


Abstract
Background/Aim: Hepatocellular cancer is a rising dilemma. Patients with unresectable disease may benefit from locoregional therapy. The comparative effectiveness of radioembolization and Doxorubicin-Drug-Eluting-Beads (DEBDOX) has not been established to date. We compared the performance of radioembolization and DEBDOX in the treatment of hepatocellular carcinoma. Patients and Methods: An analysis of our prospectively managed locoregional therapy (LRT) database was performed. Three hundred and fifty-eight patients were treated with LRT for unresectable HCC, out of which 291 were treated with DEBDOX and 67 with Ytrrium-90 (90Y). Comparative toxicity, tumor response, progression-free survival (PFS) and overall survival (OS) were assessed. Propensity score matching was used to reduce treatment-selection bias, producing 48 pairs. Comparative analysis was repeated after propensity matching. Results: Median age was 67 and 65 years for the DEBDOX and 90Y groups respectively (p=0.2). Overall survival favored the DEBDOX group (DEBDOX: 15-months, 90Y: 6-months, p<0.0001). PFS also favored the DEBDOX group (DEBDOX: 15-months, 90Y: 6-months, p<0.0001). All-grade adverse events were similar in both groups, although slightly favoring the DEBDOX group (DEBDOX 10%, 90Y 15%, p=0.1). After propensity score matching, again longer OS was seen with the DEBDOX group (DEBDOX 13 months, 90Y 4 months; p=0.0077). There were also similar all-grade adverse events that slightly favored DEBDOX (DEBDOX 14%, 90Y 20%, p=0.3). Disease control rate was found to be statistically significant, favoring the DEBDOX group (DEBDOX 72%, 90Y 48%; p=0.02). Conclusion: Our observation suggests that DEBDOX outperforms 90Y with superior efficacy and survival with a trend towards lower all-grade toxicity.
- Efficacy
- toxicity
- DEBTACE
- RECIST
- Ytrrium-90
- DEBDOX
- radioembolization
- chemoembolization
- hepatocellular carcinoma
Hepatocellular carcinoma (HCC) is one of the most common cancers worldwide and a major cause of global mortality. Surgical resection, ablation or transplantation provide the only chance of cure; however, there is a substantial population with advanced disease not amenable to surgery. Locoregional therapies (LRT), such as Yttrium-90 (90Y) radioembolization and chemoembolization, can provide local tumor control in those patients (1-3). In addition, they can potentially help down-stage patients to resection or help bridge patients to transplantation (4-6). Transarterial chemoembolization (TACE) may be performed in a conventional fashion (cTACE) utilizing lipiodol mixed with one or more chemotherapeutic agents (mitomycin C, doxorubicin, cisplatin). Alternatively, it can be performed using Drug Eluting Beads loaded with Doxorubicin (DEBDOX). DEBDOX is a newer device created to optimize the pharmacokinetics of doxorubicin and better standardize the treatment dose delivery (7). A randomized prospective study comparing cTACE and DEBDOX showed similar efficacy between both devices, but improved safety profile with DEBDOX (8). On the other hand, a recent meta-analysis comparing cTACE with DEBDOX for the treatment of HCC, indicated that DEBTACE outperforms cTACE with superior survival and treatment response (9).
While there has been no large randomized prospective study comparing the efficacy of cTACE to radioembolization (to the best of our knowledge), several comparative cohort studies exist (4, 10-13). The largest cohort, a large retrospective study comparing cTACE with 90Y showed similar survival but longer time-to-progression and less toxicity with 90Y (14). A small pilot randomized trial comparing cTACE to radioembolization showed that both devices had similar toxicities (15).
Despite the improved safety profile of DEBDOX compared to cTACE, there has been no large comparative study between DEBDOX and 90Y. A pilot 24-patient randomized trial comparing DEBDOX to radioembolization showed median overall survivals (OS) of 788 days and 592 days for DEBDOX and 90Y respectively, but this difference did not reach statistical significance (16). Given the increased interest to establish comparative effectiveness of comparable treatments in real-life clinical scenarios, we engaged in a comparative analysis of DEBDOX and 90Y for the treatment of unresectable HCC using our prospectively managed LRT registry.
Patients and Methods
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki. A retrospective search of our Institutional Review Board-approved, prospective, multi-institutional, open, non-controlled, repeat-treatment registry was performed spanning from 2007 to 2013. Three hundred and fifty-eight consecutive patients with unresectable HCC were treated with LRT. A multidisciplinary team evaluated patients to determine the mode of therapy. Patients in our registry were 18 years or older with unresectable HCC with or without portal vein thrombosis (PVT). Those with another primary malignancy and advanced liver disease (defined as bilirubin levels >3 mg/dL, aspartate aminotransferase/alanine aminotransferase >5-times the upper limit of normal or >250 U/L) were excluded. Standard pre-therapy evaluation of patients with HCC included at least a 3-phase CT of the abdomen and pelvis. Patients were grouped according to their index (first) intra-arterial treatment modality.
Chemoembolization technique. Our technique for DEBDOX (Drug-Eluting Bead (DEB); Biocompatibles UK) has been previously published. In brief, visceral angiogram was performed to evaluate the arterial anatomy, tumor vascularity, and presence of arteriovenous shunting. Patients were typically planned for two to three treatment cycles based on the extent of liver tumor involvement. Patients with bi-lobar disease were planned for a minimum of four treatments (100-150 mg each, depending on the hepatic reserve and extent of tumor burden), with two treatments per lobe spaced in three to four week intervals depending on patient toxicity. Placement of the delivery microcatheter was based on the extent and location of liver disease. For a finite number of lesions, the microcatheter was placed according to tumor location and size for the first bead vial infusion. The microcatheter was then pulled back for lobar infusion for the second bead vial infusion. For diffuse disease, a lobar infusion was performed. Various bead sizes were used at the discretion of the treating physician ranging from 100-300 (most common) to 500-700 micron beads.
Radioembolization technique. A visceral angiogram was performed to evaluate arterial anatomy and determine optimal placement of the microcatheter for embolization. 99mTC-labeled macro-aggregated albumin was delivered through the hepatic artery to assess hepatopulmonary shunting and to detect hazardous extrahepatic deposition. Shunt fractions were calculated by using planar scintigraphy. The radioembolization device used was TheraSphere (MDS Nordion Inc., Kanata, ON, Canada). Our method for calculating the required TheraSphere activity and the mean dose delivered to the liver and lungs has been published (17). If eligible, the TheraSphere dose was delivered in strict accordance with the manufacturer's recommended guidelines.
Study schedule and outcome measures. Patients were assessed for any treatment-related adverse experiences for 1 month after each treatment. Adverse events were recorded per standards and terminology set by the Cancer Therapy Evaluation Program's Common Terminology Criteria for Adverse Events (CTCAE) version 3.0. Pre-therapy evaluation included a 3-phase CT of the abdomen and pelvis. Follow-up protocol consisted of a 3-phase CT scan of the liver within 3 months post-treatment. Tumor response rates were measured according to European Association for the Study of the Liver (EASL) or modified Response Evaluation Criteria in Solid Tumors (mRECIST) criteria (18, 19). Follow-up was repeated every 3 months for the first year and every 6 months for the second year. Overall response rate (ORR) refers to the combination of complete and partial responders per mRECIST. Disease control rate (DCR) refers to the combination of all responders and those with stable disease. Overall survival (OS) was defined as the time between the treatment start date and death from any cause. Progression-free-survival (PFS) was defined as the time between the start of treatment and image-based disease progression or death.
Statistical analysis. An as-treated analysis was performed with patients censored at switch from the index treatment modality to the other. They were also censored to definitive curative therapy (surgical resection, transplant, ablation) and to last clinic follow-up if death was not confirmed.
The Student's t-test and Mann-Whitney U-test were used for continuous data comparisons. The Fisher's exact and Chi-square tests were used for categorical data comparison (two-tailed). Survival and progression-free survival probabilities were generated with Kaplan-Meier statistics. Difference in the probability curves was assessed using the log-rank test. Multivariable Cox regression was used to evaluate the association between independent variables and survival. p-Values less than 0.05 was considered statistically significant. All statistics were calculated using the JMP software (JMP, SAS Institute Inc, Cary, NC, USA).
Propensity score analysis. Given that both populations were heterogeneous and not randomized, selection bias was inevitable. Therefore, a propensity match was performed. This is the most aggressive statistical method to control for patient background variables in a cohort study, ensuring that prognostic factors in the different groups are similarly distributed. This method has been shown in multiple studies to observationally mimic randomized control trials (20-23). The propensity scores generated were used to create matched pairs of patients in the DEBDOX and 90Y groups. Propensity scores were generated using treatment as the dependent variable and factors potentially influencing treatment as independent variables. Logistic regression was used to generate a propensity score ranging from 0 to 1. One-to-one matching between patients undergoing M1-DEBIRI and DEBIRI was performed. Patient scores were matched to at least 3 digits. If we could not find a match, we proceeded to two- and one-digit matched pairs. We were able to match 48 DEBDOX patients to 48 90Y patients. The scores ranged from 0.104 to 0.992. After score-based matching, the groups differed by no more than 0.09. The independent variables (prognostic factors) used in our model were age, gender, history of hepatitis, PVT, total size of target, Child Pugh status, extrahepatic disease, Karnofsky Performance Status, prior liver surgery, history of ablation, prior sorafenib and current sorafenib. Similar to the pooled patient analysis described above, the same comparative analysis was subsequently performed on the matched patients. In addition, a sub-group comparative analysis involving patients with PVT was also performed, given the general debate on which modality is preferred in this patient subset.
Clinical characteristics of the pooled cohort.
Results
Pooled Cohort (Non-Matched)
Patients' characteristics. Using the selection criteria above, a total of 358 consecutive patients were included. Two hundred ninty-one patients were treated with DEBDOX and 67 patients with 90Y. Baseline characteristics are summarized in Table I. Median age was similar between both groups, 67 years for DEBDOX and 65 years for 90Y (p=0.2). There was a better baseline in performance status in the 90Y group (Karnofsky score 90% vs. 72%; 0.0025). Child Pugh status favored the DEBDOX group (<0.0001). Okuda staging was different between both groups with the DEBDOX group having a higher percentage of Okuda 1 classification and the 90Y group having a higher percentage of Okuda II classification. In addition, there was a higher proportion of patients with PVT in the 90Y group (0.0001). The groups were similar in the remaining characteristics including age, gender, hepatitis type, alpha fetoprotein (AFP), tumor extent, total size of target, extrahepatic disease, prior sorafenib, concurrent sorafenib and prior liver surgery.
Clinical characteristics of the matched cohort.
Toxicity in the pooled cohort.
Treatment factors and adverse events. There were 596 DEBDOX treatments in 291 patients. The mean dose planned was 100 mg (range=50-300 mg) and the mean dose delivered was 75 mg (range=0-250). There were also 117 90Y treatments in 67 patients. Overall adverse events were similar in both groups (DEBDOX-10%; 90Y-15%; p=0.1). There was no difference between groups in high-grade adverse effects (DEBDOX 4.5% and 90Y 4%; p>0.999). The most common side-effects were pain, nausea/vomiting, and liver dysfunction in the DEBDOX group and pain, nausea, liver dysfunction and dehydration in the 90Y group. Adverse events are summarized in Table III.
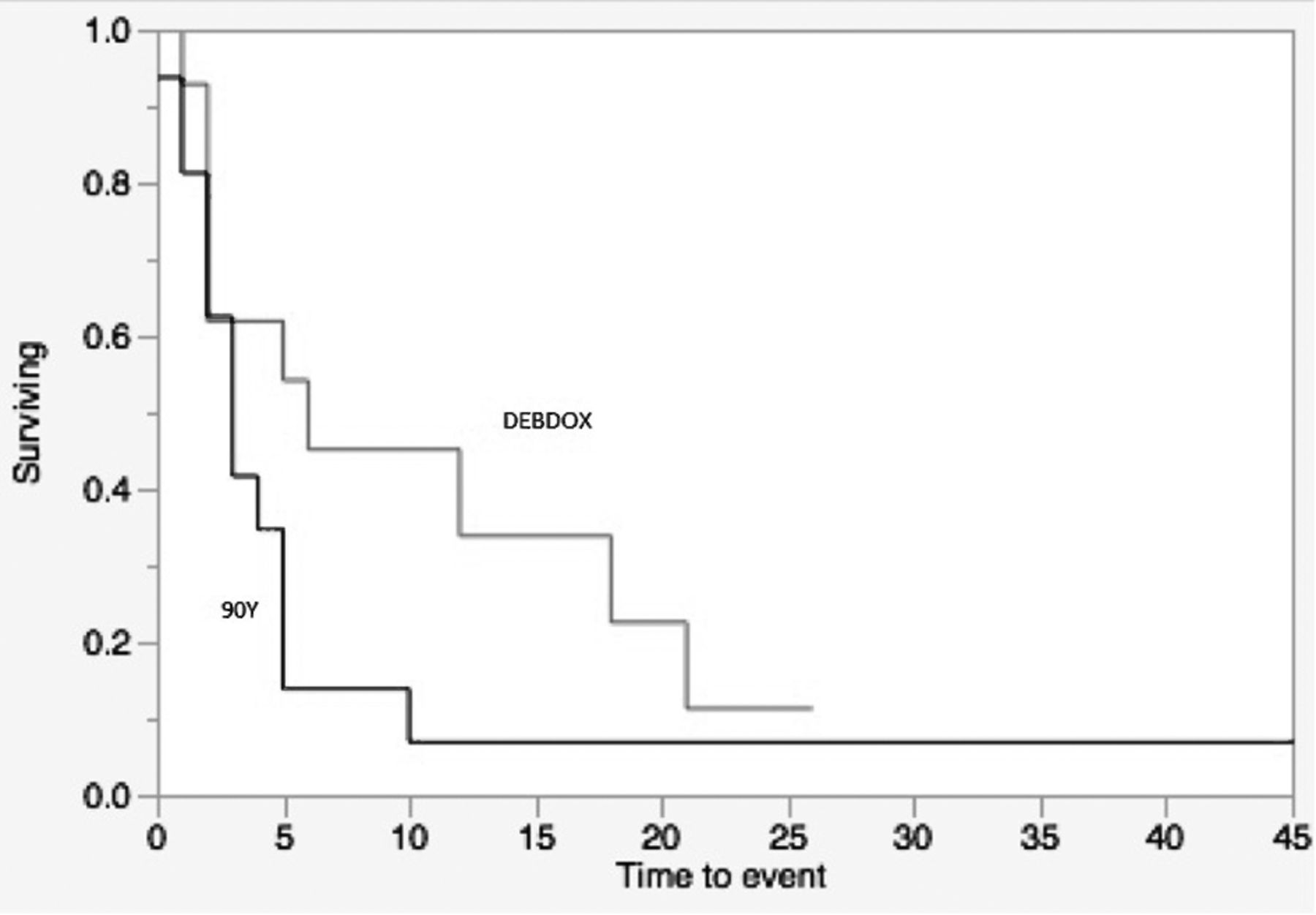
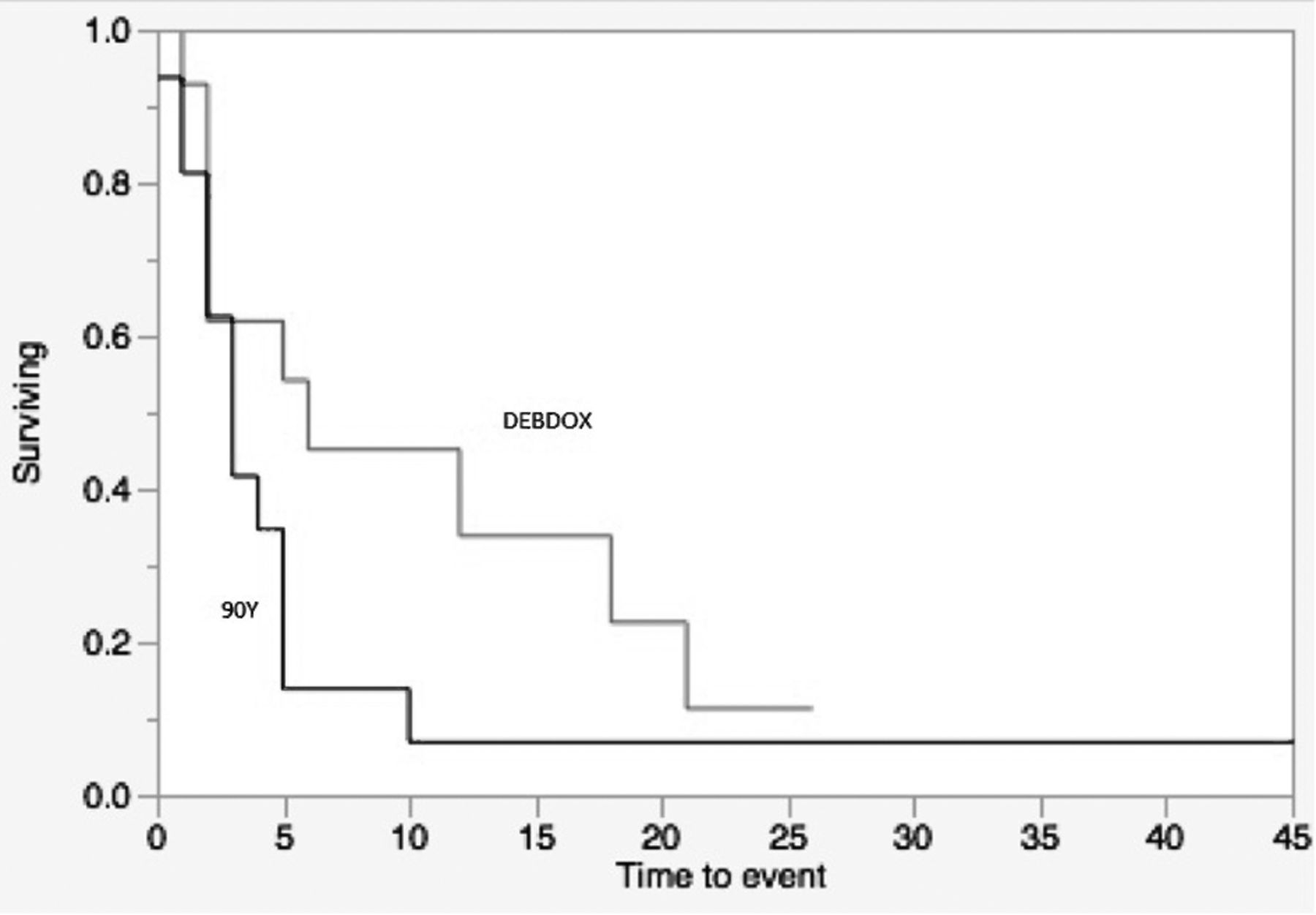
Treatment efficacy and survival. Treatment response is summarized in Table V. There was 41% overall response for DEBDOX and 34% overall response for 90Y- this trend did not approach statistical significance. On the other hand, DCR was statistically significant favoring the DEBDOX group (p=0.0041). Median survival was found to be significantly different between both groups. The DEBDOX group had a median survival of 15 months compared to 6 months for the 90Y group (log-rank, p<0.0001) (Figure 1a). PFS was also different between the groups with 15 months for DEBDOX and 5 months for 90Y (log-rank, p<0.0001) (Figure 1b). Multivariate analysis showed that treatment type, PVT, prior sorafenib and total size of target were independent prognostic factors (Table VII). The remaining patient variables were not identified as prognostic factors in our patient cohort. Thirteen patients (4%) in the DEBDOX group proceeded to RFA (n=9) and transplant (n=4). One patient (1%) in the 90Y group had liver resection. There were 10 patients (3%) in the DEBDOX group that crossed over to receive 90Y, and 16 (24%) patients in the 90Y group that crossed over to receive DEBDOX. The reason for crossover was most commonly target lesion progression on index treatment.
Toxicity in the matched cohort.
Matched Cohort
Patients' characteristics. Patients' characteristics are summarized in Table II There were 48 DEBDOX-treated patients matched with 48 90Y treated patients. Median age was similar; 61.5 and 66.5 years for DEBDOX and 90Y respectively (p=0.08). Aside from better performance status in the 90Y group compared to the DEBDOX group (p=0.02), both groups were similar in the remaining patient characteristics including age, gender, presence of hepatitis, Karnofsky score, alpha-fetoprotein level, Child Pugh status, Okuda classification, tumor extent, sum of target lesions, PVT, extrahepatic disease, prior sorafenib, concurrent sorafenib and prior liver surgery/ablation.
Treatment factors and adverse events. Adverse events are summarized in Table IV. There were 96 treatments in the DEBDOX group and 80 treatments in the 90Y group. The time from diagnosis-to-treatment was 6-months and 5-months for the DEBDOX and 90Y groups respectively (p=0.56). The rate of adverse events per treatment was higher in the 90Y group compared to the DEBDOX group (20 % vs. 14 %); although this trend did not reach statistical significance (p=0.3). The rate of high-grade adverse events was similar between both groups with 7% for DEBDOX and 6% for 90Y (p>0.999). The most common adverse events were pain and vomiting for the DEBDOX group and pain and nausea for the 90Y group.

90Y versus DEBDOX overall survival for the pooled cohort (a). 90Y versus DEBDOX progression-free survival for the pooled cohort (b).

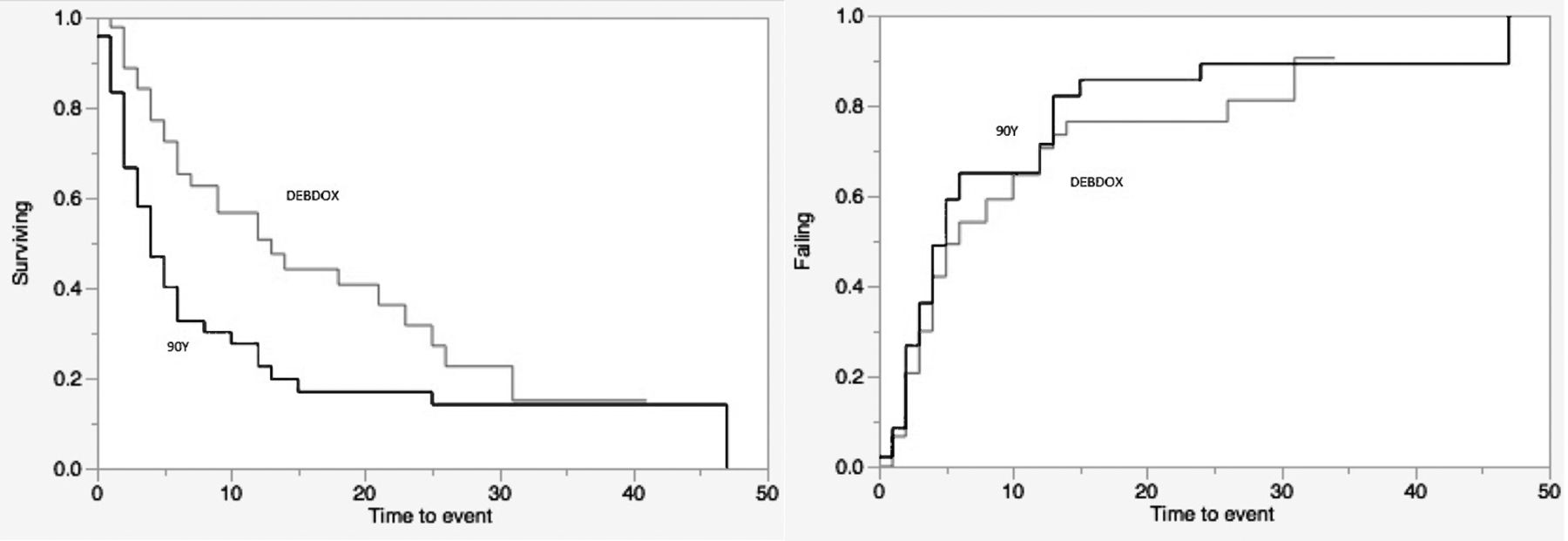
90Y versus DEBDOX overall survival for the matched cohort (a). 90Y versus DEBDOX progression-free survival for the matched cohort (b).
Treatment efficacy and survival. Treatment response is summarized in Table VI. There was a higher overall response for DEBDOX (47%) compared to 90Y (35%); however, this was not statistically significant (p=0.29). On the other hand, DCR was found to be statistically significant favoring the DEBDOX group (DEBDOX 72%, 90Y 48%; p=0.02). As also seen in the pooled cohort, median survival was significantly different between both groups (Figure 2a). The DEBDOX group had a median survival of 13 months compared to 4 months for the 90Y group (log-rank, p=0.0077). PFS was similar between the groups with 6 months for DEBDOX and 5 months for 90Y (log-rank, p=0.42), although most of the progression seen in the 90Y group was death rather than disease progression, as seen with the DEBDOX group (Figure 2b). There were 3 patients (6%) in the DEBDOX group that proceeded to ablation. One patient (2%) in the 90Y group had liver resection. No patients underwent transplantation. There were 10 patients in the 90Y group (20%) that crossed over to receive DEBDOX, with no patients from the DEBDOX group (0%) who crossed over to receive 90Y. As with the pooled cohort, the reason for crossover was most commonly target lesion progression on index treatment. Multivariate analysis revealed treatment type (DEBDOX, 90Y) to be an independent prognostic factor (Table VIII). Okuda classification was also an independent prognostic factor with the remaining patient variables not identified as prognostic factors.
90Y versus DEBDOX overall survival for the portal vein thrombosis sub-group.
PVT sub-group analysis (from matched cohort). The PVT sub-group showed a trend towards longer overall survival favoring DEBDOX with a 6-month overall survival for DEBDOX compared to 3 months for 90Y (log-rank; p=0.13) (Figure 3).
Discussion
Chemoembolization and radioembolization are LRT modalities that show efficacy in the treatment of HCC. There exists strong evidence showing the benefit of chemoembolization in the treatment of HCC (24, 25). DEBDOX is a new chemoembolization device that allows more standardized delivery of chemotherapy while reducing toxicity. TheraSphere, the radioembolization device we utilized, has been approved by the Food and Drug Administration (FDA) for the treatment of HCC.
Our pooled data showed similar rates of all-grade and high-grade adverse events in both groups. On the other hand, there was better disease control and longer OS/PFS with DEBDOX compared with 90Y. Given that the results seen in our pooled data was marred by the heterogeneity of both groups, it was difficult to draw conclusions about the comparative effectiveness of each treatment. After propensity score matching, baseline characteristics in both groups were homogenous aside from higher performance status in the 90Y group. Again, as with the pooled cohort, there were similar rates of all-grade and high-grade toxicity in both groups (with a trend favoring DEBDOX). Better disease control in the DEBDOX group compared to the 90Y group was again seen, congruent with the pooled cohort. Furthermore, overall survival significantly favored the DEBDOX group with a 13 month overall survival compared to 4 months in the 90Y group. This was quite surprising given that the 90Y group had better baseline performance status. PFS was similar in both groups (DEBDOX, 6 months; 90Y, 5 months), but this is a misleading end-point since some of the progression in the 90Y group was due to death rather than pure disease progression. The superiority of DEBDOX over 90Y in this comparative study is further validated by its identification as an independent prognostic factor by multivariate analysis in both pooled and matched cohorts.
Response in the pooled cohort.
Response in matched data.
Despite better efficacy seen with DEBDOX, the ability to down-stage patients to surgery/ablation was similarly low in both groups and not statistically significant. This is in keeping with the observation that both treatment modalities had similar image-based response rates (although slightly favoring the DEBDOX group). Although, they provide similar response rates, DEBDOX provides superior disease control (due to higher rates of stable disease) and slightly lower toxicity that may explain the observed survival advantage.
DEBDOX and radioembolization are generally utilized as equivalent therapies for HCC in some institutions, but this common practice is primarily based on cohort comparative studies (without propensity matching), which showed cTACE with similar efficacy compared with 90Y (4, 10, 11, 14). Our study did not reproduce those findings. Of note, those studies did not evaluate DEBDOX and were not propensity matched cohorts. DEBDOX is more embolic than 90Y, and there is evidence that suggests that the embolic aspect of an LRT device -in and of itself- is important and cannot be trivialized in the setting of HCC (26). In fact, some practitioners exclusively use bland embolization for the treatment of HCC (27). Overall, we do concede that our findings are observations and large randomized control studies are needed to validate these findings before current clinical practice is altered.
Multivariate Cox regression for pooled cohort.
Because a sizable number of patients in both groups had PVT (DEBDOX 29%, 90Y 33%) and the locoregional treatment-of-choice for PVT is somewhat controversial, we performed a sub-group analysis. Our findings in the PVT sub-group showed a trend towards longer overall survival favoring DEBDOX. The insignificant p-value was most likely a result of the smaller sample size. As many studies have shown, PVT in the setting of HCC is not a contraindication to chemoembolization as previously believed (28-31). However, dedicated comparative studies are needed in this area to establish the preferred treatment.
There are several limitations to the current study. First is the retrospective study design. Second, the matched data set was small, therefore larger matched sets may provide more compelling conclusions in the future. Third, the strength of a propensity match is subject to the detail of the registry. There may be characteristics that influence survival that are unknown and therefore not recorded which may significantly impact our findings. Fourth, there may be specific subgroups that may benefit more from one treatment device over the other (i.e. Okuda class, Child Pugh, Barcelona Clinic Liver Center class); however, sub-stratification was not performed in this study. Our interest was to determine the comparative effectiveness of each device in a “real-life” treatment population since both modalities are commonly regarded as equivalent therapies.
Our observation from our LRT registry suggests that DEBDOX has similar toxicity compared to 90Y, but outperforms 90Y with better efficacy and survival. Given the small sample of the propensity-matched pairs, larger prospective studies are warranted to validate or refute our findings.
Multivariate Cox regression for the matched cohort.
- Received November 10, 2015.
- Revision received November 8, 2015.
- Accepted December 10, 2015.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}