


Abstract
Aim: To evaluate the efficacy of prophylactic radiotherapy at intervention sites in patients with malignant pleural mesothelioma (MPM). Patients and Methods: From 05/2010 to 12/2014, 53 patients with histologically confirmed MPM were treated in order to prevent interventional site metastases. Irradiation was carried out with 3×7=21 Gy with 6-18 MeV electrons. Results: The mean follow-up period was 14.4 months (range=0-37 months). At the time of the analysis, 20 patients were alive. Three patients had developed a local recurrence within the irradiated site, representing a local recurrence rate of 5.7%. Toxicity was low, with transient grade I erythema found in 20.7% of patients. No grade II or higher toxicity was observed. Conclusion: Our simple and time-saving RT approach to interventional sites in patients with MPM was both effective and well-tolerated. This approach is easily integrated into general treatment concepts. Until publication of results from prospective randomized trials, prophylactic RT to intervention sites should remain standard.
- Malignant mesothelioma
- prophylactic radiotherapy
- intervention-site metastases
- procedure-tract metastases
Malignant pleural mesothelioma (MPM) is a rare tumor arising from the mesothelial cells of the pleura, with a high correlation with exposure to asbestos (1). Chest wall seeding following invasive procedures such as thoracoscopy, pleural aspiration and biopsy, has been described to occur in around 20%, but may be as high as 50% (2-4).
In 1995, prophylactic RT to the drainage site after thoracoscopy was found by Low et al. to prevent seeding (5). Several retrospective trials have confirmed those results (6-11). However, three prospective trials with a limited number of patients and heterogeneous radiotherapy (RT) schedules provided divergent results (2, 12-13). Therefore, prophylactic RT to the drainage sites is not recommended in international guidelines (14-16), although often used in routine practice (17, 18).
Due to the lack of high-quality prospective randomized data, we performed this study to evaluate efficiency and safety of treatment with a convenient and time-efficient hypofractionated prophylactic RT approach following endoscopy in patients with MPM. In addition, we reviewed published data focusing on different RT schedules and techniques.
Patients and Materials
Between 05/2010 and 12/2014, 53 consecutive patients with histologically confirmed MPM were treated with prophylactic RT to the drainage site (video-assisted thoracoscopy) with the following schedule: 7 Gy on three consecutive days (total 21 Gy) with electrons. This RT approach is both very convenient for the patient and time efficient.
The energy of electrons was determined using computed tomography (CT) by measuring the distance (depth) between the skin surface and pleura (energies: Table I). The scar was highlighted with a radiopaque marker before measurement. Field size was estimated clinically, taking the size of the drainage site into account by adding a margin of 1-2 cm in all directions. In cases of initially existing drainage seeding, another RT schedule was used (10×3=30 Gy, 15×2.5=37.5 Gy, or 20×2=40 Gy) (data not shown). In the first two patients in 2010, photons were used; additionally photons were used in two patients with simultaneous treatment of bone metastases.
Further treatment after prophylactic RT to the drainage sites and regular follow-up visits were carried out-at the Department of Pneumology, Siloah Hospital, Hannover.
First-line chemotherapy consisting of cisplatin or carboplatin and pemetrexed was applied in 47 patients. Three patients refused further systemic treatment and in three patients best supportive care was provided due to reduced general condition.
Acute toxicity and late toxicity were assessed according to Common Terminology Criteria for Adverse Events (CTCAE) version 4.0 (19).
Patient- and treatment-related parameters.
Patient- and treatment-related parameters are summarized in Table I.
A literature review was carried out searching Medline using the following terms: mesothelioma, prophylactic radiotherapy, tract metastases, seeding, intervention-site metastases, procedure-tract metastases, port-site prophylaxis, and drain site radiotherapy. All original articles providing new data on prophylactic procedure site RT in patients with MPM were included (Table II).
Results
Outcome. The median follow-up was 14.4 (range=0-37) months. One patient died immediately after completion of RT. At the time of analysis, 20 patients were still alive, and 33 patients had died of progressive disease. Out of 53 patients (81 locations) being treated with 3×7=21 Gy, three patients developed a local recurrence within the irradiated area after 12, 16, and 27 months, respectively (Figure 1). Out of those, two patients were re-irradiated with either 3×7=21 Gy or 15×2.5=37.5 Gy. In both cases, the patients described a sufficient pain relief after repeat RT. The third patient was not symptomatic and died 1 month after detection of local failure due to systemic progression.
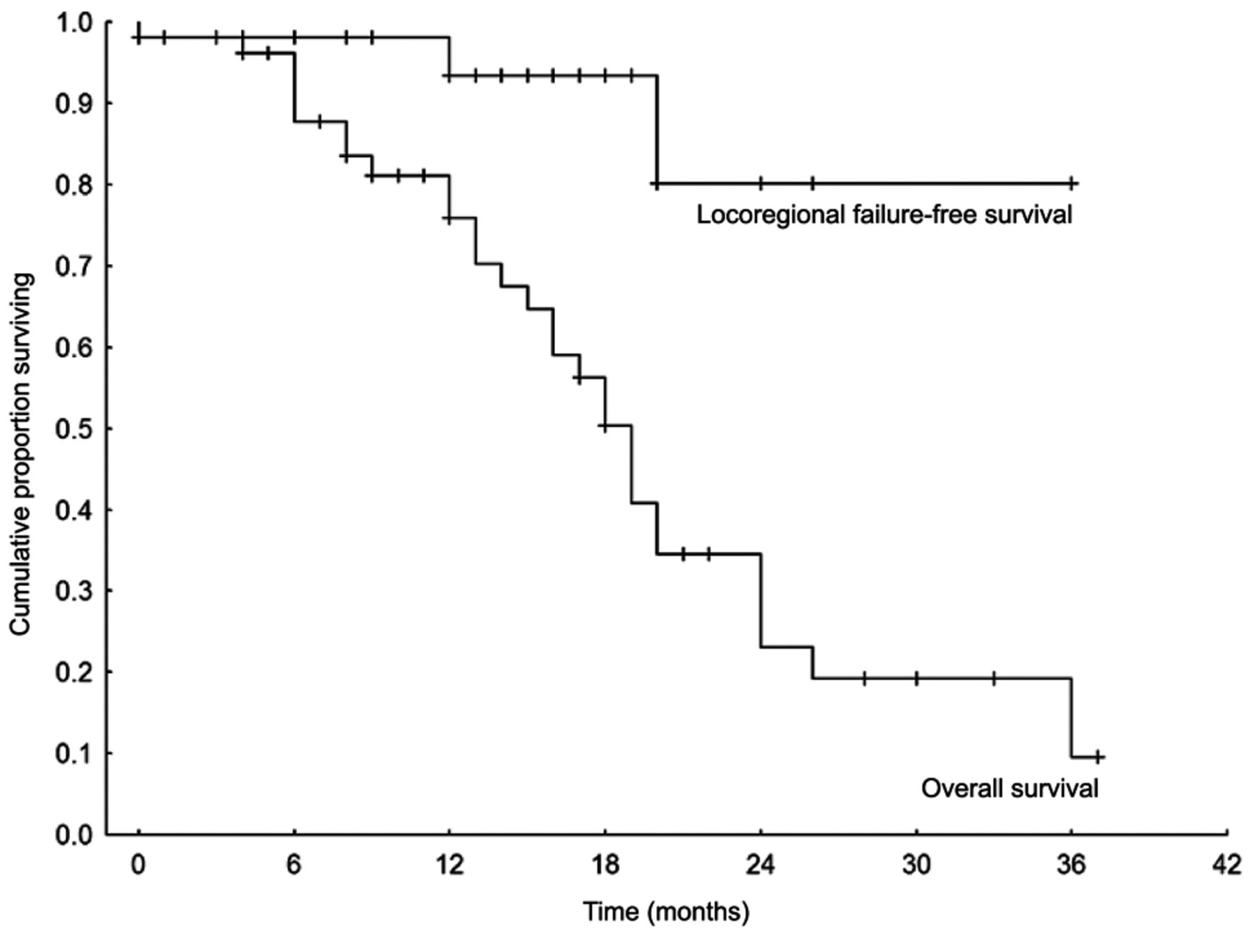
Locoregional failure-free survival and overall survival.
The local recurrence rate was 5.7% considering the number of patients (n=53) and 3.7% considering all treated sites (n=81).
Acute toxicity. Treatment was well-tolerated, with no grade 2 or higher side-effects. Grade I radiation-induced erythema was described in 20.7%, and one patient suffered from slight transient fatigue syndrome (1.9%).
Time interval from intervention to RT. The median time interval from last procedure to start of RT was 15.5 days, with a range from 4 to 40 days. The patients with local recurrence started RT 4, 20, and 22 days after procedure, respectively.
Discussion
MPM quite often recurs along the tracks of chest wall instrumentation. Post-intervention RT to drainage sites has the potential to reduce the rate of tract metastases, which has been shown in several retrospective studies (5-11). However, three prospective studies showed conflicting results. The studies of O'Rourke et al. (12) and Bydder et al. (13) failed to demonstrate any significant benefit from prophylactic RT to the drainage sites. In contrast, Boutin et al. recommended the use of prophylactic RT, since none of their 20 irradiated patients developed a local recurrence, while 40% of the patients without RT experienced local failure (2). The results of all of these studies may have been confounded by the relatively small numbers of patients, ranging from 20 to 31, in the RT arms. Furthermore, the RT schedules and RT techniques were quite heterogeneous. While two studies treated patients with 3×7 Gy (2, 12), Bydder et al. only used 1×10 Gy, which would likely be an insufficient radiation dose for a less radiosensitive tumor such as MPM (13). Additionally, the electron energy of 9 MeV, which was used as a ‘one size fits all’ energy, might not be appropriate for some patients. If 9 MeV is used, the maximum depth receiving a sufficient dose is limited to only about 3 cm. In our analysis, we used a homogenous schedule of 3×7 Gy, with individualized electron energy accounting for the unique anatomy of every patient. Excluding the study of Bydder et al. due to these methodological flaws and limitations, only one prospective study, with a limited number of patients, stands against another prospective study and several retrospective studies (Table II) all demonstrating a benefit from prophylactic RT.
Studies reporting on outcome of prophylactic radiotherapy (RT) to intervention sites in patients with mesothelioma.
Our local recurrence rate of 5.7% (considering patients) or 3.7% (considering all treatment sites) compares favorably with most of the heterogeneous literature results of 0-21% for irradiated patients. Remarkably, out of our three patients developing a recurrence within the radiation field, two were treated successfully with a second series of RT (pain relief and local control until death).
In the study from the literature with the highest recurrence rate of 21%, the authors considered the long delay between intervention and RT as one possible explanation for the unsatisfactory outcome. In contrast to their series with a mean delay of 37 days, our mean time from intervention to RT was only 15.5 days. West et al. also highlighted the need for prompt RT referral and early treatment following chest instrumentation, as 8% of their patients had already developed tumor invasion by the time RT was started (7).
In patients with MPM, median survival is limited and treatment is mostly palliative in nature (11). Taking into account the poor survival prognosis of many patients with MPM, it becomes obvious that the application of prophylactic RT has to be simple, time-efficient and convenient for the patients in order not to compromise systemic treatment or quality of life, as well as to minimize the time the patients need to spend receiving treatment. With our schedule, only three sessions of irradiation were necessary. The absence of grade II toxicities demonstrates that our approach was very well tolerated. Moreover, this approach proved to be feasible even when concurrent systemic treatment was given and when re-treatments to other thoracic sites were required. The percentage of patients receiving chemotherapy was much greater than in other studies (88.7% versus 19-63%), when reported (8-11).
Although the results of the present study are very encouraging, its retrospective design and the limited number of patients need to be taken into account when interpreting the results. However, this is the largest cohort of patients receiving prophylactic RT after intervention for MPM reported in the literature so far. Since MPM is a rare disease, prospective trials with adequate numbers of patients and adequate statistical power cannot be expected in the near future.
Conclusion
This study suggests our simple and convenient approach for prophylactic RT to drainage sites in patients with MPM to be both effective and safe. This is the largest patient cohort reported in the literature being treated with a homogenous RT approach. We recommend this approach of prophylactic RT to drainage sites for patients with MPM, not least for patients with a poor survival prognosis.
- Received April 9, 2015.
- Revision received April 30, 2015.
- Accepted May 4, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.