resection of HCC. Nine risk factors, namely maximum tumor diameter >2 cm, maximum tumor diameter >5 cm, multiple tumors, any vascular invasion (which could be identified by imaging studies), major vascular invasion (vascular invasions to the first branches of the portal vein, the main portal vein, the right, the middle, the left hepatic veins, the inferior right hepatic vein, the short hepatic veins, or the inferior vena cava which could be identified by imaging studies), liver damage grade B/C (10, 17), α-fetoprotein >400 ng/ml, des-γ-carboxy prothrombin >300 mAU/ml and tumor rupture, were analyzed as risk factors for tumor recurrence and patient death for the 1031 patients (Table II). The cut-offs of α-fetoprotein and des-γ-carboxy prothrombin were determined by previous reports (18, 19). All risk factors were significant not only for tumor recurrence but also for patient death after R0 hepatectomy in univariate analyses. However, tumor rupture was neither a risk factor for tumor recurrence nor for overall survival in multivariate analyses.
Comparisons of recurrence sites among TNM stages. Table III shows recurrence sites by TNM stage. The most frequent recurrence site was the liver in all TMN stages. Peritoneal recurrence was occasionally encountered in the stages other than stage III C. All 19 patients with stage III C disease who experienced recurrence had intrahepatic recurrence, while only three patients had peritoneal recurrence. The time to intrahepatic recurrence in patients with stage III C patients was longer than that for patients with stage III A (323 vs. 186.5 days).
The current staging systems for hepatocellular carcinoma.
Risk factors for tumor recurrence and patient death after curative resection of hepatocellular carcinoma.
Discussion
The current study clearly demonstrated that patients who underwent hepatectomy for ruptured HCC experienced favorable outcomes with respect not only to recurrence-free survival but also to overall survival although they were classified with stage IV A disease by the current LCSGJ staging system and stage III C by the current UICC staging system. Tumor rupture seems to result in tumor cell seeding in the peritoneum and therefore an increased incidence of recurrence on the peritoneum (20-22). Contrary to our expectations, only three patients with ruptured HCC experienced peritoneal recurrence. Most patients experienced intrahepatic recurrence, as observed for patients with non-ruptured HCC. Rupture was not a significant risk factor for recurrence-free and overall survival in multivariate analyses, as reported by Cheng et al. (23).
Results in the current study with regard to complete resection for ruptured HCC were obtained from a relatively small number of patients (27 patients). However, encountering patients with ruptured HCC has become rare, even in high-volume centers for HCC, probably because of the advancement of screening for patients with high risk for developing HCC. Analyses among affiliated hospitals have benefits of studying patients with similar backgrounds in the region, with similar management styles, and with similar follow-up schedules. Despite the small number of patients with ruptured HCC in the current study, the results clearly show that such patients experienced favorable outcomes with regard not only to recurrence-free but also to overall survival.
Summary of first recurrence sites according to the Union for International Cancer Control (UICC) stages (11).
Staged hepatectomy may be a safer procedure than emergency hepatectomy for ruptured HCC (24-26). On the other hand, Hai et al. demonstrated a favorable outcome of one-stage hepatectomy for ruptured HCC (27). Most patients with ruptured HCC have unstable condition caused by considerable blood loss in the peritoneal cavity. Patients may subsequently be afflicted by shock liver. In addition, most patients with HCC have impaired liver function due to chronic liver diseases. In these situations, emergency hepatectomy without sufficient preoperative evaluation seems to be dangerous because it may result in postoperative liver failure. Emergency hepatectomy for ruptured HCC should be reserved only for healthy and stable patients. The advancement of intervention techniques enables radiologists to control bleeding from ruptured HCC in most cases (28, 29). After the patient's condition is stabilized and sufficient preoperative evaluations are made, staged hepatectomy should be planned for ruptured HCC.
It is a matter for debate whether a complete resection of ruptured HCC should be performed after the control of bleeding by TAE/TACE. Some investigators reported that staged hepatectomy for ruptured HCC seemed to yield a better prognosis than TAE alone (30, 31). TAE/TACE alone rarely leads to complete necrosis of HCC. Because peritoneal recurrence is a rare event, complete resection of ruptured HCC may lead to long-term survival (2, 32, 33). In addition, another benefit of resecting ruptured HCC is that it completely erases the possibility of re-bleeding. As shown in Table III, most patients with ruptured HCC had intrahepatic recurrence, the same recurrence pattern, as observed in patients with non-ruptured HCC. In order to eliminate possible intrahepatic metastases, an anatomical resection may be desirable even in patients with ruptured HCC.
Why is the incidence of peritoneal recurrence of ruptured HCC quite low? Digestive malignancies such as gastric cancer readily lead to peritoneal seeding of cancer cells once they invade the visceral peritoneum. HCC is known to be one of the most hypervascular tumors among digestive malignancies. HCC cells freely released into the peritoneal cavity probably cannot survive unless there are appropriate blood vessels nourishing these cells in the immediate vicinity. This may be one reason why peritoneal seeding of ruptured HCC is relatively rare.
With regard to rupture as a risk factor, the current staging systems (LCSGJ and UICC) might have to be modified, as suggested by Aoki et al. (12). Most patients with advanced cirrhosis succumb to bleeding within 30 days because they are only able to undergo conservative therapies because of their poor liver function (2, 28). In such patients, rupture has a detrimental impact on outcome, which is why rupture as a factor results in T4 staging. However, patients with ruptured HCC referred to surgery have a good liver function and can tolerate various types of treatment. In patients with preserved liver function, rupture does not have a detrimental impact on outcome.
In conclusion, complete resection of ruptured HCC yielded favorable outcomes with regard not only to recurrence-free but also overall survival, and might lead to long-term survival. Contrary to expectations, peritoneal recurrence was a rare event. Surgery (an anatomical resection is desirable) should be actively considered for patients with ruptured HCC as in patients with non-ruptured HCC.
Footnotes
Conflicts of Interest
There was no funding source for this work and none of the Authors had any conflict of interest to declare.
- Received October 16, 2015.
- Revision received November 13, 2015.
- Accepted November 17, 2015.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}