


Abstract
Background/Aim: Regorafenib has been approved for treatment of patients with unresectable or recurrent gastrointestinal stromal tumors resistant to imatinib or sunitinib. However, regorafenib has severe side-effects, including acute liver failure. We describe the case of a patient with multiple liver metastases of a small intestinal stromal tumor who experienced acute liver failure while being treated with regorafenib. Case Report: A 50-year-old patient with an unresectable small intestinal stromal tumor resistant to prior treatment with imatinib and sunitinib was started on regorafenib, but experienced acute liver failure 10 days later. Plasma exchange and steroid pulse treatment improved her liver function. During liver failure, abdominal ultrasonography showed to-and-fro flow in the portal vein. Lactate dehydrogenase concentration was markedly elevated to 1633 U/l. These findings indicate that liver failure in this patient was due to impaired liver blood flow. Conclusion: Regorafenib may impair liver blood flow, inducing acute liver failure.
Gastrointestinal stromal tumors (GISTs) are among mesenchymal tumors that occur in the gastrointestinal tract. GISTs arise from the interstitial cells of Cajal, which are present in the neuroplexus of the digestive tract wall (1, 2). The treatment- of- choice for primary GIST is surgery, with chemotherapy prescribed for patients with recurrent or unresectable GIST. The treatment for unresectable and recurrent GISTs was revolutionized by the introduction of inhibitors of KIT and platelet-derived growth factor receptor-α (PDGFRA) kinase, such as imatinib (3, 4) and sunitinib (5). Unfortunately however, most tumors develop resistance to these agents.
Regorafenib, an oral inhibitor of several protein kinases involved in tumor growth and angiogenesis, was recently approved to treat patients with unresectable and recurrent GISTs resistant to imatinib or sunitinib. Regorafenib was found to significantly enhance progression-free survival compared to placebo in patients with metastatic GIST after progression on imatinib and sunitinib (6). However, the incidence of adverse events was high, with side-effects observed in 93% of patients. The most common side-effects of regorafenib included hand-foot syndrome (45.0%), diarrhoea (33.8 %), decreased appetite (30.4%), fatigue (29.0%), dysphonia (28.4%), hypertension (27.8%), and rash (22.6%). The most severe side-effect was liver failure, with two Japanese patients dying of severe liver failure. Acute liver failure induced by regorafenib is of hepatocellular type (6-8), but its precise mechanism is not known.
This report describes a patient with GIST of the small intestine who experienced severe liver failure due to regorafenib. Ultrasonography showed to-and-fro flow in the bloodstream, and blood tests showed elevated lactate dehydrogenase (LDH) concentrations, indicating that impaired liver blood flow resulted in severe liver failure. To our knowledge, this is the first report to show that liver failure due to regorafenib resulted from impaired liver blood flow.
Case Report
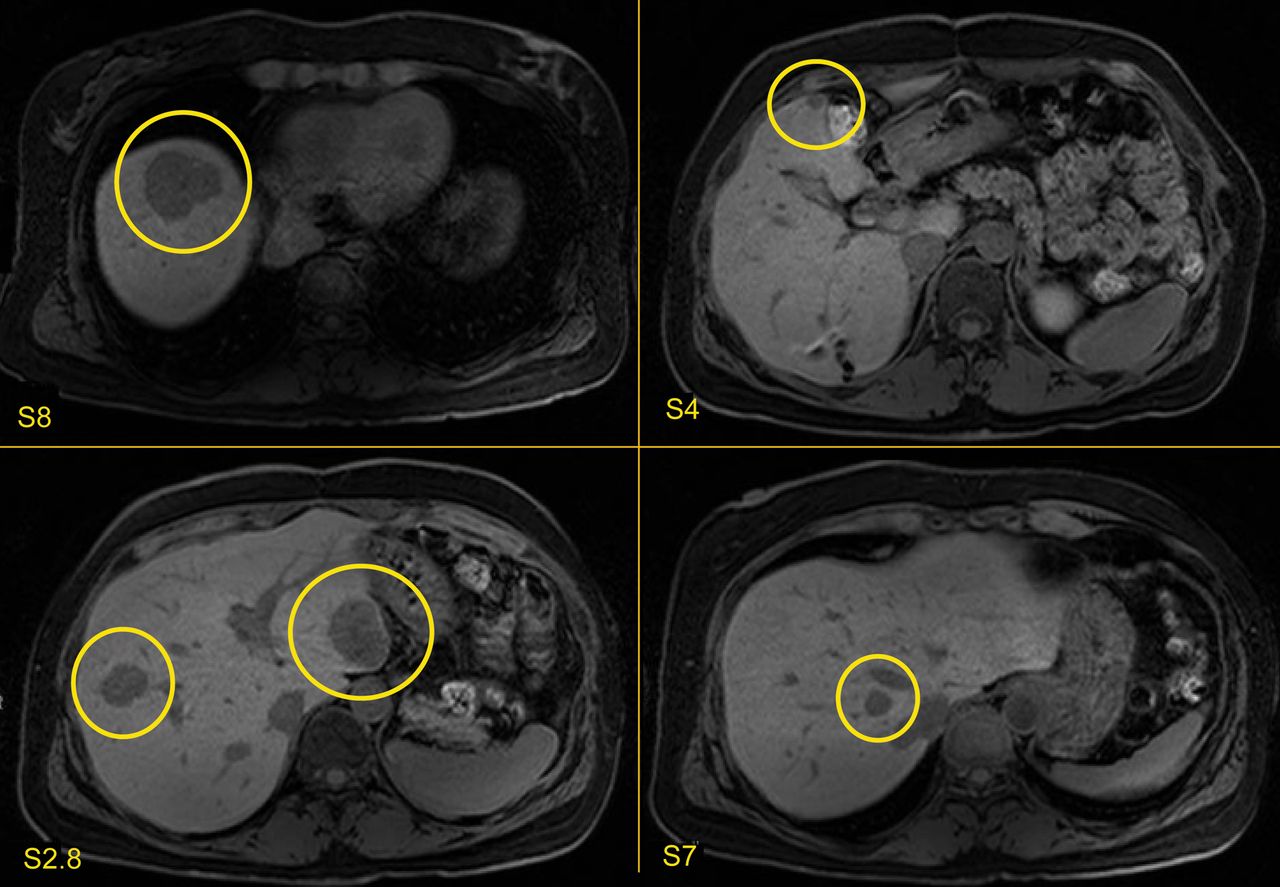
A 50-year-old woman with a good performance status was admitted to our Department in 2007 with a stomach tumor. She was diagnosed with a tumor of the small intestine and underwent partial resection of the intestine. The tumor was pathologically diagnosed as GIST. Two years later, GIST recurrence was found in S6 of the liver, and she underwent partial resection of the liver. In 2011, many new liver metastases were observed. As these tumors were unresectable, the patient was treated with imatinib and sunitinib. She achieved a partial response and underwent partial liver resection for these metastases. An examination in February 2014 showed multiple liver metastases (Figure 1). As these tumors could not be resected, the patient was started on chemotherapy with regorafenib (160 mg/day). Ten days after starting regorafenib, the patient visited our Outpatient Clinic with a high fever of 40°C and general fatigue. Blood tests showed elevated hepatic enzymes, including aspartate aminotransferase (AST) and alanine aminotransferase (ALT) concentrations of 145 U/l and 103 U/l, respectively, and a low platelet count of 54000/μl (Figure 2). She was immediately hospitalized and started on liver support therapy with ursodeoxycholic acid, while regorafenib was stopped.

Multiple liver metastases before regorafenib treatment. Magnetic resonance imaging shows multiple liver metastases in S2, S4, S7 and S8.
However, her liver function seriously worsened four days after admission, 15 days after starting regorafenib (Figure 2). She was moved to the Intensive Care Unit, where she was treated with plasma exchange and steroid pulse therapy (1 g/day) for three days. At that time, abdominal ultrasonography showed to-and-fro flow in the portal vein (Figure 3), an indicator of impaired hepatic blood flow, and her lactate dehydrogenase (LDH) concentration was markedly elevated, at 1633 U/l (Figure 2). These results indicated that regorafenib-induced acute liver failure in this patient was due to impaired liver blood flow.
Her liver function improved three days after plasma exchange (Figure 2). The patient was moved back to the ward 10 days after emergency treatment, 20 days after starting regorafenib. She now attends an Outpatient Clinic undergoing strict follow-up.
Discussion
This report describes a patient with multiple liver metastases of a GIST of the small intestine who experienced acute liver failure due to regorafenib administration.
Regorafenib inhibits several tyrosine kinases, including VEGFR, TIE2, c-KIT, rearrangement during transfection (RET), v-raf murine sarcoma viral oncogene homolog B1 (BRAF), PDGFR and fibroblast growth factor receptor (FGFR). VEGFR and TIE2 are associated with angiogenesis; c-KIT, RET and BRAF with tumor progression; and PDGFR and FGFR are growth factor receptors. Regorafenib is used to treat patients with recurrent or unresectable colorectal cancer, and GIST. The CORRECT study showed that regorafenib has survival benefits in patients with metastatic colorectal cancer whose disease progressed after all standard therapies (7). In addition, the GRID trial showed that regorafenib can significantly improve progression-free survival compared to placebo in patients with metastatic GIST after progression on standard treatments (6).
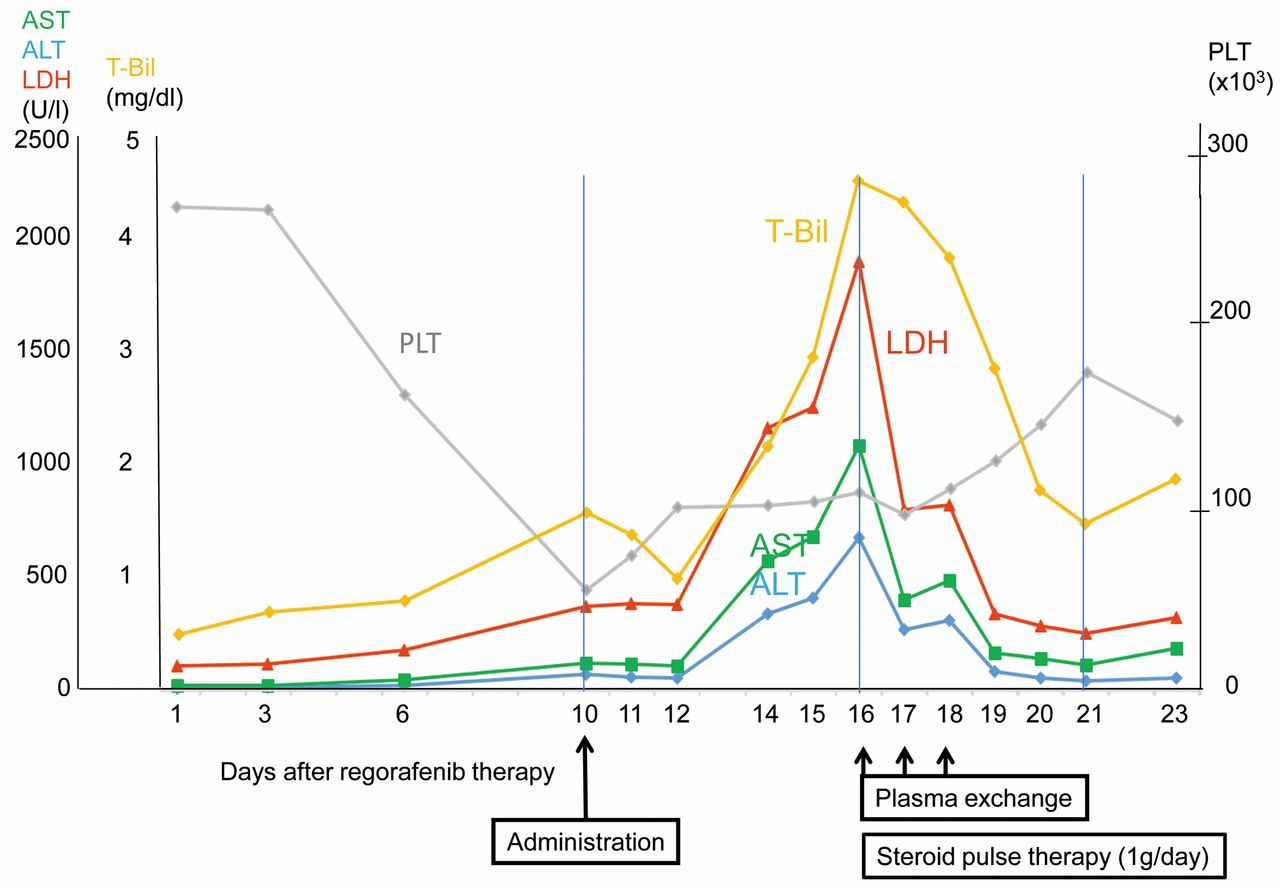
Effects of treatment on concentrations of the liver enzymes aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin (T-bil) and lactate dehydrogenase (LDH), and on platelet counts. LDH was significantly elevated 16 days after starting regorafenib treatment.
Despite its activity in patients with colorectal cancer and GIST, regorafenib has many side-effects, the most severe being liver failure. An analysis of Japanese and non-Japanese sub-populations in the CORRECT study found that indicators of liver failure, including elevated ALT (and AST) concentrations, were frequently observed in Japanese patients (9). Moreover, one Japanese patient experienced lethal liver dysfunction related to regorafenib.
Drug-induced liver failure can be classified into three groups: hepatocellular, cholestatic, and mixed type. Regorafenib induces hepatocellular-type failure. Findings in our patient, including the highly elevated LDH level and to-and-fro flow in the portal vein, indicate that regorafenib may have impaired liver blood flow, resulting in severe liver dysfunction.
LDH, an enzyme found in almost all tissues in the body, plays an important role in cellular respiration. Although LDH is abundant in tissue cells, its levels in blood are normally low. However, tissues damaged by injury or disease release LDH into the bloodstream. Conditions that increase LDH in the blood include liver disease, heart attack, anaemia, muscle trauma, bone fractures, cancer, and infections such as meningitis, encephalitis and HIV. The combination of a two- to five-fold elevation in LDH with elevations in enzymes related to liver function indicates both necrotic and obstructive liver disease (10). The to-and-fro flow observed by ultrasonography is indicative of impaired blood flow in the liver. Chemotherapy, including treatment with actinomycin, azathioprine, dacarbazine, 6-thioguanine, 6-mercaptopurine, and cyclophosphamide has been shown to impair liver blood flow and induce veno-occlusive disease (11, 12). Our findings suggested that regorafenib may also cause veno-occlusive disease.

Ultrasonography of the portal vein, showing the to-and-fro flow pattern indicative of impaired blood flow in the liver.
In conclusion, we described a patient with GIST of the small intestine who experienced acute liver failure after regorafenib treatment. Regorafenib may impair liver blood flow, resulting in severe liver failure.
- Received March 28, 2015.
- Revision received April 30, 2015.
- Accepted May 4, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}