


Abstract
Background/Aim: In the past decade, the human Nottingham histological grade (NHG) has been applied to canine mammary carcinomas (CMC). The Nottingham Prognostic Index (NPI) enables identification of more aggressive human breast cancer. The prognostic value of grading parameters and NPI has never been detailed in CMC. The aim of the present study was to assess the prognostic value of NHG, its parameters and NPI. Materials and Methods: Univariable and multivariable analyses were used to assess the prognostic value of NHG, its parameters and NPI in a cohort of 59 dogs with CMC. Results: Short disease-free interval and overall survival were associated with higher NHG, particularly of grade III. Only high nuclear pleomorphism score was significantly associated with poor survival. NPI exhibited a strong predictive value for disease progression. Conclusion: NHG, nuclear pleomorphism and NPI have prognostic value in CMC. Nuclear pleomorphism is an independent prognostic factor. Evaluation of nuclear pleomorphism should be included in routine pathology reports.
Although the body of evidence on biological markers of canine mammary tumors has increased tremendously in the last few years, the individual prognosis and clinical management of female dogs affected by the disease are still challenging topics, emphasizing both the need for an in-depth evaluation of the existing prognostic factors and the search for new ones (1).
In the past decade, the human Nottingham histological grade (NHG) has been applied (with or without modifications) to canine mammary carcinomas (CMC) (2-8). NHG is based on the assessment of three morphological parameters: tubule formation, nuclear pleomorphism and mitotic count (9). Each parameter of the NHG is scored from 1 to 3 and the total combined score defines the grade (Figure 1). Both tubule formation and mitotic count are evaluated semi-quantitatively using thresholds, but nuclear pleomorphism, classified according to the size of the nuclei and their variability, is scored in a much more subjective way (9, 10).
Despite two recent studies demonstrating that the NHG with modifications provided independent prognostic information (5, 8), others only detected an association with survival when grades were grouped -e.g. grade I plus grade II versus grade III (2, 6)- thus raising the issue of the validity of a three-tier classification for CMC grading. Moreover, the individual prognostic value of each of the NHG parameters to our knowledge has never been detailed in CMC.
In fact, it has been stressed that in order to be universally accepted in CMC, the prognostic legitimacy of a grading method must be validated in various prospective cohorts (1, 11).
In human pathology, the NHG is highly correlated to survival and has been included in a prognostic index, called the Nottingham Prognostic Index, NPI (12, 13). This index allows stratification of patients with breast cancer (14), and incorporates three independent prognostic factors: tumor size, lymph node stage and histological grade (12, 15).
The tumor size corresponds to the largest diameter, determined by the pathologist during the macroscopic examination of fresh specimens or the microscopic examination of very small invasive carcinomas (16). In veterinary medicine, the tumor size, also defined as the largest diameter determined either by the clinician or by the pathologist, has been integrated into the World Health Organization (WHO) staging of CMC (17-19), and there is general agreement that it has prognostic significance (20, 21).

Nottingham histological grade: criteria for scoring each grading parameter [adapted from Elston and Ellis (9)]. *Cells similar to normal surrounding parenchyma; **counted in 10 high-power fields, field diameter of 0.55 mm.
Lymph node staging in human breast cancer is also a three-tier system, depending on the number of metastatic lymph nodes and their location (13). In veterinary medicine, the presence of regional lymph node metastases is also relevant for disease staging, but the number of positive nodes is disregarded (18). Other differences reside in the diagnostic imaging of regional lymph nodes and the sentinel lymph node examination, which are routinely assessed in women but not routinely performed in veterinary medicine (22). In dogs, the recommended procedures depend on the anatomical location of the primary tumor. In all cases, regional lymph nodes should be carefully evaluated during the pre-surgical physical examination (21); for axillary nodes, cytological evaluation is advised when nodes are enlarged and surgery should be performed when metastatic disease cannot be excluded (23). In contrast, the superficial inguinal nodes are usually dissected during the gross examination of all the regional caudal or radical unilateral mastectomy specimens and routinely submitted for histological examination (21, 23, 24). Several authors have confirmed that the histological evidence of metastases in regional lymph nodes at the time of diagnosis is a significant prognostic factor (25-27).
The presence of vascular invasion has been also considered as evidence of the metastatic potential of CMC (28). In human medicine, vascular invasion closely correlates with regional lymph node involvement and local recurrence (16). According to some authors, vascular invasion may be a valuable surrogate for the lymph node stage, when nodes were not removed, while others have stressed that vascular invasion adds prognostic information to histological grade and tumor size in women with node-negative breast carcinoma (16, 29). In CMC, the presence of neoplastic emboli in vessels also has an independent role in survival (30), and it was recently reported that vascular invasion (associated or not with regional lymph node metastases) was associated with short survival times (31). Therefore, it is reasonable to assume that the assessment of vascular/lymph node invasion at the time of diagnosis may be a valuable estimator of the metastatic capacity of a tumor (28, 31, 32).
Distribution of grades by histological subtype of 59 canine mammary malignant tumors.
Scoring of each grading parameter of the Nottingham system in 59 canine mammary malignant tumors.
Whilst, as far as we are aware of, no study has ever reported a prognostic index in CMC, it has been suggested that a combination of factors could strengthen the prognostic information (17, 30). Moreover, a comprehensive evaluation of the individual prognostic value of each grading parameter for NHG in CMC has never been performed as far as we know. Therefore, in this study we aimed to: i) evaluate the prognostic value of NHG in a cohort of female dogs with CMC; ii) analyze each of the three grading parameters regarding their individual prognostic impact; iii) compute the NPI and assess its sensitivity and specificity in predicting postsurgical disease progression in CMC.
Materials and Methods
Selection of cases, histological analysis and follow-up. A cohort of 59 female dogs with spontaneous CMC treated at the veterinary clinic of Institute of Biomedical Sciences Abel Salazar, University of Porto was retrospectively selected. Dogs included in this study underwent surgery as the only treatment and the surgical procedure was performed in all the cases by the same surgeon. Owners provided consent for surgery with curative intent and 2 years' follow-up, as well as for the use of the material for research purposes. Of these female dogs, 33 were treated between 2008 and 2012 and the remaining 26 cases were selected from a previous series based on the presence of a single malignant tumor (1). The selection of cases and their histological study were blinded to survival outcomes, thus following recent guidelines in veterinary oncology (22). Dogs with distant metastases at the time of the diagnosis were excluded.

Kaplan–Meier curves of disease-free interval (DFI) and overall survival (OS) of cases included in each WHO tumor-size category. Female dogs with largest tumor diameter <3 cm had better survival outcomes but no statistical difference seemed to exist between the other two categories regarding DFI (log-rank test, p=0.03 for DFI; p=0.04 for OS). Censoring is indicated by vertical marks.

Kaplan–Meier plots comparing the disease-free interval (DFI) and overall survival (OS) of 59 female dogs according to largest tumor diameter. Cases with ≥2.9 cm were associated with poor survival (log-rank test, p=0.009 for DFI and p=0.02 for OS). Censoring is indicated by vertical marks.
The histological diagnosis was reviewed by two pathologists (MS and PDP) using the criteria of the WHO classification (33). For each case, the tumor size and the histological evidence of vascular invasion/regional lymph node metastases at the time of diagnosis were recorded. The tumor size was categorized according to WHO criteria (T1<3 cm, T2 3-5 cm and T3>5 cm) and to a previously defined cut-off (<2.9 cm and ≥2.9 cm) (31). The NHG (Figure 1) was performed by two pathologists (MS and PDP) and when discrepancies occurred for a particular parameter, a consensus was reached. Only epithelial cells were considered for NHG. In the subgroup of 10 dogs with multiple malignant tumors, a reference lesion was assigned in accordance to published approaches for synchronous breast cancer and CMC (6, 34-36). In brief, the reference lesion was considered as the tumor presenting vascular invasion (primary criterion) or the one with the largest diameter (secondary criterion) and only its NHG and NPI were considered for the statistical analysis.
NPI was adapted from (15), and computed as: NPI=[tumor size (cm)×0.2]+NHG (1, 2 or 3 respectively for grades I, II and III)+evidence of vascular invasion/regional lymph node metastases (1 or 2 if absent or present, respectively).
The schedule and the protocol of clinical evaluations before the surgery and during the follow-up period were performed as previously described (6). The disease-free interval (DFI) was calculated from the date of surgery to the diagnosis of disease progression (recurrence or metastasis, with cytological or histological confirmation). Overall survival (OS) was calculated from the date of surgery to the date of animal death/euthanasia due to metastasis. Animals that died or were euthanized for unrelated causes and those that were lost to follow-up were censored at the time of death and at the data of their last follow-up examination, respectively. Complete necropsies were performed, after owner consent had been obtained, on all the dogs that died spontaneously or were euthanized, and suspected metastatic lesions were confirmed by histopathological examination.
Statistical analysis. The association between histological sub-type and grade was assessed using the Fisher's test. Disease-specific survivals were determined using Kaplan–Meier product-limit estimates, with log-rank (Mantel-Cox) tests used to estimate differences in survival fractions according to the NHG (I, II and III) and the score of each grading parameter (1, 2 and 3). A similar approach was taken considering the final combined grading scores (3 to 9) to categorize tumors of low grade (final score ≤6) and of high grade (final score ≥7). Regarding the mitotic score, we also considered tertile values (or 3-quantiles, i.e. the two thresholds that divide the ordered distribution of mitotic counts into three parts) as alternative cut-offs [i.e. scores 1, 2 and 3, respectively for <11, 11-23 and >23 mitotic figures per 10 high-power field (each field with a diameter of 0.55 mm)].
Receiver operating characteristic (ROC) curves were used to assess the sensitivity and specificity of the veterinary-adapted NPI for predicting tumor progression at 12 months postsurgery. The optimal cut-off was defined according to the maximization of sensitivity and specificity. Using the optimal cut-off, Kaplan–Meier curves were generated and compared using the log-rank test. Cox hazard's regression model was used to evaluate the independent prognostic role of various pathological factors in multivariable analysis. As vascular invasion, tumor size and NHG were components of the NPI, when this index was included in the multivariable analysis, their components were excluded from the model, in order to avoid co-linearity.
In all cases, a p-value of less than 0.05 was considered significant. Statistical analyses were performed with R Development Core Team software, version 2.7.1 (Vienna, Austria) and IBM SPSS Statistics, version 22 (IBM, New York, NY, USA).
Results
Fifty-nine female dogs aged from 6 to 18 years (mean of 10.9 years) were included. Out of these, 38 animals presented simple carcinomas (18 tubulopapillary, 17 solid, 1 anaplastic, 1 squamous cell and 1 mucinous carcinoma), 18 had complex carcinomas and 3 had carcinosarcomas. The largest diameter of the tumors ranged from 0.5 to 15 cm, being 2.9 cm or larger in 26 cases (44%). According to the WHO tumor size system, 35 were T1, 11 were T2 and 13 were T3. In all the cases, surgical margins were considered histologically complete. At the time of diagnosis, 17 cases (29%) presented vascular/regional lymph node invasion. Postsurgical progression was diagnosed in 17 cases (in 14 out of 17, the diagnosis of recurrence or metastasis occurred within the first 12 months of the follow-up period). tumors that progressed included different histological subtypes: seven solid carcinomas, five complex, three tubulopapillary, one anaplastic carcinoma and one carcinosarcoma. During the follow-up, 14 dogs (24%) died or were euthanized due to progressive disease, 29 (49%) were alive and free of disease at 24 months after the surgery, whilst 16 dogs (27%) were censored before the end of the follow-up period, being lost to follow-up or which had died from non-malignancy-related causes (in these, the median follow-up time was 13 months).
Animals older than 10.9 years (median age in this series) had increased risk for developing recurrence and metastases (p=0.01). The WHO category of tumors T1<3 cm was associated with better survival times, but no significant difference seemed to exist between the two other size categories regarding DFI (Figure 2). The cut-off of 2.9 cm allowed for stratification of tumors with significant differences in survival: those with tumor size <2.9 cm had 21 and 22 months of DFI and OS, respectively, whereas those with size ≥2.9 cm had 15 and 18 months of DFI and OS (p=0.009 for DFI and p=0.02 for OS) (Figure 3). The evidence of vascular invasion or regional lymph node metastases at the time of diagnosis was associated with shorter DFI and OS (p<0.0001).
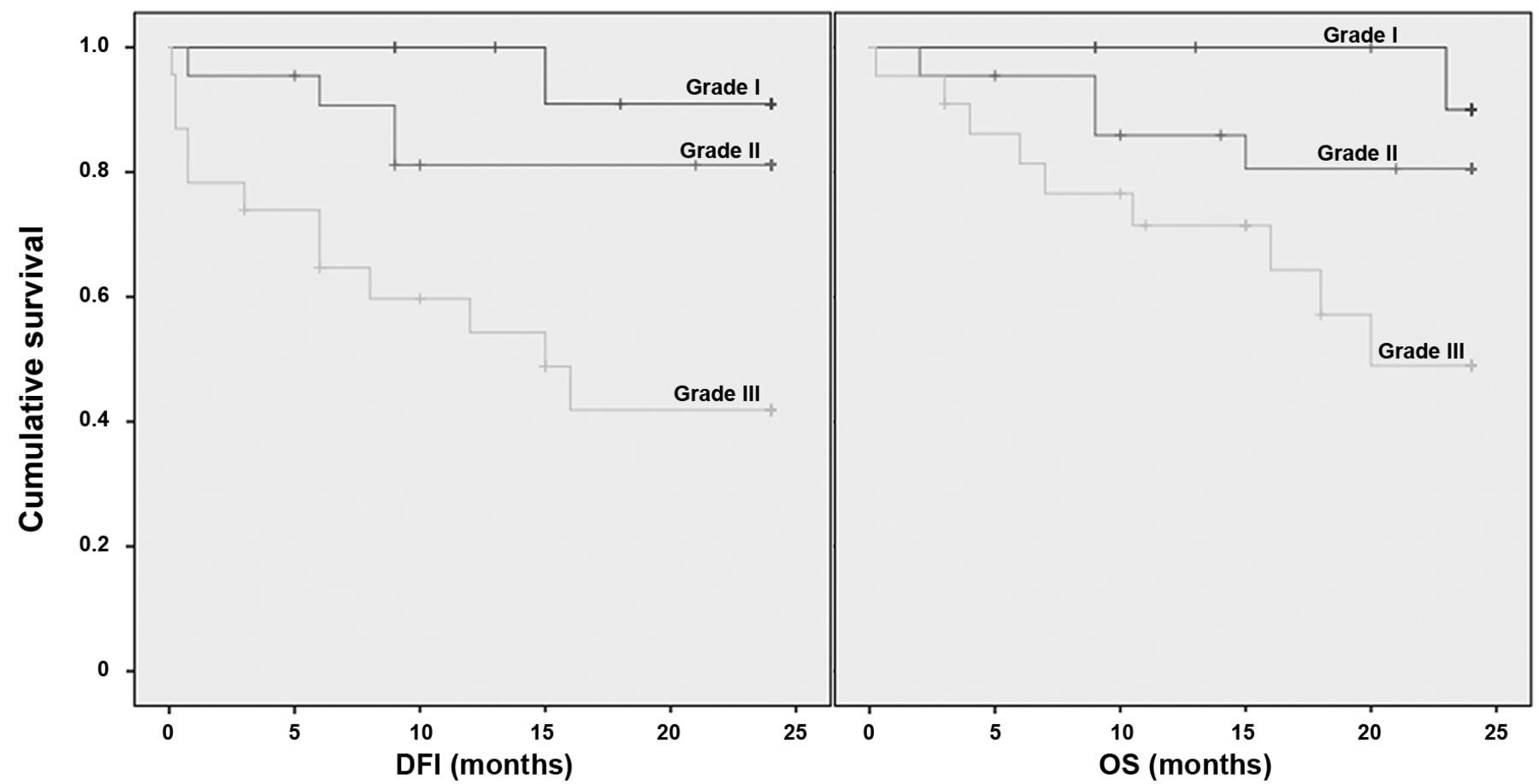
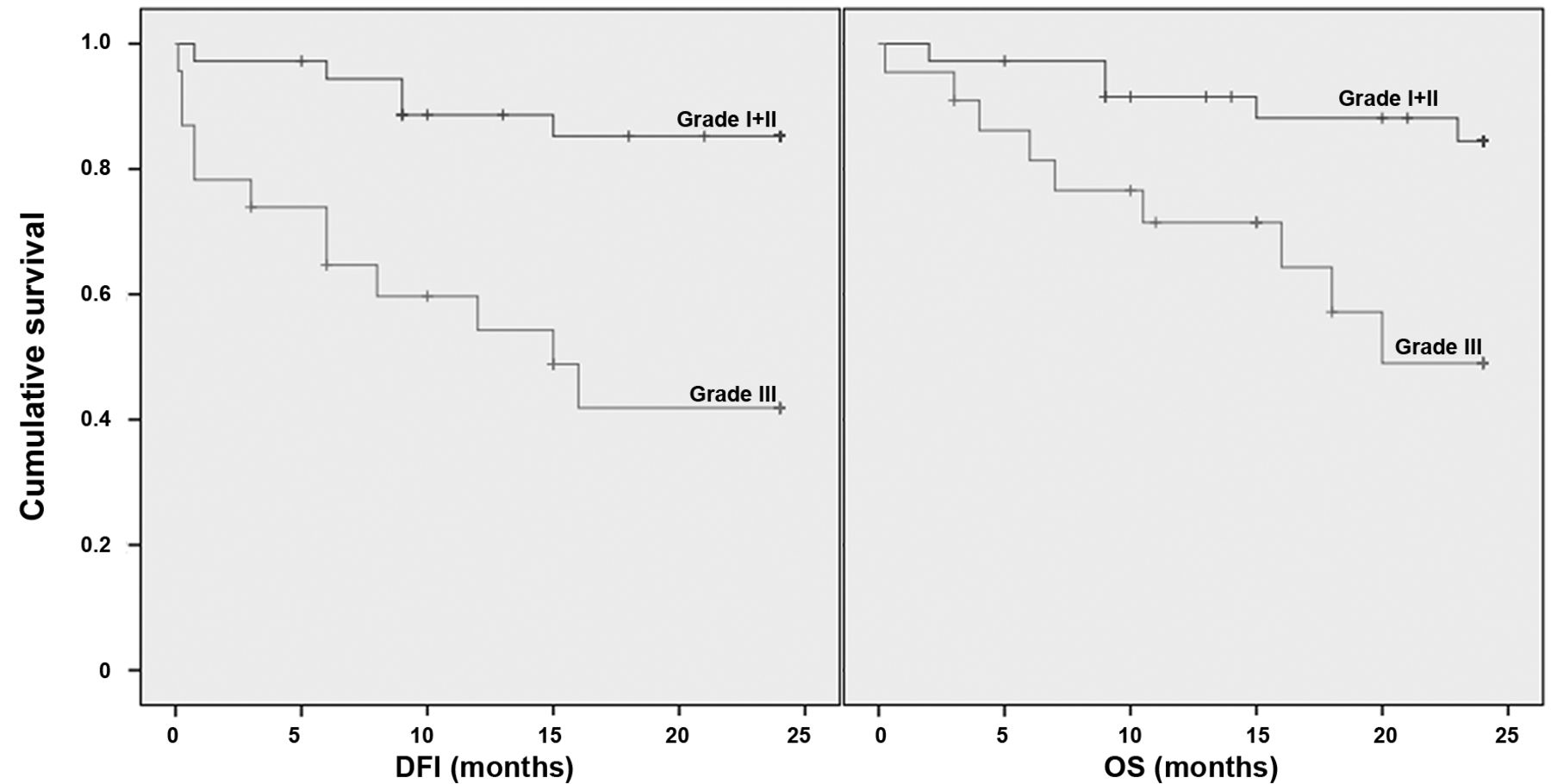
Regarding the NHG, 14 (24%) tumors were grade I, 22 (37%) grade II and 23 (39%) were grade III. A final combined score of 6 or less (considered as low-grade tumor) was computed for 22 cases (38%), whilst 37 (62%) cases had a combined score of 7 or more (considered as high-grade tumor). The distribution of grades for each histological subtype and the scores of NHG parameters are presented in Table I and II, respectively. An association between the histological subtype and grade was observed (p=0.01). Notably, all solid carcinomas and carcinosarcomas were graded II and III. However, no significant association existed between histological sub-types and survival, even when the simple carcinomas were compared to all the other groups together. DFI and OS were significantly related to NHG (p=0.002 and p=0.02, respectively) (Figure 4). The mean DFI for dogs with tumor of grades I, II and III was 23, 21 and 14 months, respectively, whereas their mean OS was 24, 21 and 17 months. When evaluating the DFI, the prognosis strength of a two-tier classification (high and low grades determined by the final score) was slightly lower (p=0.04) than that of the original three-tier system of NHG (p=0.002), and that classification was not significantly associated with OS (p=0.1). When cases graded I and II were grouped and compared with those of grade III, the former presented significantly longer DFI (p<0.0001) and OS (p=0.008) (Figure 5).

Disease-free interval (DFI) and overall survival (OS) of 59 female dogs with grade I, grade II and grade III mammary malignant tumors. Significant differences existed between the three curves (log-rank test, p=0.002 for DFI and p=0.02 for OS). Censoring is indicated by vertical marks.

Kaplan–Meier analyses of disease-free interval (DFI) and overall survival (OS) among 59 female dogs with malignant mammary tumors. Animals with tumors graded I or II had a significantly longer DFI and OS when compared to animals with tumors graded III, according to the Nottingham histological grading method (log-rank test, p<0.0001 for DFI and p=0.008 for OS). Censoring is indicated by vertical marks.
Among the NHG components, nuclear pleomorphism emerged as a statistical significant predictor of the outcome, with longer OS (p<0.0001) and DFI (p<0.0001) in animals bearing tumors with nuclear pleomorphism scores of 1 or 2, as opposed to those with score 3 (Figure 6). Tubule formation and mitotic counts had no prognostic significance, even when scores 1 and 2 were grouped and compared to score 3, or when score 1 was compared to scores 2 plus 3. No association with outcome was observed when tumors were scored according to the tertile values of the mitotic counts.
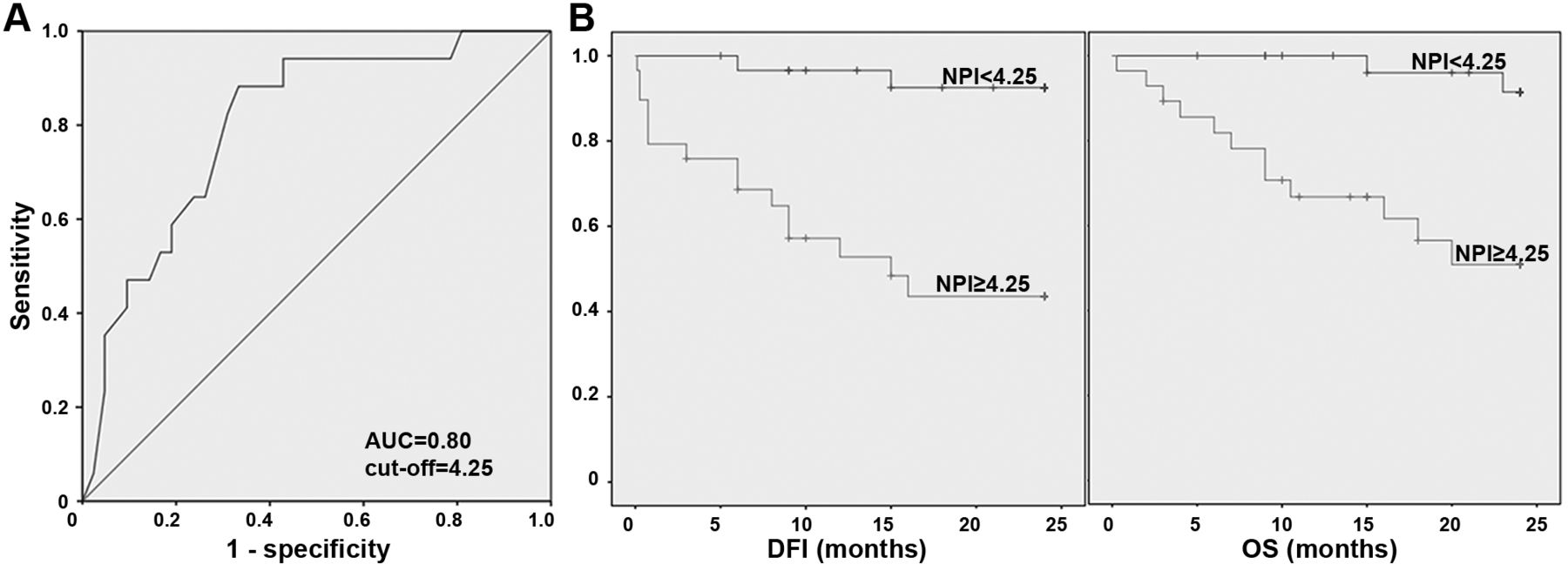
The mean veterinary-adapted NPI was 4.2±1.4, ranging from 2.1 to 7. According to the ROC curve results, the performance of this index in identifying tumors progressing in the first 12 months post-surgery was moderately accurate as the area under the ROC curve (AUC) was 0.80 (95% confidence interval=0.68-0.92) (Figure 7A) (37). An optimal veterinary-adapted NPI cut-off value of 4.25 was defined based on the maximal pair of sensitivity and specificity values (sensitivity of 88% and specificity of 67%). High cut-off levels were associated with high specificity, with an obvious decrease of sensitivity (for instance, an NPI cut-off of 5.3 was associated with 91% specificity and 47% sensitivity). In order to perform a survival analysis, cases were grouped by the previously determined NPI cut-off value. Cases with an NPI of 4.25 or more were associated with poorer outcome (Figure 7B).
Taking DFI and OS as dependent variables and selecting a set of independent pathological variables including tumor size (either defined as a continuous variable or with categories defined by the 2.9 cm cut-off), vascular invasion, nuclear pleomorphism (score 1 plus 2 versus score 3), and NHG (I plus II versus III)-the multivariable Cox hazard's regression selected two independent covariates, in decreasing order of significance: i) nuclear pleomorphism (p<0.0001 for DFS and p=0.002 for OS); ii) vascular invasion (p=0.01 for DFS and p=0.03 for OS). When NPI and nuclear pleomorphism were used as covariates in the Cox regression model, the two variables were independent predictors of survival.
Discussion
When examining a CMC, the pathologist is expected to provide relevant information with prognostic significance. This goal could be achieved by tumor grading, since it has long been known that the microscopic appearance of tumors and their biological behaviour are associated (16, 38). In recent years, the NHG has been applied (with or without modifications) for grading CMC by several investigators (2-4, 7, 8, 28, 35, 39-41), but data regarding its prognostic value are still relatively limited, namely when compared to data of human breast cancer.
This study analyzed the relationship between the NHG and survival in a cohort of animals with CMC and, to the best of our knowledge, this is the first study where the association between survival and each parameter of the NHG was systematically assessed. In our cohort, a high proportion of tumors were graded II and III, which is in line with previous studies (3, 6). In contrast, other survival studies had a higher proportion of grade I tumors (2, 5). Since the selection of cases was completely blinded to histological features and follow-up data, it is likely that the high proportion of grade II and III represents an intrinsic feature of this cohort. At the same time, it should be stressed that in our cohort there was an over-representation of female dogs with a single CMC and, ultimately, this could represent a bias of selection. This should not affect our results because solitary and multiple tumors have no significant differences in conferring survival (25, 42). In fact, the prevalence of tumor progression (29%) and cancer-associated death (24%) observed in our study are within the published range of values (2, 5, 25).
Herein, the histological type and grade were significantly associated, corroborating previous studies (2, 3, 5, 7). Such association has been justified with the evaluation of tubule formation that is typically scored 3 in solid carcinomas-a histological type often associated with a worse prognosis (5).
Regarding the NHG, it was associated with disease progression and cancer-related death, especially when grade I and II tumors were compared to grade III; this is also in line with previous findings (2, 6). However, in the present study, we assessed for the first time the role of each NHG parameter. In this regard, only nuclear pleomorphism stood as relevant, with a significant difference in survival between animals bearing tumors scored 1 or 2 and those affected by score 3. Notably, the multivariable survival analysis also highlighted nuclear pleomorphism as an independent prognostic factor, in detriment of NHG. This suggested that only two scores of nuclear pleomorphism should be considered for an accurate prognostic assessment of CMC. The use of a two-tier system for classifying nuclear pleomorphism could also increase the modest interobserver agreement associated with the use of NHG three scores criteria (31). Our results also suggest that tubule formation and mitotic counts may dilute, rather than strengthen the prognostic value of the NHG. The lack of association between mitotic counts and patient outcomes corroborates previous findings (6, 30), although it seems to contradict other reports, where higher proliferative activities were associated with poorer outcomes (17, 30, 39, 43). However, the latter studies used immunohistochemical techniques for the detection of proliferative markers (e.g. Ki-67 and Proliferating Cell Nuclear Antigen) rather than mitotic counts. In routinely-stained slides, it may be difficult to identify mitotic figures, particularly in tumors with high apoptotic activity or in those with large areas of necrotic tissue (10, 44). Furthermore, the mitotic count of the NHG is largely dependent on the sampling strategy (selection of high-power fields by the observer) and the cellularity of the tumor (44). Considering that the distribution of the mitotic count scores was skewed (half of the cases were score 3), we also analyzed this feature with tertile boundaries, following an approach previously used in human and veterinary pathology (45, 46). Nevertheless, such analysis also failed to improve the separation of survival plots obtained with the original thresholds of NHG.

Disease-free interval (DFI) and overall survival (OS) curves of female dogs with tumors scored 1 or 2 in nuclear pleomorphism compared to female dogs with tumors scored 3 in this parameter. Nuclear pleomorphism was significantly associated with survival (log-rank test, p<0.0001 for DFI and OS). Censoring is indicated by vertical marks.

A: Receiver operating characteristic curve for tumor progression in 59 female dogs based on the veterinary-adapted Nottingham Prognostic Index (NPI). The NPI had good discriminative power between tumors that progressed within the first 12 months post-surgery and those that did not progress. B: Kaplan–Meier plots of disease-free interval (DFI) and overall survival (OS) among 59 female dogs with malignant mammary tumors grouped by the NPI cut-off. NPI ≥4.25 was associated with poor survival outcomes (log-rank test, p<0.0001 for DFI and p=0.001 for OS curves). Censoring is indicated by vertical marks.
Tubule formation is closely related to the differentiation of epithelial cells (23) and with the histological diagnosis (5). In agreement with previous studies (27, 42), our results failed to demonstrate an association between the histological type and survival. To the best of our knowledge, no other study has ever assessed the association between tubule formation as defined in NHG and prognosis in CMC. In the veterinary literature, only a recent study devoted to feline mammary carcinomas reported a weak association between tubule formation and survival (46).
In this cohort of dogs, we also assessed the NPI; to the best of our knowledge, this is the first report of its use in CMC. Notably, this index exhibited a strong discriminative power for identifying cases which progress in the first 12 months after surgery. Therefore, it seems to be useful for CMC, and it could also be included in the pathologist report. In our case, we introduced some modifications to the original NPI. Considering that vascular invasion was as an independent prognostic factor in our cohort, we surrogated the lymph node stage from the original formula with the histological evidence of vascular invasion or regional lymph metastases; all the remaining items of NPI (size and NHG) were maintained. It should be noted that the influence of tumor size on survival is well-acknowledged (21). Even if we have shown the utility of a veterinary-adapted NPI, we anticipate that further modifications to the NPI could be introduced. According to our multivariable analysis, the inclusion of nuclear pleomorphism could increase its prognostic value. At this point, we have already highlighted the value of this index, but a formula more fitted to CMC must be validated, and perhaps upgraded by larger prospective studies.
In conclusion, this study demonstrated that the NHG is associated with survival outcomes in CMC. Regarding its components, nuclear pleomorphism was the only parameter associated with survival, retaining its prognostic significance in multivariable analysis. We also showed that a veterinary-adapted NPI provides valuable data for the prediction of post-surgical disease progression. We suggest that nuclear pleomorphism should be classified by a two-tier system and its score should be included in routine pathological reports. Efforts to further validate the use of NPI (or other similar prognostic indices) in CMC would be helpful so that adjuvant therapies could be assigned to properly selected cases, similar to the current standards in human breast cancer care.
Footnotes
Conflicts of Interest
None of the Authors has any financial or personal relationships that could inappropriately influence or bias the content of this article.
- Received March 31, 2015.
- Revision received April 29, 2015.
- Accepted May 4, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.