


Abstract
Aim: The current study investigated outcomes and prognostic factors of pulmonary oligometastases at two Institutions. Patients and Methods: SBRT (stereotactic body radiotherapy) as performed for pulmonary oligometastases from January 2004 to April 2014, and patients with a biologically effective dose (BED10) ≥75 Gy were registered in the study. Control of the primary tumor was not a criterion: we included both oligo-recurrence and sync-oligometastases. Results: A total of 34 patients were enrolled in the study. The median overall survival was 20 months (range=1-119 months) and the 2-year overall survival rate was 65.7% [95% confidence interval (CI)=48.3-83.1%]. The two-year local control rate was 79.1% (95% CI=62.4-95.8%). Stratified by oligo status, the 2-year overall survival rate of the oligo-recurrence group was 68.5% (95% CI=50.3-86.7%), while that of the group with sync-oligometastases was 50.0% (95% CI=1.0-99.0%). These rates were significantly different (p=0.037). No grade 5 early- or late-adverse events were recognized in the current study. Conclusion: SBRT for pulmonary oligometastases achieved good results and there was no serious adverse event. The oligo-recurrence group, in particular, achieved fairly good results.
For a long time, patients with recurrence or metastasis of cancer have been considered to be in a terminal stage. Patients with distant recurrence or metastases receive systemic therapies strictly aimed at prolonging survival or relieving symptoms as palliation.
Hellman and Weichselbaum proposed the concept of ‘oligometastases’ in 1995 (1). In this concept, the primary tumor was active, with a few distant metastases, but ‘oligometastases’ implied that patients could live longer with local treatment (surgery, radiotherapy, radiofrequency ablation) of the distant recurrences/metastatic sites. At about the same time, Niibe performed radiotherapy for an abdominal para-aortic node in a case of isolated recurrence of cervical cancer at the National Institute of Radiological Sciences hospital in Japan, and achieved long-term survival, ultimately reporting in 2003 that c-ERBB2/HER2 (human epidermal growth factor receptor 2) is a prognostic factor for radiotherapy for such patients, and that such treatment can achieve a 5-year survival rate of 38% (2). Thereafter, multi-institutional retrospective studies on radiotherapy of isolated para-aortic nodes in uterine cervical cancer were undertaken, with similar results (3, 4). Moreover, investigations of patients with controlled primary lesions and brain metastases treated by stereotactic radiosurgery were performed and also led to good results (5). In 2006, Niibe et al. proposed a new concept that refined the concept of oligometastases to ‘oligo-recurrence’ (3-10), a state in which the primary tumor is controlled and only around 1-5 distant recurrences or metastases appear, for which local treatment of the distant recurrences/metastases can result in longer survival with better quality of life.
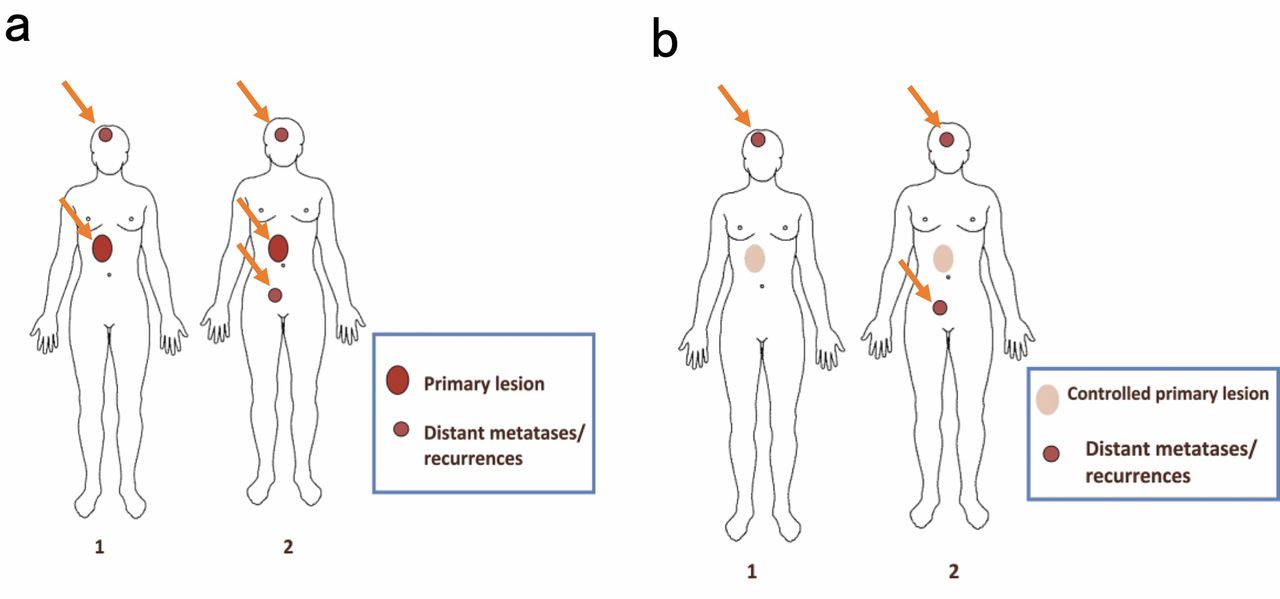
Niibe and Chang proposed the concept of sync-oligometastases (7). This is similar to the notion of oligometastases first suggested by Hellman and Weichselbaum with 1-5 distant recurrences/metastases and an active primary tumor; they argued that such patients benefit from local treatment to both the distant lesions and the primary tumor. Thus, the state for performing local treatment both for 1-5 distant recurrent/metastatic lesions and the primary tumor has been defined as ‘sync-oligometastases’. Figure 1 depicts the states of oligo-recurrence and sync-oligometastases. The primary tumor is controlled in the case of oligo-recurrence with only a few distant recurrences/metastases. In sync-oligometastases, both the primary tumor and distant recurrences/metastases are active.
The current study investigated SBRT (stereotactic body radiotherapy) for pulmonary oligometastases and treatment outcomes. At the same time, we examined the prognostic difference between oligo-recurrence and sync-oligometastases and examined other prognostic factors previously reported.
Patients and Methods
SBRT for pulmonary oligometastases was performed at the St. Luke's International Hospital or the University of Tokyo Hospital, from January 2004 to April 2014, and patients registered were those treated with BED10 ≥75 Gy (the current study adopted α/β=10). The study was approved by the Ethics Committees of both institutions.
Control of the primary tumor was not a criterion: we included both oligo-recurrence and sync-oligometastases cases in the study.
A radiotherapy dose of 12-12.5 Gy, by four fractions, to a total SBRT dose of 48-50 Gy was given to 20 out of 34 patients. This was the main treatment method in the study. The other 14 patients were treated by SBRT using 5 to 8 Gy/fraction and a total of 7 to 10 fractions because the target tumor was situated in the medial side.
Survival curves and local control curves were constructed by the Kaplan–Meier method; a curve was drawn for every potential prognostic factor, and significant differences were determined by the log-rank test. The level of significance was set at the 0.05 alpha level. All statistical analysis was performed using SPSS v.22.0 (IBM Corp., Armonk, NY, USA).
Results
Patients. Thirty-four patients on whom SBRT of BED10 ≥75 Gy was performed from January 2004 to April 2014 were enrolled in the current study. Patient's characteristics are listed in Table I. The patients included 22 men and 12 women, with a median age of 69.5 years (range=25-88 years). Most patients (32/34) had a Karnofsky Performance Status of 70 or more. Regarding the oligostatus, 30 patients were included in the oligo-recurrence group, and four patients in the sync-oligometastases group. In the oligo-recurrence group, the disease-free-interval (DFI), which was the time to recurrence from the start of primary treatment until the date of onset of distant recurrence/metastasis, was a median of 29 months (range=0-116 months). Of course, in the sync-oligometastases group, the DFI was 0 months.
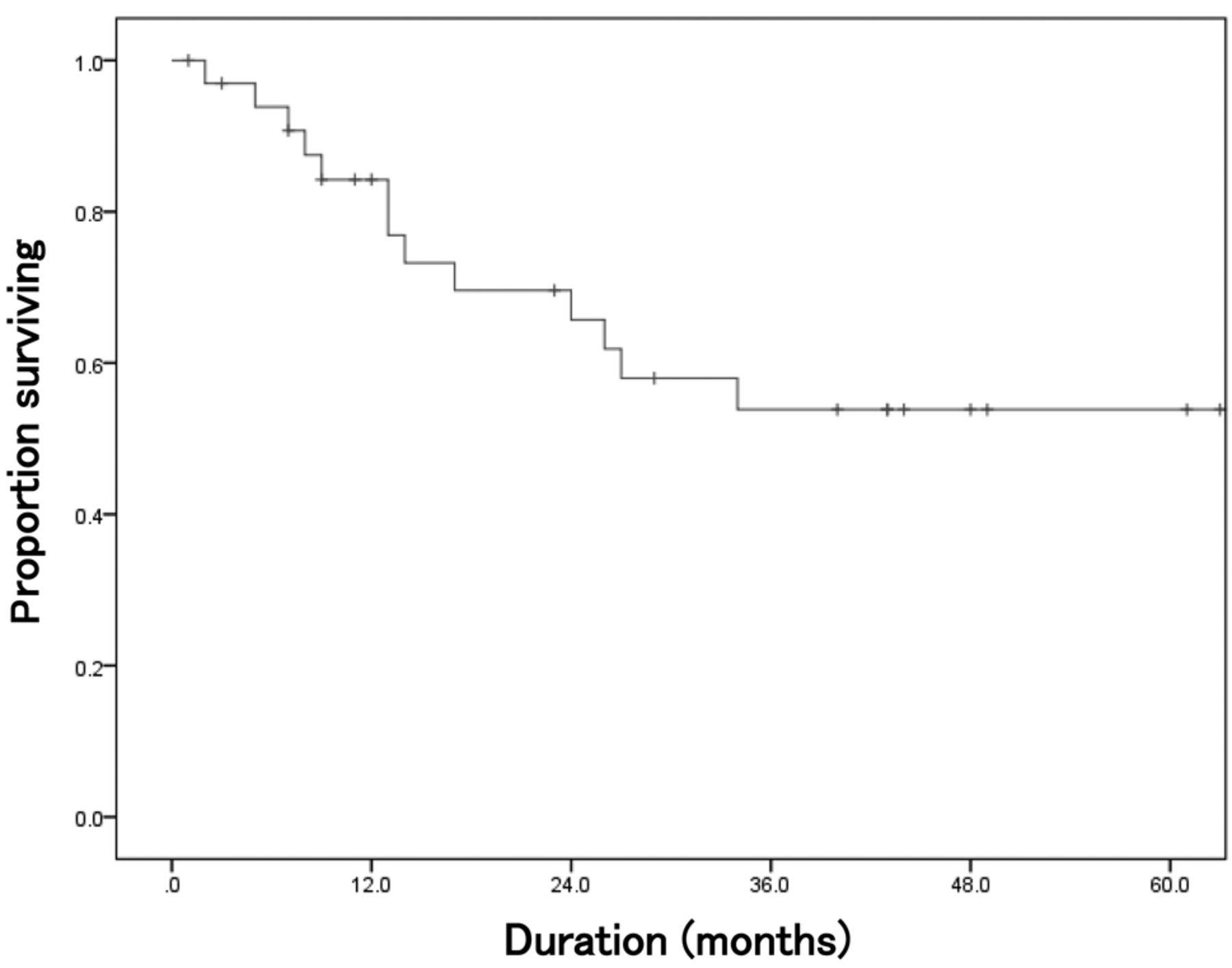
Survival and local control. The median overall survival of the whole patient cohort was 20 months (range=1-119 months) and the 2-year overall survival rate was 65.7% [95% confidence interval (CI)=48.3-83.1%]. These results were fairly good (Figure 2). The 2-year local control rate was also good at 79.1% (95% CI=62.4-95.8%) (Figure 3).
Patient's characteristics.
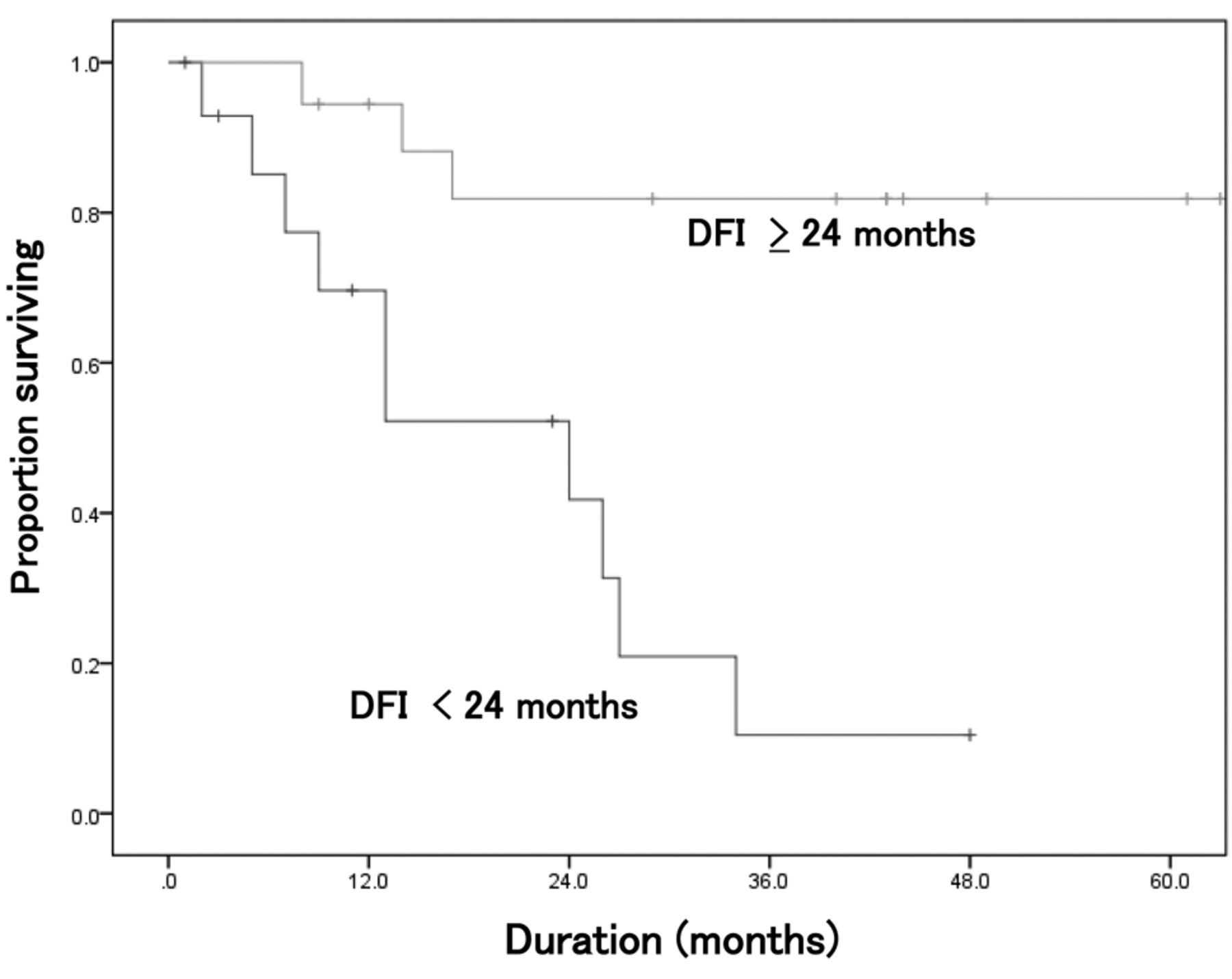
When stratified by oligostatus, the 2-year overall survival rate of the oligo-recurrence group was 68.5% (95% CI=50.3-86.7%), while the 2-year overall survival of the sync-oligometastases group was 50.0% (95% CI=1.0-99.0%). These rates were statistically different (p=0.037) (Figure 4). Stratified by histopathology, in order to compare the typically reported poor results of colon and rectal cancer with those of other primary cancer types, the 2-year overall survival rate for patients with colon and rectal cancer was 66.7% (95% CI=13.4-100%) while the 2-year overall survival rate of patients with other types was 66.2% (95% CI=48.0-84.4%). There was no statistically significant difference in outcome by primary site (p=0.878) (Figure 5). Regarding the local control rate, the 2-year local control rate in patients with cancer of the colon and rectum was 100% while that of patients with other types was 77.6% (95% CI=60.0%-95.2%; p=0.507) (Figure 6). Stratified by DFI, the 2-year overall survival of patients with a DFI ≥24 months was 81.9% (95% CI=63.3%-100%), while that of those with a DFI <24 months was 41.8% (95% CI=12.8-70.8%). These results achieved statistical significance (p<0.001) (Figure 7).
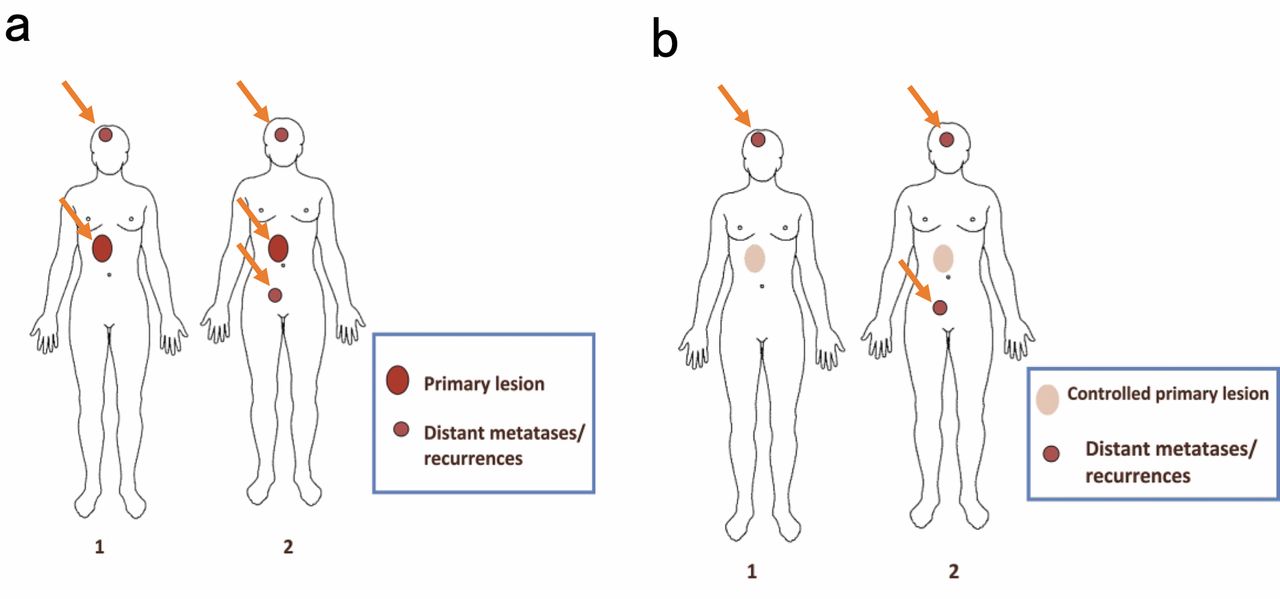
Schema of sync-oligometastasis and oligo-recurrence. a: In sync-oligometastasis, there are several distant recurrent or metastatic lesions and an active primary lesion. Both distant and recurrent or metastatic lesions should be treated and any active primary lesion by local treatment, if possible. b: Schema of oligo-recurrence. There are several distant recurrent or metastatic lesions and a controlled primary lesion. Only distant recurrent or metastatic lesions should be treated locally. Partially modified from Niibe et al. (6).
Adverse events. Regarding adverse events, one grade 4 event occurred in the acute phase. The case was a 59-year-old man with esophageal cancer, whose esophagus had been rebuilt with a gastric tube. Perforation occurred in the gastric tube. However, this event was thought to be due to the patient's general debility rather than being a side-effect of SBRT (using 48 Gy/4 fractions and no hot spot in the gastric tube area), since the patient was a heavy smoker and an alcoholic, and his overall status was weakened by these habits.
No late adverse events of grade 3 or more occurred according to the criteria of Radiation Therapy Oncology Group-The European Organization for Research and Treatment of Cancer Late Radiation Morbidity Scheme (11).
Discussion
It has been 20 years since the concept of oligometastases was proposed in 1995, but it is only in the recent past that the concept has begun to attract attention. The International Registry of Lung Metastases (IRLM) reported that the 5-year survival rate of completely resectable pulmonary metastasis cases was 36% when patients were operated on (12). However, as imaging and biochemical tests had not progressed very far at that time, it was difficult to predict the likelihood of complete resection before surgery. Furthermore, there were often numerous metastases even when physicians could find only one metastasis. Recently, rapid progress in such technologies as computed tomography, magnetic resonance imaging, and positron emission tomography-computed tomography and their integration make it easier to detect a state of oligometastases, including patients with isolated pulmonary metastasis. Tumor markers are also often measured regularly and are thought to contribute to the finding of several pulmonary metastases. One more reason oligometastases and oligo-recurrence have attracted attention recently is that less-invasive local treatment modalities such as sophisticated thoracoscopic surgery, SBRT and radiofrequency ablation are now available. Therefore, the Japanese guidelines recommend resection whenever possible for pulmonary metastasis in the oligo-recurrence state, such as in the primary site of colorectal cancer (13).

Overall survival of patients. The median survival time was 20 months (range=1-119 months). The 2-year overall survival rate was 65.7% (95% confidence interval=48.3%-83.1%).

Local control rate for the whole patient group. The 2-year local control rate was 79.1% (95% confidence interval=62.4-95.8%).

Overall survival stratified by oligo-status. The 2-year overall survival rate for the oligo-recurrence group was 68.5% (95% confidence interval=50.3-86.7%), whereas that for the sync-oligometastases group was 50.0% (95% confidence interval=1.0-99.0%). This was statistically significant (p=0.037).
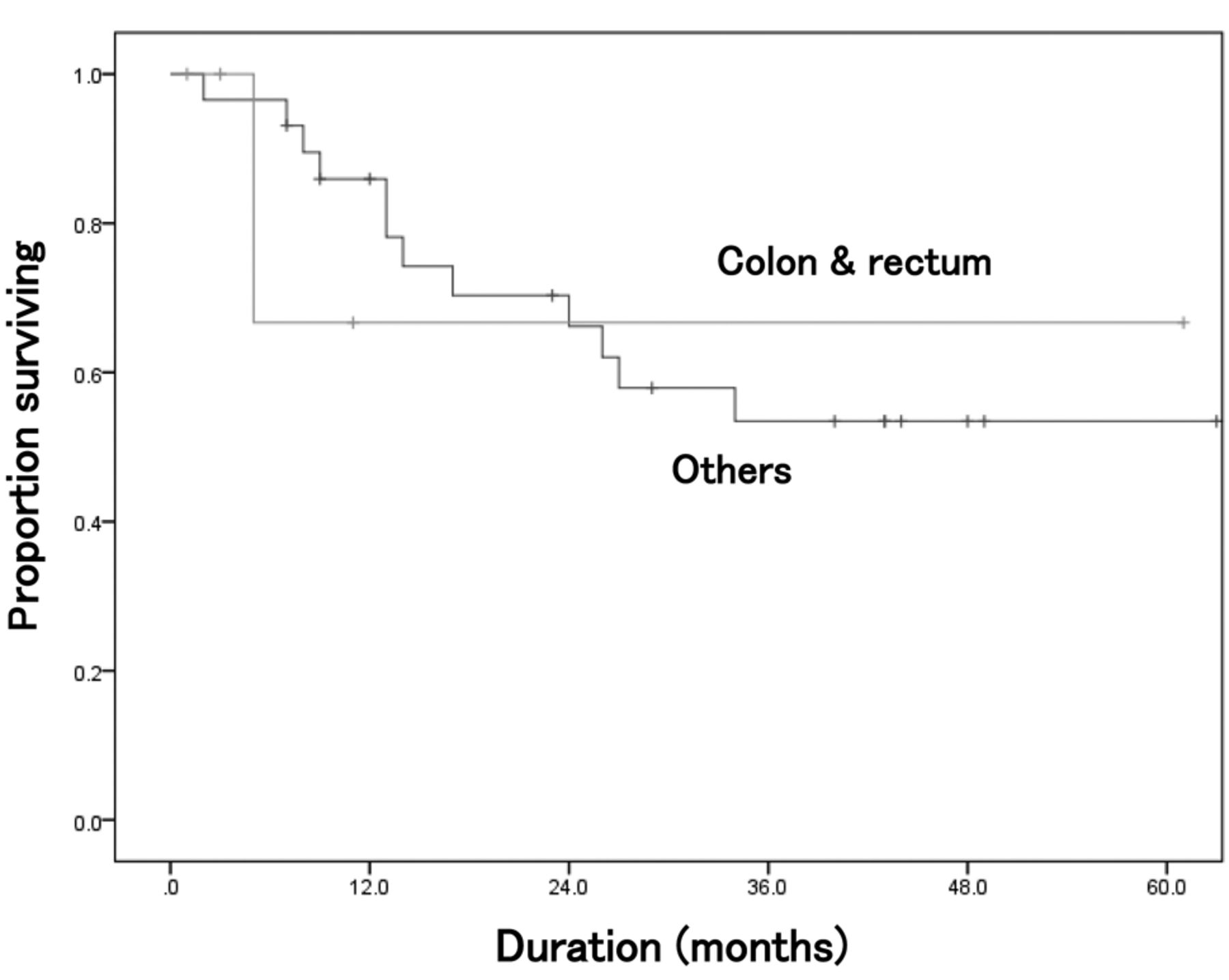
Overall survival stratified by histopathology. Comparing patients with colon and rectal cancer to those with other cancer types, no statistically significant differences in overall survival were found (p=0.878).

Local control stratified by histopathology. Comparing patients with colon and rectal cancer to those with other cancer types, no statistically significant differences in local control were found (p=0.507).
The current study achieved a 2-year overall survival rate of 65.7% (95%CI=48.3-83.1%) for the whole patient group. This is promising, considering that all our patients had recurrent or metastatic disease. The 2-year local control rate for the whole group was 79.1% (95% CI=62.4-95.8%). This was also a good result. Even if there were too few cases of pulmonary oligometastases in this study to draw firm conclusions, it is suggested that SBRT should be performed, rather than no treatment or systemic therapy alone, in these situations. Systemic therapy alone, for recurrent or metastatic cancer, does not generally achieve a cure.

Overall survival stratified by DFI. The 2-year overall survival rate of DFI ≥24 months was 81.9% (95% confidence interval=63.3%-100%), whereas that of DFI<24 months was 41.8% (95% confidence interval=12.8-70.8%). This was statistically significant (p<0.001)
This is the key difference between SBRT and systemic therapy. SBRT and other local treatments can achieve a cure for patients with oligometastases, especially those with oligo-recurrence. When another recurrence occurs after SBRT, patients with oligo-recurrence can repeat SBRT, even if the metastatic tumor occurs in again in the lung. Onishi et al. recently gave an excellent case report about sequential oligo-recurrence (14).
However, it cannot be said that patients with oligometastases always have long-term survival with good quality of life and achieve a cure. From the results of stratification by status, the oligo-recurrence group achieved a significantly higher 2-year overall survival rate (68.5% vs. 50.0%; p=0.037). As shown herein, for patients with oligometastatic disease, controlling the primary tumor is very important. Primary lesions often invade neighboring tissues and are often associated with regional lymph node metastases. This is why control of primary lesions is more difficult than that of round- or oval-shaped recurrent or metastatic lesions. In addition, recurrent or metastatic lesions rarely lead to regional lymph node metastasis.
In terms of histopathology, recurrent or metastatic lesions originating from the colon and rectum were reported to have worse responses than those from other origins when these lesions were treated by SBRT (15). In the current study, recurrent or metastatic tumors originating from the colon and rectum did not show a statistically worse response than those of other origins. However, it is difficult to generalize from these findings as there were only 34 patients in the study, and there were only the cases of colon and rectum primary cancer.
A relationship between outcomes of oligometastases treated by SBRT and the DFI has been reported: a DFI of 39.1 months or more was reported to predict better prognosis than that of less than 39.1 months in the study of SBRT for pulmonary oligo-recurrence (16). In another study, a DFI of 36 months or more was associated with better prognosis than that of one of less than 36 months (17). The threshold of the current study DFI was set at 24 months. A DFI of 24 months or more led to a 2-year overall survival rate of 81.9% versus 41.8% for a DFI of less than 24 months. These results were comparable to those of previous reports. A long DFI was found to be associated with a good prognosis. In addition, it was reported that certain interleukin molecules were involved when new distant recurrences or metastases arose from a disease-free state (7).
Conclusion
SBRT for pulmonary oligometastases achieved good results and there were no serious adverse events among 34 patients. However, a prospective study is required to validate these results. For such a study, we recommend that registered patients should be limited to those with oligo-recurrence due to their better prognosis compared to those with sync-oligometastases. Other findings in the current study confirmed that a long DFI (≥24 months) was a favorable prognostic factor for patients with pulmonary oligometastases.
Acknowledgements
This study was supported partly by grant-in-aid from JSPS KAKENHI Grant Number 21791209 and 25461926.
Footnotes
Conflicts of Interest
The Authors declare that they have no competing interests.
- Received May 5, 2015.
- Revision received June 13, 2015.
- Accepted June 15, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Pulmonary Oligometastases Treated by Stereotactic Body Radiation Therapy: A Nationwide Survey of 1,378 Patients
- Clinical Impact of Re-irradiation with Carbon-ion Radiotherapy for Lymph Node Recurrence of Gynecological Cancers
- Salvage Radiotherapy for Solitary Metachronous Bone Metastasis in Patients with Breast Cancer