


Abstract
Aim: To report on clinical outcomes of prostate cancer patients treated with hypofrationated radiotherapy employing a simultaneous integrated boost strategy. Patients and Methods: A consecutive series of 104 patients affected with prostate cancer was treated with intensity-modulated radiotherapy using a hypofractionated schedule and a simultaneous integrated boost consisting of 70 Gy (2.5 Gy daily) to the prostate gland, 63 Gy to the seminal vescicles (2.25 Gy daily) and 53.2 Gy to the pelvic nodes (1.9 Gy daily) when needed, delivered in 28 fractions. All patients underwent image-guided radiotherapy procedure consisting of daily cone-beam computed tomography. Results: After a median observation time of 26 (range=15-48) months, the 3-year biochemical failure-free survival was 96.5% [95% confidence interval (CI)=89%-98%], 3-year cancer-specific survival was 98.5% (95% CI=91%-99%) and 3-year overall survival was 96.5% (95% CI=89%-98%). The gastrointestinal and genitourinary toxicity profiles were mild with fewer than 2% of grade 3 events. Erectile function was partially affected by radiation in men potent at baseline. Conclusion: Hypofractionation delivered with intensity-modulated radiotherapy and a simultaneous integrated boost approach proved to be a safe and effective treatment option for patients with prostate cancer. Patients with a preserved baseline erectile function experience a decrease in functionality correlated with the mean dose received by penile bulb.
External-beam radiation therapy (EBRT) is a common treatment option for patients with prostate cancer (1). Strong clinical evidence raised up for this therapeutic approach within all risk groups either as exclusive approach or combined to androgen deprivation therapy (ADT) (2). EBRT delivered through conventional fractionation and dose escalation is able to provide consistent biochemical control and has a mild toxicity profile (3). Nevertheless, since the α/β ratio of prostate cancer has been demonstrated to be lower than that of surrounding normal tissues, hypofractionation has been proposed as a suitable option for RT delivery (4). Prospective phase III trials testing hypofractionation in patients with prostate cancer showed clinical isoefficacy compared to conventionally fractionated schedules (5, 6). Moreover, recent technological advances led to the possibility of safe delivery of high-dose hypofractionated EBRT for patients with prostate cancer (7). Specifically, intensity-modulated radiotherapy (IMRT) provides conformal and homogeneous target coverage and simultaneous sparing of organs at-risk, also allowing for the concomitant delivery of different nominal doses per fraction to different target volumes employing a simultaneous integrated boost (SIB) approach (8). This is noteworthy in prostate cancer RT as in other oncological scenarios (9, 10). Image guidance has further improved EBRT ballistic precision, minimizing geometric uncertainties and diminishing unintended irradiation of normal tissue (11). We herein present clinical results of a consecutive series of patients with prostate cancer treated with image-guided IMRT using a hypofractionated schedule and a SIB approach in case of multiple target volumes, reporting on biochemical control and treatment-related toxicities.
Patients and Methods
Inclusion criteria. Patients affected with organ-confined or locally advanced prostate cancer were included and stratified according to the National Comprehensive Cancer Network (NCCN) guidelines: ‘low risk’ for cT1a-cT2a, Gleason Score (GS) <7, Prostate Specific Antigen (PSA) <10 ng/ml; ‘intermediate risk’ for cT2b-cT2c, GS=7 and PSA between 10 and 20 ng/ml; ‘high risk’ for cT3a-cT3b-cT4, GS ≥8, PSA >20 ng/ml (14). All patients underwent histological confirmation using trans-rectal ultrasound (TRUS)-guided biopsies and pre-treatment evaluation (complete medical history, physical examination including digital rectal examination, blood test with PSA level, multi-parametric pelvic magnetic resonance imaging and 99mTc bone scan for high-risk patients). Androgen deprivation therapy (ADT) was allowed for intermediate- to high-risk patients, given neoadjuvantly, concomitantly and adjuvantly to EBRT for a total of 6 months (intermediate-risk) or 24 months (high-risk). Synchronous inflammatory bowel disease and severe comorbid conditions were considered as exclusion criteria. Written informed consent was obtained from all patients.
Set up, target volumes and definition of organs at risk. Each patient underwent a pelvic computed tomographic (CT) scan for planning purposes in the supine position with an indexed-shaped knee rest and ankle support (CIVCO Medical Solutions, Kalona, IA, USA) to prevent hip rotation. Five-millimeter axial images were acquired from the top of L5 vertebral body to the bottom of lower trochanters. An isocenter was found during virtual simulation by CT and its projection were subsequently marked on the patient's skin under laser guidance. To allow for daily reproducibility of bladder and rectal filling, all patients were instructed to drink 500 ml of water 1 h before planning CT (as for every treatment fraction) and to perform a daily enema and to follow a low-residue fiber diet starting 3 days prior to simulation. Clinical target volumes (CTVs) included the prostate gland only (from the apex to the proximal portion of seminal vesicles) for low-risk cases (CTV1); prostate gland plus seminal vesicles (CTV2) for intermediate-risk cases; and adjacent pelvic lymph nodes (bilateral common, external and internal iliac, obturator and pre-sacral) in case of high-risk features (CTV3). An 8 mm margin expansion was required from CTVs to planning target volumes (PTVs) except for prostate and seminal vesicles in the posterior direction (5 mm) and for pelvic lymph nodes, whenever an overlap with bony structures was present (5 mm), to generate corresponding PTV1, PTV2 and PTV3. Organs at-risk outlined for the optimization process were the bladder and rectum (from the anal canal to the recto-sigmoid flexure) defined as solid organs, bilateral femoral heads, penile bulb and peritoneal cavity, including both small and large bowel.
Prescription, planning and image-guided radiotherapy. All patients received 70 Gy/28 fraction (2.5 Gy daily) to the prostate gland; for intermediate- and high-risk patients, seminal vesiscles received 63 Gy/28 fractions (2.25 Gy/day); high-risk cases also underwent elective pelvic lymph node irradiation to 53.2 Gy/28 fractions (1.9 Gy/day). Multiple volumes were treated concomitantly with a different dose per fraction within the same treatment plan using a SIB approach.
The dose was prescribed at the International Commission of Radiation Units (ICRU) point. Dose distribution was optimized so that 95% of all PTVs received at least 95% of the prescription dose, minimizing hot-spot occurrence (Dmax <105% of prescribed dose). Dose constraints for organs at risk were set to V50<35%, V60<25%, V65<15%, and V68<5% (rectum), V60<35% and V40<50% (bladder), Dmean<50 Gy (penile bulb), D50<40 Gy, D10<50 Gy and D5<60 Gy (peritoneal cavity), Dmax<50 Gy (femoral heads). IMRT plans were generated using the Oncentra Masterplan treatment planning software (Elekta, Crowley, UK), employing seven coplanar fields and using 6 MV photons. Treatment was delivered with LINAC equipped with an on-board imaging device, namely an On Board Imager OBTM cone-beam CT (CBCT) (Varian Medical System, Palo Alto, CA, USA). The image-guided RT protocol comprised of daily kilovoltage CBCT during the first five fractions and a weekly CBCT thereafter. Alignment verification with planning CT was performed with both automatic bone alignment and soft-tissue matching, using the prostatic–rectal interface as a positional marker. If the mean values of displacement along each axis during the first five fractions exceeded 5 mm, the patient underwent a new simulation session with the identification of new skin markers.
Tumor control and toxicity assessment. All patients underwent a weekly clinical examination during the EBRT course. As prevention, milk enzymes were given during EBRT. Follow-up evaluation consisted of clinical examination and PSA level assessment at 3 and 6 months and every 6 months thereafter. Follow-up discontinuation was planned after 5 years. Biochemical failure (BF) was defined as a 2-ng/ml PSA level rise after nadir was reached, according to the Phoenix Criteria (13). Gastrointestinal and genitourinary acute and late toxicities were evaluated according to the Radiation Therapy Oncology Group criteria (14). Late toxicities were defined as occurring 90 days from EBRT end. Generally, as grade 1 toxicities, we scored the occurrence of new symptoms not requiring medication or an increase in the magnitude of symptoms compared to baseline. Grade 2 toxicities were defined whenever new medications (e.g. anti-diarrheal drugs) or an increase in previous medications were needed or in case of a single surgical intervention performed (i.e. single laser coagulation for bleeding). Grade 3 toxicities were defined when requiring surgery (i.e. Trans-Urethral Resection of Prostate (TURP) or permanent catheter or multiple laser coagulation for bleeding occurrence) (14). Erectile dysfunction (ED) was assessed according to the International Index of Erectile Function-5 (IIEF-5) (15). The questionnaire was filled in by patients at baseline and at every follow-up. The IIEF-5 score is defined as follows: severe ED=1-7 score, moderate ED=8-11 score, mild to moderate ED=12-16 score, mild ED=17-21 score, no ED=22-25 score. BF as defined above was considered as event for Biochemical-failure Free Survival (BFFS). Death of disease was defined as death due to disease and considered for Cancer-specific Survival (CSS). Death of any cause was considered for Overall Survival. Survival curves and actuarial rates of relapse were calculated using Kaplan-Meier method. The significance of dosimetric parameters in terms of erectile dysfunction was assessed using stepwise Cox proportional hazard regression models. A p-value <0.05 was considered significant.
Results
Patients' characterictics. Between January 2010 and October 2012, a total of 104 consecutive patients with prostate cancer were treated with image-guided IMRT under a hypofractionated schedule. The median follow-up time was 26 (range=15-48) months. The median age at diagnosis was 72 (range=53-81) years. Most patients were affected with a T1c (35%) prostate carcinoma, with GS=7 (39%) and an intermediate-risk category (39%) according to the NCCN. The median PSA level at diagnosis was 7 ng/ml. Up to 78% of patients had comorbid conditions and 6% had undergone a previous TURP. Up to 25% of patients received neoadjuvant and concomitant ADT, while 21% also had adjuvant hormonal manipulation. Most of them (14%) had hormonal monotherapy either with Luteinizing Hormone Releasing Hormone (LH-RH) analog or anti-androgen. The median duration of ADT was 25 months (Table I).
Dosimetric results. The median dose to 95% of PTV1 (D95%) was 95.97% of the prescribed dose (range=93.54-97.65%); nine patients (15.5%) had a D95% value below 95%. The median D95% for PTV2 was 96.58% (range=94.20-98.54%); two patients (3.4%) had D95%<95%. For PTV3, the median D95% was 97.3% (range=94.68-99.4%); ore patient (1.7%) had D95%<95%. The median rectal volume receiving 52 Gy (V52) was 16.36% (range=6.87-31.72%), while the median V61 was 7.56% (range=2.3-17.53%). The median V45 for bladder was 29.95% (range=10.21-69.68%); 11 patients (18.65%) had a V45>50%.
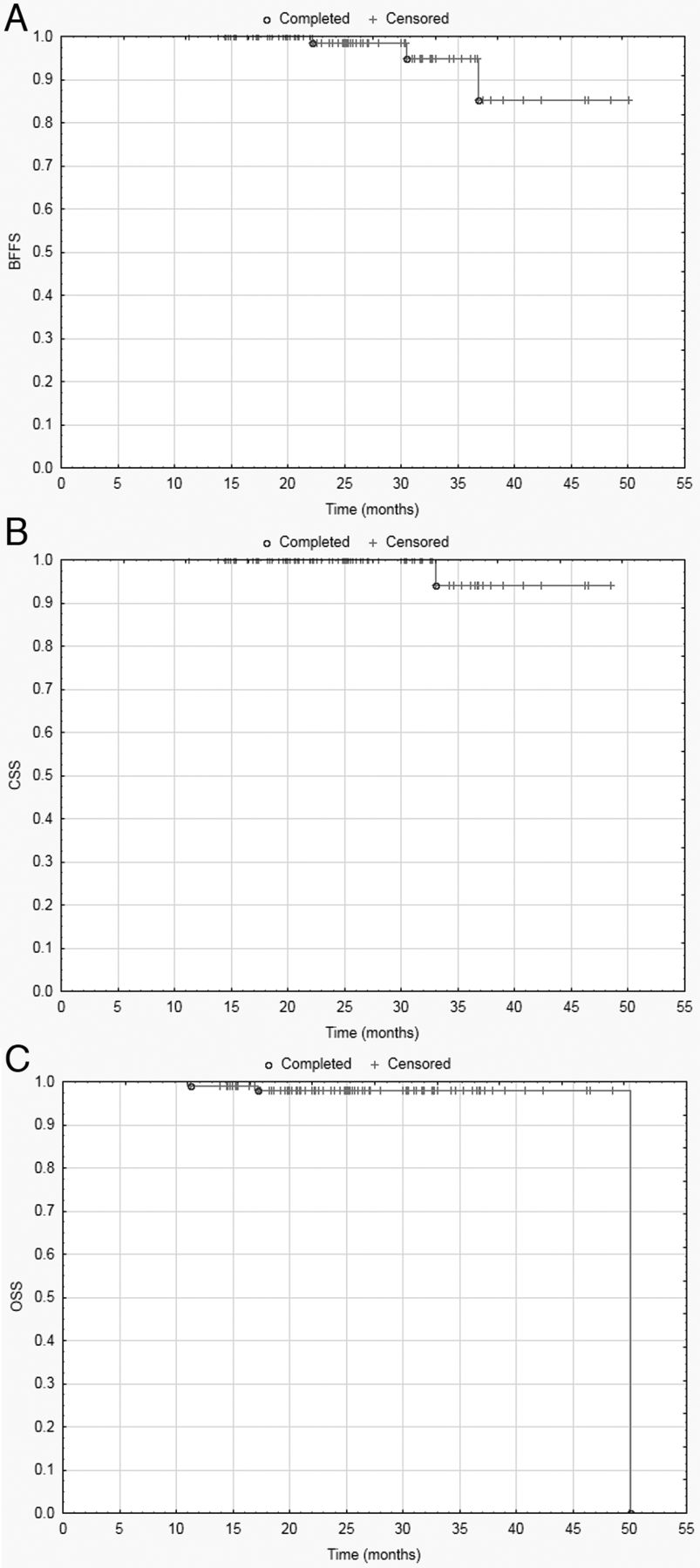
Clinical results. The median observation time was 26 months. By the time of last follow-up, 98 patients were free from disease. Two patients developed BF, while one patient also developed bone metastases. One patient died of disease, while two patients died of other causes. The 3-year biochemical failure-free survival (BFFS) was 96.5% (95% CI=89%-98%; Figure 1A), 3-year cancer-specific survival (CSS) was 98.5% (95% CI=91%-99%; Figure 1B) and 3-year overall survival (OS) was 96.5% (95% CI= 89%-98%; Figure 1C).
Acute toxicity. A total of 15 patients (14.4%) experienced acute rectal toxicity of any grade by the end of the EBRT course. Grade 1 gastrointestinal toxicity was seen in 11 patients (10%), G2 in three (3%) and G3 in one (1%). Acute genitourinary symptoms were more frequent, being developed by 33 patients (32%): 27 (26%) had G1, three (3%) had G2 and two (2%) had G3. No G4 toxicities were observed. Age, treatment volumes, neoadjuvant and concurrent ADT, previous TURP, NCCN risk category and comorbid conditions did not predict the occurrence of acute gastrointestinal and genitourinary symptoms. At 3 months, both gastrointestinal and genitourinary toxicities fell to 2.9% of grade 1.
Late toxicity. A total of 16 patients (15.3%) developed late gastrointestinal toxicity, specifically proctitis during follow-up evaluation: G1=6 patients, 5.7%; G2=8 patients, 7.6%; G3=2 patients, 1.9%; G3 events were treated with multiple laser coagulation, with no need for blood transfusion and no G4 events were recorded. At 12 months, the gastrointestinal toxicity rate of any grade was 6.8%. The median time at development of late gastrointestinal toxicity of any grade was 12 (range=4-17) months. A total of 11 patients (10.5%) had genitourinary toxicity, with a median development time of 13 (range=5-18) months, specifically G1 in six patients (5.8%) and G2 in five patients (4.8%); no G3 GU events were observed and most G2 events (80%) were due to frequency and urgency. At 12 months the genitourinary toxicity rate of any grade was 1.9%.

A. Biochemical failure-free survival. B. Cancer-specific survival. C. Overall survival.
Erectile dysfunction. For the present analysis, only patients with IIEF score ≥12 and free from ADT were taken into account. This gave a total of 45 patients to be evaluated for eventual erectile dysfunction. Patients were equally distributed into three different categories of erectile dysfunction: mild-moderate (IIEF score=12-16): 14 patients (31%), mild (score: 17-21): 15 patients (33%) and none (score=22-25): 16 patients (36%). In the subset of patients with preserved erectile function at baseline, only 25% showed no change over baseline, while 75% of them had worsening in erectile dysfunction class (mild: 25%; mild-moderate: 25%; moderate: 25%). In the subset of patients with mild erectile dysfunction at baseline, up to 83% remained within the same class, while 17% had a decrease of erectile function with a score <7 (severe erectile dysfunction). Among patients with mild to moderate baseline IIEF score (12-16), 66% had no change, while 33% had a class modification to severe erectile dysfunction (score <7). A mean RT dose >50 Gy to the penile bulb had a statistically significant correlation with a worsening by at least one category in IIEF score (OR=1.14; 95% CI=1-1.3; p<0.05).
Discussion
Hypofractionated EBRT is an attractive therapeutic option in the radical setting of prostate cancer (16, 17). From a radiobiological point of view, the low α/β ratio for prostate cancer cells and the fact that this value seems to be lower than those for surrounding normal tissues represents a unique opportunity to perform a ‘radiobiological’ dose escalation without harming neighboring organs at risk, thus achieving a widening of the therapeutic index. As in other oncological settings, potential advantages of hypofractionation are tailored towards patients (increase in convenience and reduction of costs), radiation oncology departments (increase in patient turnover) and healthcare providers (reduction of costs) (18). Recent technological advances have provided reliable RT platforms and precise delivery systems to safely administer hypofractionated schedules to patients with prostate cancer (7, 10). Interestingly, Zaorsky et al., in a recent review, defined a ‘technologically advanced radiotherapy modality’ as one with a more favorable benefit-to-risk ratio than standard RT approaches, where the advantage derives from the use of up-graded IGRT, IMRT or integration of both (19).
The fractionation we employed was taken from the Cleveland Clinic experience, where 770 consecutive patients were treated between 1998 and 2005 using IMRT. Using the PSA nadir plus 2 ng/ml definition of biochemical failure, the 5-year BFFS was 94%, 83% and 72%, respectively for low-, intermediate- and high-risk disease, after a median observation time of 45 months (20). The acute toxicity profile was acceptable, with a maximum 9% rate of G2 rectal and 1% of G3 genitourinary toxicities. Late events were rare with 1.4% of G3 or more for rectal and 0.1% for genitourinary toxicity. Our results are similar, even if they refer to a shorter follow-up time. Our BFFS was 96.5% (95% CI=89%-98%) and the toxicity profile was mild, with G3 acute events down to 1% for genitourinary and 2% for gastrointestinal and late rectal bleeding rate of 1.9%.
Patients' characteristics.
Radiation-induced erectile dysfunction remains a controversial and poorly-understood issue in RT for prostate cancer, even if hemodynamic alterations of the erectile tissue are a quite common observation after radiation (21). Several structures have been advocated as regions sensitive in the development of erectile dysfunction: the crura of the corpora cavernosum, neurovascular bundles and internal pudendal arteries (22). The penile bulb has been found to be a potential predictor of erectile dysfunction, even if it may not be a component critical to erectile function (22). Data concerning the role of hypofractionated schedules on post-radiation erectile dysfunction are generally lacking. McDonald et al. recorded a 3-point decrease in the median Sexual Health Inventory for Men score after hypofractionated RT, with a concomitant doubling of the rate of phosphodiesterase-5 inhibitor use. These results are similar to those reported using conventional fractionation. In two studies investigating the effect of dose-escalated RT in fully potent men, the potency preservation rates were between 60% and 64% (23, 24). Our results are in line with the aforementioned findings for patients having a mild or mild-to-moderate baseline erection deficit, while for patients with ‘ab initio’ normal function, the observed reduction in our series is higher. This may be due to the small sample size evaluated for erectile function, which may have led to a selection bias. Another explanation is that in our fully potent subset of patients, the median IIEF score was 22.5, meaning that even a small reduction in erectile function may have led to a modification in the score group allocation.
In conclusion, hypofrationated radiotherapy delivered with IMRT and image-guided RT was safe and effective in the treatment of prostate cancer, with consistent biochemical control and a mild toxicity profile. However, erectile function does seem to be affected by this hypofractionated schedule.
Footnotes
Conflicts of Interest
The Authors declare that they do not have any conflict of interest.
Financial Support
None to declare.
- Received April 3, 2015.
- Revision received April 29, 2015.
- Accepted May 4, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}