


Abstract
Aim: To investigate the efficacy and safety of carboplatin, paclitaxel, and bevacizumab (CPB) combination chemotherapy in patients with non-squamous non-small cell lung cancer (NSCLC) with pre-existing interstitial lung disease (ILD). Patients and Methods: Twenty-five patients with non-squamous NSCLC with ILD who underwent CPB therapy between March 2007 and July 2013 were analyzed for treatment profiles. Results: The median age was 67 (range=53-79) years and 96% were men. The triplet chemotherapy was repeated for a median of four cycles. The objective response rate was 72% (18/25), the median progression-free survival time was 7.2 months, and the median overall survival time was 8.5 months. The most frequent adverse event of grade 3 or more was neutropenia (72%, 18/25). Chemotherapy-induced acute exacerbation of ILD occurred in 12% of patients. Conclusion: CPB therapy may be an effective and feasible regimen even for patients with ILD, although clinicians should be concerned regarding neutropenia and acute exacerbation of ILD.
Interstitial lung disease (ILD) is a heterogeneous group of non-neoplastic disorders resulting from lung parenchymal inflammation or fibrosis and is a risk factor for development of lung cancer (1, 2). Chemotherapy for lung cancer occasionally exacerbates pre-existing ILD and this can be fatal (3). Although treatment for lung cancer with ILD has been investigated, optimal regimens showing favorable efficacy and safety, particularly with low risk of chemotherapy-induced acute exacerbation of ILD (AE-ILD), have not been yet established. Several studies evaluated the efficacy and safety of carboplatin and paclitaxel (CP) doublet chemotherapy in patients with non-small cell lung cancer (NSCLC) with ILD (4-10). Minegishi et al. investigated 100 patients with NSCLC and ILD and reported that CP therapy was associated with markedly lower AE-ILD incidence than other regimens (4). CP therapy is currently considered as a relatively suitable regimen for treatment of this population, particularly in Japan.
Bevacizumab, a recombinant, humanized monoclonal antibody against vascular endothelial growth factor (VEGF), inhibits tumor angiogenesis and subsequent tumor growth and metastasis (11). A phase III, randomized controlled trial by the Eastern Cooperative Oncology Group (ECOG) compared the efficacy and safety of therapy with CP and bevacizumab (CPB) with CP therapy in patients with advanced non-squamous NSCLC (ECOG 4599 trial) (12). This pivotal trial demonstrated a marked improvement in objective response rate (ORR), median progression-free survival (PFS), and overall survival (OS) in the CPB group compared to the CP group (ORR=35% vs. 15%; PFS=6.2 months vs. 4.5 months; OS=12.3 months vs. 10.3 months). Additionally, similar tendencies were re-confirmed in the JO19907 trial in Japan (ORR=61% vs. 31%; PFS=6.9 vs. 5.9 months; OS=22.8 vs. 23.4 months) (13). According to the results of these trials, CPB therapy is a standard regimen for advanced non-squamous NSCLC. However, the eligibility or exclusion criteria of the protocols did not mention patients with pre-existing ILD; it is unclear whether CPB therapy is preferable for this population. Herein, we aimed to retrospectively evaluate the efficacy and safety of CPB therapy in patients with NSCLC with ILD.
Patients and Methods
This retrospective study was approved by the Institutional Review Boards of the Kanagawa Cardiovascular and Respiratory Center, National Cancer Center Hospital East, and Shizuoka Cancer Center (approval numbers: 26-18, 2014-391, and T26-35-26-1-2, respectively). We reviewed medical records of 208 consecutive patients who underwent CPB therapy as a first-line treatment regimen for advanced (clinical stage III or IV or recurrence after surgical resection) non-squamous NSCLC at each Institution between March 2007 and July 2013. Carboplatin at a dose of area under the concentration–time curve of 6 mg/ml×min, paclitaxel at a dose of 200 mg/m2, and bevacizumab at a dose of 15 mg/kg were administered to all patients on day 1 every three weeks. Three pulmonologists (Y. E., N. W., and H. K.) evaluated conventional or high-resolution computed tomography (CT) within 4 weeks before CPB therapy and identified 25 patients with pre-existing ILD. The diagnostic criteria for ILD were presence of chronic and bilateral reticular abnormality or ground-glass attenuation on pretreatment CT. According to the recent guideline for idiopathic pulmonary fibrosis (IPF) (14), we classified CT scans into three groups: usual interstitial pneumonia (UIP) pattern (subpleural and basal predominant reticular abnormality with honeycombing and no findings of atypical features of IPF), possible UIP pattern (subpleural and basal predominant reticular abnormality without apparent honeycombing), and pattern inconsistent with UIP. Chemotherapy-induced AE-ILD was diagnosed on the basis of the CT findings of bilateral ground-glass attenuation with/without focal consolidation superimposed on pre-existing interstitial shadows. Cases with apparent pulmonary infection, congestion, and carcinomatous lymphangiomatosis were excluded. To diagnose AE-ILD associated with chemotherapy, the duration between the last chemotherapy administration and AE-ILD onset was defined as 4 weeks or less. Objective tumor response was assessed as complete response, partial response (PR), stable disease (SD), progressive disease (PD), or not evaluable (NE) according to the Response Evaluation Criteria in Solid Tumors version 1.1 (15). Toxicities were graded using the Common Terminology Criteria for Adverse Events version 4.0 (16). PFS was defined as days from the first CPB administration to the confirmation of PD or death. OS was defined as days from the first administration to death or censoring. Patients were censored if alive on July 31, 2014. The Kaplan–Meier survival method was used to estimate median survival.
Results
Patients' characteristics. The patients' characteristics are listed in Table I. At first CPB administration, median age was 67 (range=53-79) years, 18 patients (72%) were aged ≥65 years. The majority of patients were men and had an ECOG performance status 0-1. All patients were current or former smokers. The UIP pattern on baseline CT was the most common (52%, 13/25). An emphysematous change was detected in 88% of patients. There were no patients with brain metastases at baseline. Two patients were confirmed as having pathological ILD and both the patients displayed UIP. Only one patient received systemic corticosteroid administration for the pre-existing ILD (20 mg/day prednisolone). Long-term oxygen therapy was administered to another patient. The others had not undergone any treatment for their ILDs.
Baseline characteristics of patients treated with combined carboplatin, paclitaxel, and bevacizumab therapy.
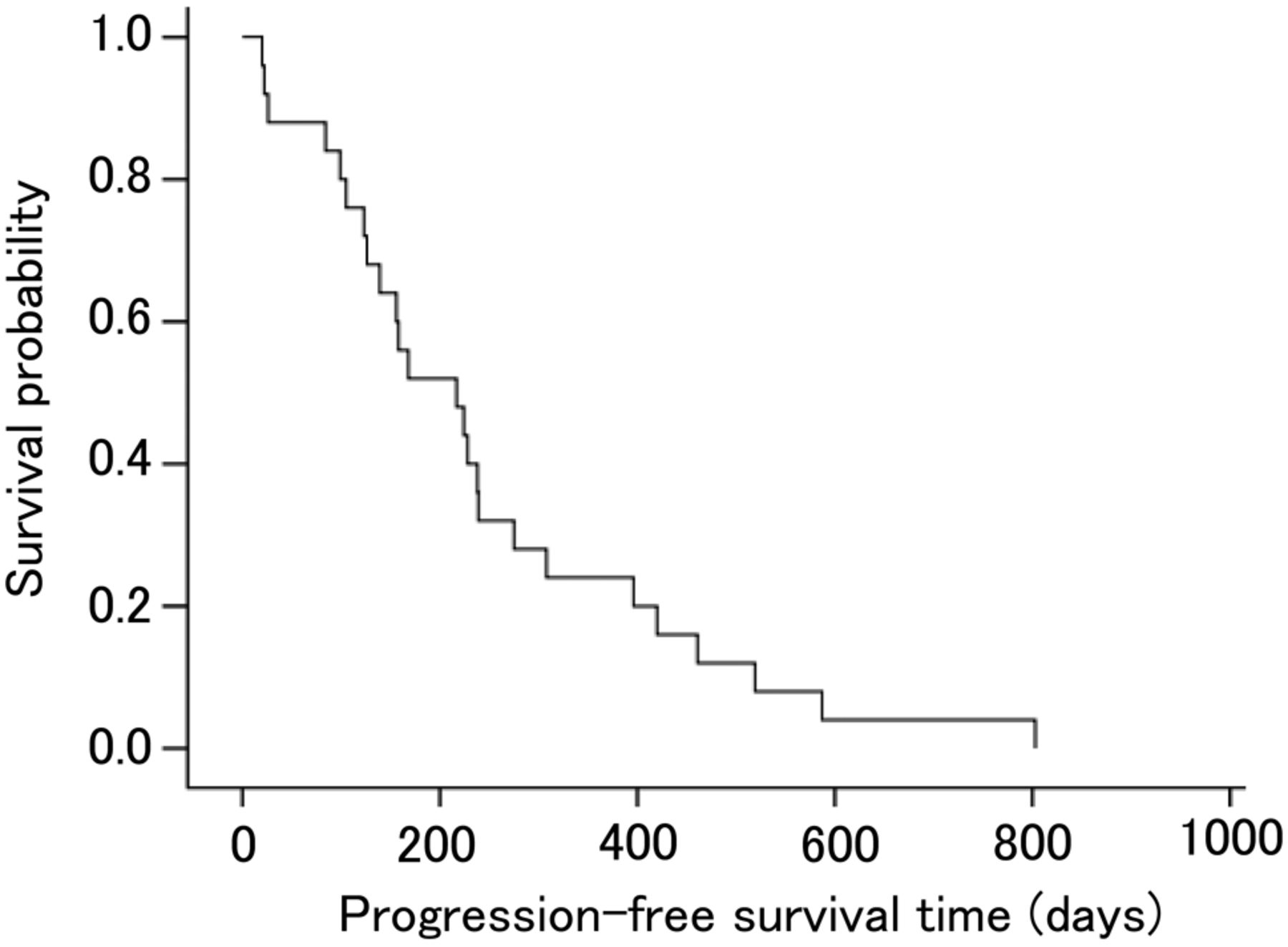
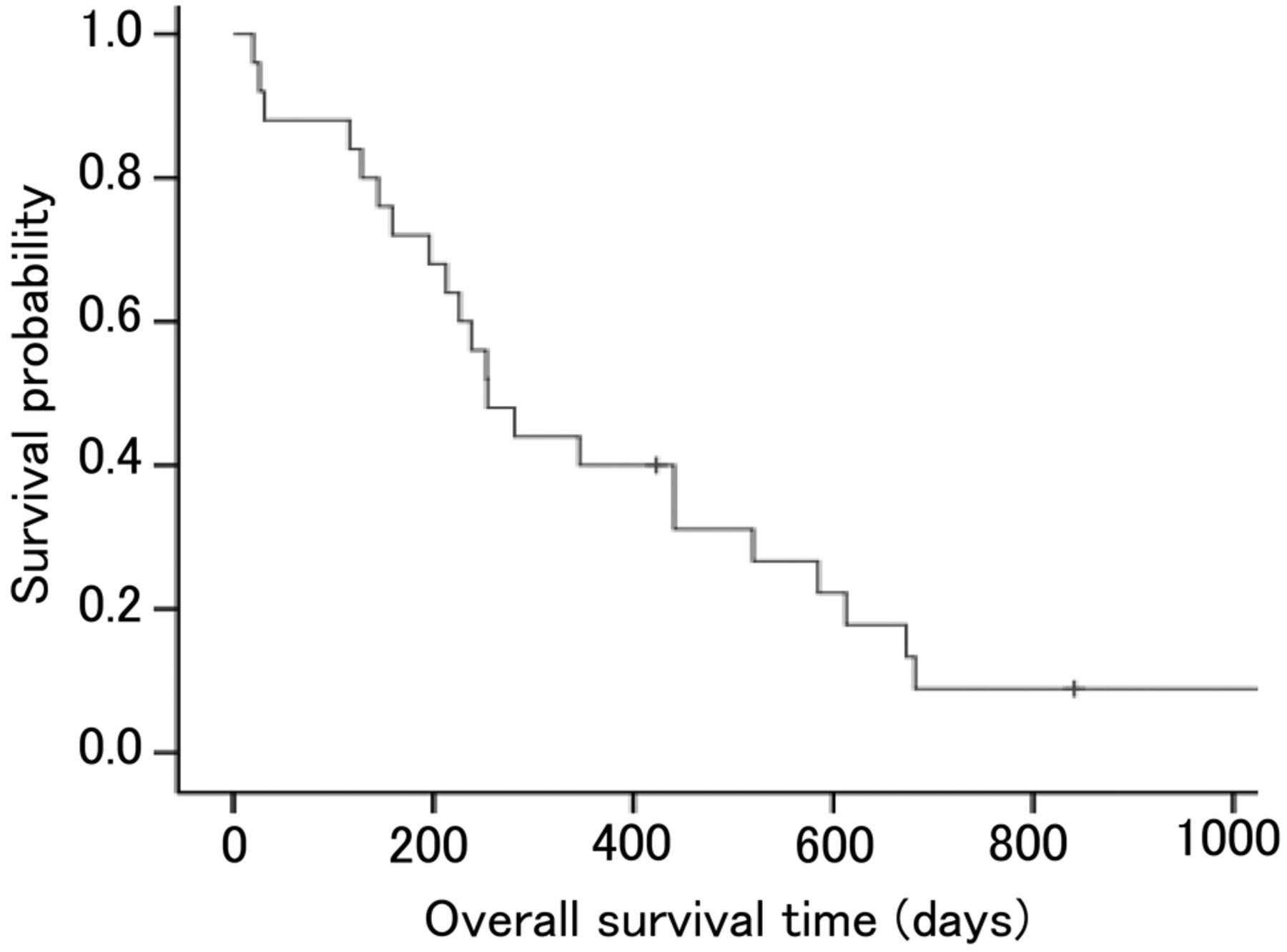
Efficacy. The CPB triplet chemotherapy was repeated for a median of four (range=1-6) cycles, and thereafter, 60% (15/25) of patients received a median of four (range=1-30) cycles of bevacizumab maintenance chemotherapy. Treatment responses were recorded as follows: PR: n=18; SD: n=3; PD: n=1; NE: n=3. The ORR was 72% [95% confidence interval (CI)=54-90%], the median PFS with first-line chemotherapy was 7.2 months (95% CI=3.6-10.8 months), and the median OS was 8.5 months (95% CI=6.1-10.8 months). The median follow-up time was 28.0 months. The Kaplan–Meier survival curves for PFS and OS are shown in Figures 1 and 2, respectively. The unadjusted 1-year survival probability was calculated as 40%.
Safety. Safety profiles are summarized in Table II. Grade 3 or more neutropenia (72%, 18/25) was most frequently observed as a severe adverse event. Febrile neutropenia was also observed in 20% of patients (5/25), and one patient died from this event. Additionally, another patient died after lung infection during a period of severe neutropenia. Chemotherapy-induced AE-ILD was observed in 12% of patients (3/25, 95% CI=0-25%; males, aged 53-75 years). Two of them underwent the event during the first cycle of CPB triplet chemotherapy. One patient developed AE-ILD during the first cycle of bevacizumab maintenance chemotherapy after four cycles of triplet chemotherapy. The pre-treatment CT scans showed the UIP pattern in two patients and pattern inconsistent with UIP (n=1). Although the three patients were treated with intravenous/oral corticosteroid therapy, one patient died. The patient who had the pattern inconsistent with UIP on pre-treatment CT died from respiratory failure 14 days after AE-ILD onset. The other grade 3 non-hematological toxicities were pulmonary embolism (n=1), fatigue (n=1), hypertension (n=1), and constipation (n=1). Three patients stopped the triplet chemotherapy because of peripheral sensory neuropathy, although the severity was less than grade 3.

Progression-free survival curve for 25 patients with non-squamous non-small cell lung cancer with pre-existing interstitial lung disease.
After CPB therapy, 13 patients received subsequent chemotherapies such as pemetrexed and S-1 monotherapy. Two patients developed AE-ILD induced by second-line pemetrexed monotherapy. Among the 25 patients in the entire cohort, there were 22 deaths during the follow-up. The causes were lung cancer (n=18), neutropenia-related infection (n=2), AE-ILD during CPB therapy (n=1), and AE-ILD during pemetrexed therapy (n=1).
Discussion
This study included 25 patients with advanced non-squamous NSCLC with pre-existing ILD who underwent CPB therapy for first-line treatment. The ORR was 72% (18/25; 95% CI=54-90%) and the median PFS was 7.2 months (95% CI=3.6-10.8 months). The most frequent severe adverse event was neutropenia (72%. 18/25), and 12% (3/25) of patients developed chemotherapy-induced AE-ILD during this treatment.
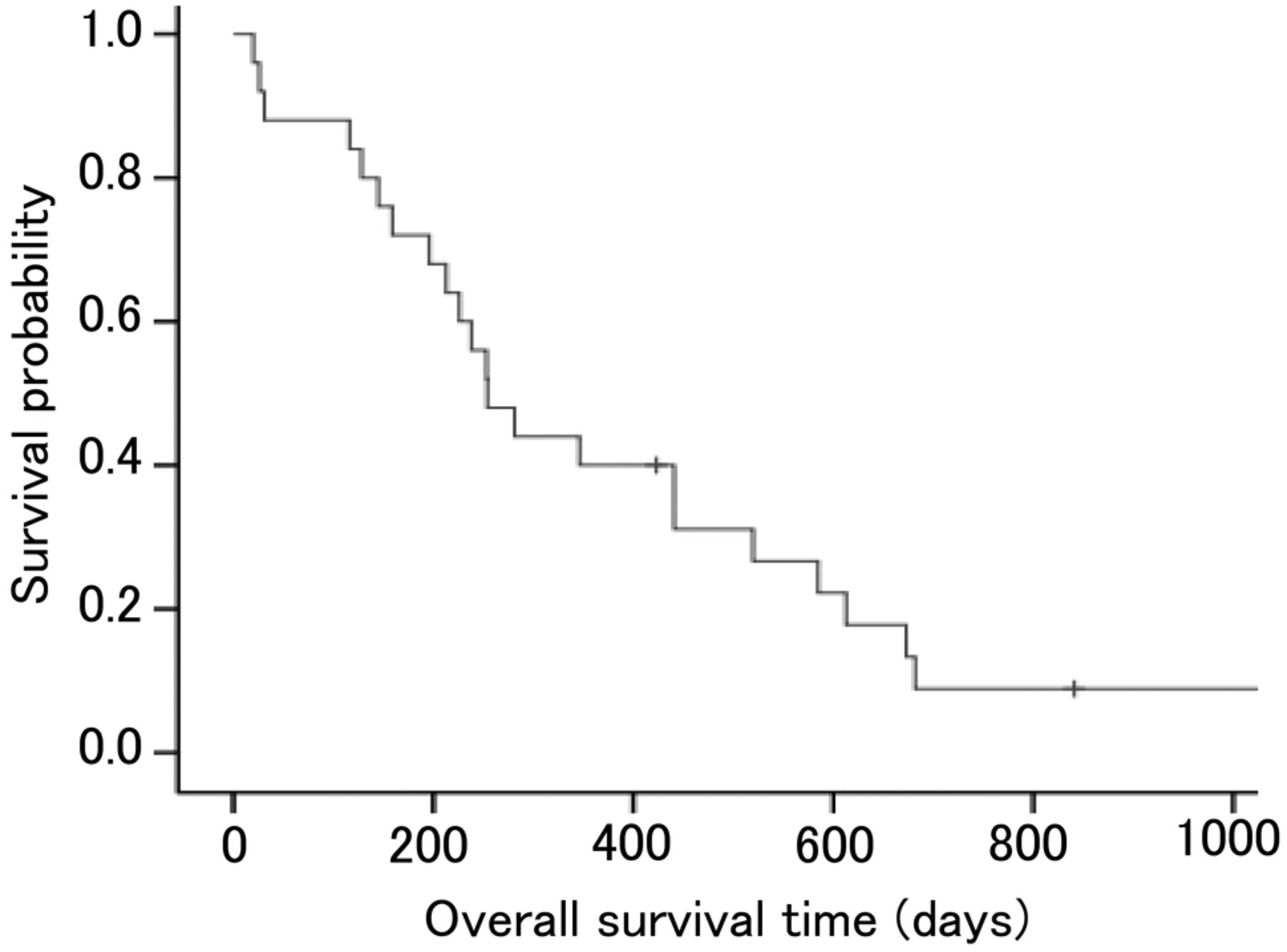
Overall survival curve for 25 patients with non-squamous non-small cell lung cancer with pre-existing interstitial lung disease.
Adverse events with grade 3 or more experienced by patients treated with combined carboplatin, paclitaxel, and bevacizumab therapy.
Several previous studies analyzed CP with/without bevacizumab therapy for patients with NSCLC and ILD (5, 7, 9, 10, 17). A data summary, including ours, is provided in Table III. Although directly comparing the results of these small studies is difficult, our efficacy profile (ORR of 72%; median PFS of 7.2 months) would be relatively favorable. Conversely, chemotherapy-induced AE-ILD by CPB therapy was observed in 12% of our patients (95% CI=0-25%). AE-ILD incidence on CP therapy was reported to be 0-26.7% (Table III), which was comparable to our results. This comparability suggests at least that the addition of bevacizumab to CP therapy may not raise AE-ILD risk. Nintedanib, a tyrosine kinase inhibitor that targets VEGF receptor, platelet-derived growth factor receptor, and fibroblast growth factor receptor, is suggested to reduce acute exacerbation incidences in patients with IPF (18). VEGF is a target of bevacizumab and nintedanib, and VEGF inhibition may have favorable effects on lung cancer and pre-existing ILD.
Comparison of previous studies for the combination chemotherapy of carboplatin plus paclitaxel with/without bevacizumab for patients with non-small cell lung cancer with pre-existing interstitial lung disease.
Two reports have evaluated CPB therapy for advanced non-squamous NSCLC patients with pre-existing ILD (17, 19). Shimizu et al. retrospectively compared 10 patients treated with CPB therapy against 11 patients treated with CP therapy (17). The ORR and median PFS were reported as 40% vs. 27%; 5.3 months vs. 4.4 months, respectively. Although these differences were not statistically significant, their results suggested that CPB therapy increased efficacy even in patients with ILD. Suzuki et al. reported on four patients who underwent CPB therapy (19). Interestingly, one patient in their study received 10 cycles of bevacizumab maintenance chemotherapy, and achieved long PFS of 487 days. In our cohort, bevacizumab maintenance chemotherapy was administered to 60% (15/25) of patients, and four received 10 or more cycles without severe complications. Bevacizumab maintenance may be feasible for patients with ILD; the significance of this should be evaluated in future studies.
Several adverse events other than AE-ILD were observed in our cohort. The most common one with grade 3 or more was neutropenia, which occurred in as many as 72% (18/25) of patients. Unfortunately, two patients died from neutropenia-related infection (febrile neutropenia and lung infection). As demonstrated in the ECOG 4599 trial (12), the addition of bevacizumab to CP therapy could increase the frequency of severe neutropenia. We should be careful with neutropenia as well as AE-ILD when using this regimen.
The median OS was very close to the median PFS in this study and may have been influenced by several factors. Second-line chemotherapy was administered to only 52% (13/25) of our patients. Although changes in performance status and quality of life were not evaluated in this study, the first-line CPB therapy might degrade such factors and lead to treatment termination in these patients. In addition, the efficacy of second- or subsequent-line chemotherapies might not be effective, or chemotherapy options may be limited because of AE-ILD risks. In fact, two patients in our study developed AE-ILD induced by second-line pemetrexed monotherapy. It would be challenging to determine whether the benefit of chemotherapy exceeded AE-ILD risks in this population.
There are several important limitations to this study. Firstly, this was a retrospective study with a small number of patients. Secondly, we could not fully exclude the possibility of other diseases with ILD- or AE-ILD-like findings, such as carcinomatous lymphangiomatosis and infectious diseases. Few patients underwent bronchoalveolar lavage or lung biopsy, although these invasive procedures are difficult to apply to every patient with advanced lung cancer in clinical settings.
In conclusion, our data suggest that CPB therapy for first-line treatment of non-squamous NSCLC has a relatively favorable efficacy and feasibility even in patients with ILD, although the risk of fatal complications, including severe neutropenia and AE-ILD, should be fully monitored.
- Received April 3, 2015.
- Revision received April 23, 2015.
- Accepted April 27, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}