


Abstract
Aim: We retrospectively investigated surgery following chemo-radiation in patients with biliary tract cancer (BTC) treated at our Institution. Patients and Methods: Among 339 patients, 44 patients underwent chemo-radiation prior to surgery. Chemo-radiation entailed 2-3 months of standardized chemotherapy and 50-60 Gy radiation at the main tumor and regional and para-aortic lymph nodes. Results: Thirty-one BTC cases were classified as initially resectable (IR) and 13 as initially un-resectable (UR). Eighty percent of the BTCs were diagnosed as extrahepatic bile duct cancers. Gemcitabine (1,000 mg/m2) and radiation was used to treat 59% of patients. Thirty percent of patients underwent hemi-hepatectomy, and 50% underwent pancreatoduodenectomy. The R0 resection rate was 90% among IR and 54% among UR, and 3-year survival rates were 82% for IR and 17% for UR, respectively. Conclusion: This retrospective analysis suggests that surgery after chemoradiation may contribute to R0 resection rate and survival for initially resectable BTC.
Abbreviations: 5FU, 5-Fluorouracil; BTC, biliary tract cancer; CA19-9, carbohydrate antigen 19-9; CEA, carcinoembryonic antigen; CTCAE, common toxicity criteria adverse events; i.a., intraarterial infusion; PVE, portal vein embolization; S-1 TS1 tegafur, gimeracil, oteracil potassium; UFT, tegafur and uracil; UICC, International Union Against Cancer.
Neoadjuvant and adjuvant therapies for biliary tract cancer (BTC) are being explored due to the unsatisfactory outcomes after radial resection (1-9); R0 resection rates were approximately 70% (2, 3), and the 5-year survival rate after R0/R1 resection was less than 50% (1-4). In adjuvant therapy, there exist several problems, including lack of a standard protocol. Severe morbidity frequently occurs after extended surgery (e.g., hemi-hepatectomy and/or pancreatoduodenectomy with or without vascular resection and reconstruction), and a 30% dose reduction would be necessitated due to impairment of organs, especially liver (1, 10, 11). Thus, appropriate neoadjuvant therapy would be a desired alternative approach.
Chemotherapy and/or radiation therapy followed by surgery for BTC has not been well-investigated. Several studies (including case reports) concern initially un-resectable cases with ‘down-sizing’ or ‘adjuvant surgery’ (12-16); little information is available on initially resectable cases or neoadjuvant therapy (17-20). Additionally, the treatments followed by surgery in almost all cases were systemic chemotherapy. Chemo-radiation therapy for BTC has been mainly investigated in liver transplants (21, 22). Based on our Institutional experience with chemo-radiation followed by surgery for pancreatic cancer (23-25), we applied a similar protocol to BTC; briefly, two to three months of chemotherapy with radiation treatment of the main tumor and regional and para-aortic lymph nodes. This addresses local control of the invasive front with radiation and addresses control of micro-metastasis with chemotherapy.
The present study aimed to investigate the use of surgery following chemo-radiation therapy for treatment of BTC by retrospective review of patients' records, to evaluate whether a prospective study is warranted. We have now conducted over 300 BTC surgeries, including over 40 BTC surgeries following chemo-radiation, and herein summarize their results. Several approaches to surgery following chemo-radiation have been taken: chemo-radiation has been applied to the initially resectable cases (neoadjuvant therapy) as well as to the initially un-resectable cases (so-called ‘down-size,’ ‘conversion,’ or ‘adjuvant surgery’). We compared patient characteristics and different approaches, with special focus on survival after first treatment.
Patients and Methods
Patients and criteria for classification of biliary tract cancer. We retrospectively reviewed records of 339 patients who underwent BTC surgery through 2013 at our Institution. This study was approved by the Institutional review board (No. 1408271143).
We used the JSBS (Japanese Society of Biliary Surgery) general rules for classification of biliary cancer, Surgical and Pathological Studies on Cancer of the Biliary Tract (5th edition) (26), and TNM classification of malignant tumors of the International Union Against Cancer (UICC) version 7 (27). Histological evaluation used the criteria proposed by Drs. Oboshi and Shimosato (28)
Pre-treatment evaluation. Pre-treatment evaluation included the patient's medical history and physical examination, blood tests, imaging tests using contrast-enhanced computed tomography or magnetic resonance imaging, endoscopic retrograde cholangiography and/or percutaneous transhepatic cholangiography, electrocardiogram, spirogram, and chest X-rays. Pathological proof was obtained before the start of treatment as follows: biopsy for papilla Vater cancer, brushing cytology and/or bile juice cytology for bile duct cancer, and bile juice cytology for gall bladder cancer. Preoperative staging were performed using image-based diagnosis (29, 30).
Criteria for surgical treatment. A decision regarding operability was made based on liver oncological and functional status (2). The criteria used to recommend surgery were based on the cut margin and size of the remnant liver. Briefly, the cutting line of the biliary duct should be 5 mm away from the biliary duct stricture, and the estimated remnant liver volume (with normal liver function) should be more than 30% of the total liver volume, before or after PVE (31, 32).
The criteria used to exclude surgery were clear distant metastasis, cancer extension beyond the 2nd branch of the remnant biliary duct, major invasion of the major vessels of the remnant liver, and/or small estimated remnant liver volume.
Categories of chemo-radiation therapy followed by surgery and treatment protocol. Patients who underwent chemo-radiation therapy were categorized with either ‘initially resectable’ or ‘initially un-resectable’ BTC. Distinct treatment protocols were applied.
Patients who met criteria for surgical treatment in pre-treatment evaluation were defined as initially resectable BTC. In contrast, when the pre-treatment evaluation did not support the criteria for surgical treatment, cases were defined as initially un-resectable BTC, similarly to a previous report (12), and these patients underwent chemo-radiation therapy with a longer chemotherapy phase than the initially resectable BTC patients. The decision regarding operability used the same criteria for surgical treatment.
Chemo-radiation was performed with the standardized chemotherapy in use at the time (through 2005: 5-fluorouracil (5-FU) or UFT (tegafur and uracil), and in 2006 or later: Gemcitabine) in combination with 50-60 Gy of radiation. The procedures are categorized in Table I. Radiation therapy targeted the main tumor and regional and para-aortic lymph nodes (Figure 1). At least one month of drug withdrawal is necessary before surgery. If necessary, PVE was performed between the end of the chemo-radiation and surgery, during the one-month withdrawal time.
Follow-up evaluation. Blood tests (including carcinoembryonic antigen [CEA] and carbohydrate antigen 19-9 [CA19-9]) and/or imaging tests were planned every 3 months (at least) after start of treatment; additional blood tests and imaging were performed to confirm recurrence if clinically suspected. Overall survival was calculated from the start of treatment and the time of surgery.
Definition of adverse events during chemo-radiation therapy and surgical complications. We retrospectively collected information concerning adverse events during chemo-radiation and surgical complications from the patients' records. We evaluated adverse events according to the common toxicity criteria adverse events (CTCAE) version 4.0, and evaluated surgical complications according to Clavien-Dindo Classification (33).
Statistical analysis. Overall and recurrence-free survival rates were calculated by the Kaplan-Meier method and differences between groups were tested by the log-rank test. Differences between groups were tested using the Student's t-test and Chi-squared test. Differences were considered statistically significant at p<0.05. All statistical analyses were performed using the StatView J-5.0 software (SAS, Cary, NC, USA).
Results
Patients' characteristics. Among 339 BTC patients, 44 patients (13%) underwent surgery following chemotherapy and/or radiation therapy. Thirty-one patients (70%) were treated for initially resectable BTC, whereas 13 (30%) were treated for initially un-resectable BTC (Figure 2). Patients' characteristics are summarized in Table I. Seventy-five percent of patients were treated after 2001, with 61% treated between 2005 and 2011. Bile duct cancer was diagnosed in 80% and hilar cholangiocarcinoma was diagnosed in 34% of the patients.
Treatment course. We summarize treatments in Table I and adverse events/complications in Table II. Most chemo-radiation treatment protocols called for 1,000 mg/m2 of gemcitabine (on day 1, 8, 15; every 4 weeks) with 50 Gy of radiation. The number of gemcitabine treatments administered was 7 to 9 (2 to 3 cycles), and the average length between first treatment and surgery was 117 days (3.9 months). Other chemotherapy regimens were as follows: 3 patients were treated with 5-FU plus radiation, 2 with UFT, 2 with UFT plus radiation, 1 with intraarterial infusion (i.a.) of 5-FU plus radiation, 1 with i.a. of 5-FU plus cisplatin, 1 with systemic cisplatin plus methotrexate, and 1 with systemic 5-FU. During this period, the main severe events observed were neutropenia and elevation of transaminase. Two patients were noted as severe hyperbilirubinemia, but these patients were treated with radiation therapy during sustained obstructive jaundice; during treatment, serum bilirubin was gradually decreased without any other complications in these patients. Nine patients (20%) underwent plastic stent exchange during chemo-radiation.
Thirty percent of surgical procedures performed were hemi-hepatectomies, and 50% were pancreatoduodenectomies. In four cases only extrahepatic bile duct resection was performed; otherwise, extrahepatic bile duct resection was performed in 91% of patients in addition to other procedures, even if extended cholecystectomy (66% extended cholecystectomy with bile duct resection and 34% without bile duct resection. The average operative time was 549 min (about 9 h) and estimated blood loss was 1,993 g; 26 patients (59%) underwent transfusion. No mortality was observed for the 30 days following surgery. The major severe complication observed after surgery was biliary leakage, which especially affected patients with initially un-resectable BTC; overall, 75% experienced biliary leakage, 66% severe leakage, and two patients succumbed to sepsis following biliary leakage at 63 and 68 days after surgery. Other severe complications, hemorrhage and liver abscess, were seen in the initially un-resectable cases.

Typical dose distribution of radiation for right hepatectomy. (A) Dose distribution around the bile duct. (B) Dose distribution around the hepatic artery in the hepatico-duodenal ligament.
Patients' characteristics and pathological status of resected specimens.
Adverse events and complications.
After surgery, 59% of the patients underwent adjuvant therapies: 13 patients underwent hepatic infusion therapy (intra-portal or intra-arterial chemotherapy), 9 systemic gemcitabine, 4 UFT, 2 systemic 5-FU plus cisplatin, 1 systemic 5-FU, 1 S-1 (TS-1; tegafur, gimeracil, oteracil potassium), and 1 radiation therapy.
Pathological evaluation. As seen by pathological diagnosis, 80% of patients achieved R0 resection. Among patients with initially resectable BTC, 90% achieved R0 resection (Figure 2). Pathological lymph node metastasis was noted in 20% of the patients (Table I). In patients treated as initially resectable, absence of pathological lymph node metastasis (pN0) was noted in 84% and negative surgical cut end in 94%. In contrast, among patients treated as initially un-resectable, R0 resection was achieved in 54% of cases, negative lymph node metastasis was noted in 69%, and negative cut end in 69%.

Surgical and pathological results after chemo-radiation followed by surgery depended on whether the BTC was defined as initially resectable or un-resectable. The upper panel shows the category and number of patients. The lower panel shows the rate of R0 resection, negative lymph node metastasis, and negative surgical cut end among the two categories, initially resectable and initially un-resectable.
Histological type, cancer-stroma relationship, and growth pattern are summarized in Table I. Micro-invasion was visualized in 11-27% of patients. Vascular invasion of major vessels was noted in 5% of the patients. Moderate and marked histological change was noted in 25% of patients according to the criteria proposed by Drs. Oboshi and Shimosato (28).
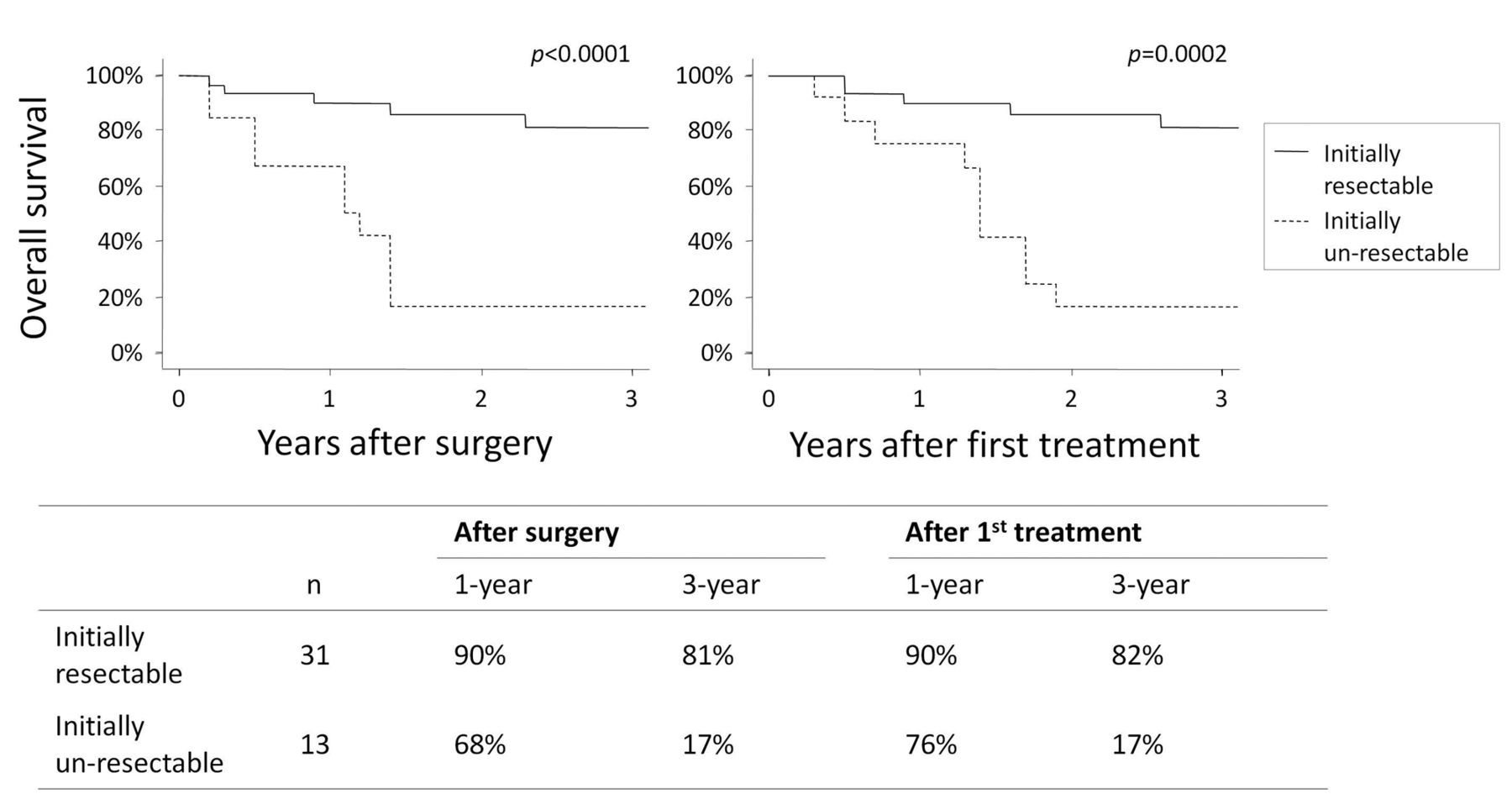
Survival. We summarize survival in Figure 3. The average observation period was 3.1 years. In patients treated as initially resectable, 3-year survival was 82%; however, in patients treated as initially un-resectable, 3-year survival was 17% (p<0.05). In 35 patients with R0 resection, 5 patients (14%) suffered from local recurrence. Nine patients (20%) survived more than 5 years in this observation period; 7 patients with initially resectable BTC (23%) and 2 with initially un-resectable BTC (15%) (note: the number of patients who survived more than 5 years would be larger with a longer observation period).
Discussion
Herein, we retrospectively reviewed the records of the 13% of BTC patients who were treated with surgery following chemo-radiation therapy at our Institution. Among the patients with initially resectable BTC, 90% achieved R0 resection and the 3-year survival rate was 82%.
The overall 5-year survival of BTC after surgery (mainly surgery-only treatment) was 30-50%, with 70% R0 resection (3). The 3-year survival rate, limited to patients with R0 resection, was 60% (2). Although statistical analysis and consideration of possible selection bias would be necessary to confirm our results, our 3-year survival rate of 82% seems not to be inferior to the surgery-only approach reported previously. The R0 resection rate, that is 90% in our study also compares favorably to already published rates (appproximately 70%) (2, 3). Our data indicate that it would be worthwhile to continue this therapeutic approach (chemo-radiation therapy in the neoadjuvant setting) and necessary to evaluate the outcome prospectively with intention-to-treat analysis and resection rate (registration: UMIN000015450), as the retrospective study might exclude patients with progressive disease during chemo-radiation. Previous reports regarding neoadjuvant therapy were supportive to our speculation (17-19). Although it is difficult to compare previous studies, one report presented the feasibility of neoadjuvant chemo-radiation with a protocol similar to that used in this study (18), and one report presented the value of achieving the negative surgical cut end (19). Another study showed that neoadjuvant chemotherapy, but not chemo-radiation therapy, did not improve patients' survival (17), suggesting that chemo-radiation, rather than chemotherapy alone, followed by surgery would be necessary for effective neoadjuvant therapy.

Survival curves after chemo-radiation followed by surgery, calculated from the time of surgery and the time of first treatment, shown for initially resectable and un-resectable cases. The left-upper panel shows a graph of overall survival from the surgery for the two categories, initially resectable and un-resectable. The right upper panel shows a graph of overall survival from the first treatment. The lower panel lists the actual percentage of 1- or 3-year survival after the surgery or the first treatment.
On the other hand, treatment of initially un-resectable cases (locally advanced BTC) for down-size should be carefully considered. Our study found 3-year survival of 17%, with 54% R0 resection. The surgical cut end was pathologically positive in 31% of cases, and severe complications had occurred. According to previous reports, chemotherapy with GEM provided 18% 3-year survival and R2 resection provided 19% (2). We consider the survival data among these treatments (chemo-radiation and surgery for initially un-resectable BTC, chemotherapy, and R2 resection) to be similar, although we consider the possibility that patients' backgrounds could be quite different. In the other aspect, only ‘chemoradiation and surgical treatment’ might provide 5-year survival of initially un-resectable BTC (2). In the present study, two of these patients survived more than 5 years. The previous report showed at least one case of 5-year survival among 8 patients who were treated with surgery following chemotherapy (note: a longer observation period would result in a larger number of 5-year survivors) (12). Although chemo-radiation therapy followed by surgery for initially un-resectable BTC provided similar 3-year survival rates compared to chemotherapy-only or with R2 resection, it may provide the best chance of long-term survival. With more severe risks yet a chance of long-term survival, careful consideration must be given to the decision whether or not to provide this treatment in cases of initially un-resectable BTC.
Pathological evidence supported our findings regarding benefit for survival and R0 resection in initially resectable BTC. Pathological evaluation after chemo-radiation showed negative lymph node metastasis in 84% (positive lymph node metastasis 16%), with an average number of 17 resected lymph nodes. Positive lymph node metastasis was noted in 39-41% in the national BTC survey (3) and in 45-51% of patients who were treated by surgery-only in previous reports (34, 35). Observations regarding other factors were similar to those from a previous report (34); scirrhous cancer-stroma relationship was 34% (in our data 34%), infiltrating growth pattern was 14% (herein 25%), micro-invasion to venous system was 29% (herein 11%) and to nervous system was 35% (herein 27%). However, micro-invasion to the lymphatic system was seen in 65% of the cases treated with surgery-only in the previous report, compared with 23% invasion seen in this study. These data indicate the possibility that chemo-radiation therapy may regulate lymphatic spread in BTC. Molecular biological evidence would be necessary for confirmation. For example, we previously showed that cells at the invasive front and metastatic sites in BTC expressed ‘chemotherapy’ resistance-related genes and showed epithelial-mesenchymal transition (EMT) and an excess of inflammatory cytokines (36). To further investigate our findings, we would need to evaluate the effect of chemo-‘radiation’ at the invasion front and/or regional lymph node metastatic site after treatment and compare with the effect of chemotherapy-only treatment.
By the way, similarities and differences of chemoradiation therapy followed by surgery between pancreatic cancer (23, 24) and BTC were as follows; the similarity was adverse effects during the chemo-radiation. In contrast, the difference was difficulty of surgery around the hepaticoduodenal ligament. In BTC, extensive bile duct resection and lymph nodes resection around the hepaticoduodenal ligament should be necessary, compared to pancreatic cancer. Cholangitis during the preoperative treatments and/or chemo-radiation effects would induce thickness of the ligament and cause difficulty of the surgery and necessity of a more careful technique.
In conclusion, our retrospective study indicated 90% R0 resection with 84% negative lymph-node metastasis after chemoradiation of initially resectable BTC before surgery. Chemo-radiation therapy followed by surgery in initially resectable BTC may contribute to patients' survival via improvement of R0 resection rates and regulation of lymph node metastasis by loco-regional control. Prospective studies of this treatment are necessary to further elucidate these observations. In contrast, in cases with initially un-resectable BTC, we found a limited R0 resection rate of 54% with chemoradiation therapy prior to surgery. We recommend the careful weighing of risks and potential benefits in cases of initially un-resectable BTC.
Acknowledgements
The Authors acknowledge our grant sponsor, Grant-in-Aid for Scientific Research (C).
- Received October 6, 2015.
- Revision received November 25, 2015.
- Accepted November 27, 2015.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}