


Abstract
Aim: Non-small cell lung cancer (NSCLC) with minor mutations in the epidermal growth factor receptor (EGFR) gene, except for the common 15 base-pair deletions in exon 19 and the L858R mutation in exon 21, is rare, and only few data exist on this patient population. The aim of the present study was to describe the clinical characteristics and to clarify the efficacy of EGFR-tyrosine kinase inhibitors (TKIs) in patients with NSCLC harboring minor mutations of the EGFR gene. Patients and Methods: This was a multicenter, retrospective study that analyzed specimens from patients with NSCLC who had minor EGFR gene mutations and were treated with EGFR-TKIs between June 2002 and March 2012. Results: Out of 56 patients with minor mutations of the EGFR gene, 44 were treated with either gefitinib or erlotinib. Mutation sites were G719X in exon 18 (n=35), L861Q in exon 21 (n=11), and G874S in exon 21 (n=1). Three patients had both the G719S and the L861Q mutation. The response rate to TKI treatment was 29.5%, and the disease control rate was 63.6%. The median progression-free survival (PFS) was 6.7 months [95% confidence interval (CI)=2.06-8.66 months]. The median PFS was 7.2 months (95% CI=4.23-12.3 months) in 32 patients who received first- or second-line treatment with EGFR-TKIs, whereas the median PFS was 1.57 months (95% CI=0.73-3.8 months) in 12 patients treated with EGFR-TKIs as a third-line or later treatment. In multivariate Cox analysis, erlotinib therapy was associated with a longer PFS than gefitinib (p=0.025). Conclusion: Patients with NSCLC harboring minor mutations of the EGFR gene exhibited a modest response to EGFR-TKI treatment. Treatment with first-generation EGFR-TKIs, in particular erlotinib, may be considered a first- or second-line option for patients with NSCLC with minor EGFR mutations.
The prevalence of epidermal growth factor receptor (EGFR) gene mutations in patients with non-small cell lung cancer (NSCLC) is estimated to be 10% to 15% in Caucasian patients, and 30% in East-Asian patients. Characteristics of patients with NSCLC harboring EGFR gene mutations include female gender, never smokers, and adenocarcinoma by histology (1). Recently, several studies have demonstrated that patients with NSCLC with EGFR gene mutation, including the point mutation L858R in exon 21 or the 15 base-pair deletions (del746_A750) in exon 19, were highly responsive to the EGFR-tyrosine kinase inhibitors (TKIs) gefitinib or erlotinib (1-3) leading to an improvement in progression-free survival (PFS) in those treated with either as a first-line option (4-7).
Patients' characteristics (n=44).
The efficacy of EGFR-TKI treatment for NSCLC harboring major mutations in the EGFR gene, for example, L858R in exon 21 and deletions in exon 19, has been confirmed. In addition, the T790M mutation and insertions (or in-frame duplications) in exon 20, which induce resistance to EGFR-TKIs, have also been frequently documented (8-13).
In addition to the two major EGFR mutations, L858R in exon 21 and deletions in exon 19, many types of EGFR gene mutations are known to occur in exons 18 to 21, the location of the adenosine triphosphate (ATP)-binding pocket of the kinase domain; however, these mutations occur with a relatively low frequency. The clinical significance of minor EGFR gene mutations and the efficacy of treatment with EGFR-TKIs of patients with such mutations is still not fully understood. Therefore, this retrospective study evaluated patients with NSCLC who harbored minor mutations of the EGFR gene and were treated with EGFR-TKIs over a period of approximately 10 years at Japanese cancer research Institutes.
Patients and Methods
Patients. Patients with minor mutations of the EGFR gene who received either gefitinib or erlotinib between July 2002 and March 2012 at institutions participating in the Hanshin Cancer Research Group were included. The cut-off date for data collection was November 30, 2012. Patients' medical records were retrospectively reviewed, and the following information was retrieved: age, gender, lung cancer histology, performance status, smoking status, EGFR gene mutation status, and clinical response to therapy. Histological classification of lung cancer was defined on the basis of the World Health Organization pathology classification (14). Clinical staging was defined according to the seventh edition of the tumor node metastasis classification system for NSCLC (15). This study was approved by each of the Institutional Review Boards. The requirement for informed consent was waived because the clinical data were retrospective and anonymous.
Treatment and clinical assessments. Patients were administered oral, once-daily doses of either 250 mg of gefitinib or 150 mg of erlotinib until tumor progression, death, significant uncontrolled toxicity, or the patient's refusal. Treatment choice was at the physician's discretion. Baseline assessments were performed approximately 2 weeks before treatment initiation. Routine chest radiography was conducted every month to evaluate treatment responses. Chest computed tomographic (CT) scans were performed every 8 to 12 weeks as a routine procedure and were also used to confirm disease response or progression. Treatment effect was evaluated with RECIST 1.1 (16). PFS with EGFR-TKIs was assessed from the initiation of EGFR-TKI treatment to the day on which the first objective signs of disease progression or death were recorded.
Analysis of EGFR mutations. The majority of cytological or histological specimens were examined for EGFR mutations with the peptide nucleic acid-locked nucleic acid (PNA-LNA) polymerase chain reaction (PCR) clamp method (17). Mutations associated with sensitivity to EGFR-TKIs, including G719C, G719S, G719A, L858R, L861Q, and deletions in exon 19, were investigated, as well as T790M, a mutation associated with resistance to EGFR-TKIs. EGFR mutations were analyzed from exon 18 to exon 21 by direct sequencing methods for only five patients.
Objective tumor responses and progression-free survival
Results of univariate and multivariate Cox analyses for progression-free survival (n=41)
Statistical analysis. To compare groups, the Kruskal-Wallis test was used for continuous data, and either Pearson's χ2 test or Fisher's exact test was used for categorical data. PFS after initiation of treatment with either gefitinib or erlotinib was estimated with the Kaplan–Meier method to assess the time to disease progression or death. A log-rank test was used to compare cumulative survival of different groups. Prognostic factors were analyzed using univariate and multivariate Cox proportional hazards regression models with stepwise methods. All analyses were performed with JMP software, version 10 (SAS institute Inc., Cary, NC, USA). A p-value of less than 0.05 was considered to denote a statistically significant difference.
Results
Specimens from 3,306 patients with NSCLC were examined for gene mutations in the EGFR tyrosine kinase domain. Minor mutations in the EGFR gene were identified in 44 patients treated with either gefitinib or erlotinib. The medical records of these patients were reviewed in detail. Patient characteristics are shown in Table I. Among the 44 patients, 35 had been treated with gefitinib, and the other nine with erlotinib. The population comprised of 22 males and 22 females, with the median age being 66 years (range=46-82 years). Histology indicated that 40 patients had adenocarcinoma, and four patients had squamous cell carcinoma. A history of smoking was recorded for 26 patients, while 18 had never smoked. The majority of patients (n=36) had good Eastern Cooperative Oncology Group (ECOG) performance status (0 or 1). Six patients had stage IIIB disease and 38 patients had stage IV disease. EGFR-TKIs were administered as a first-line treatment for 13 patients, second-line for 19, and as third-line or later for 12. Mutation sites were G719S in exon 18 (n=20), G719A in exon 18 (n=9), G719C in exon (n=3), L861Q in exon 21 (n=11), and G874S in exon 21 (n=1). Three patients had both the G719S and the L861Q mutation. There were no substantial differences between the characteristics of patients treated with gefitinib versus erlotinib, except for treatment line.
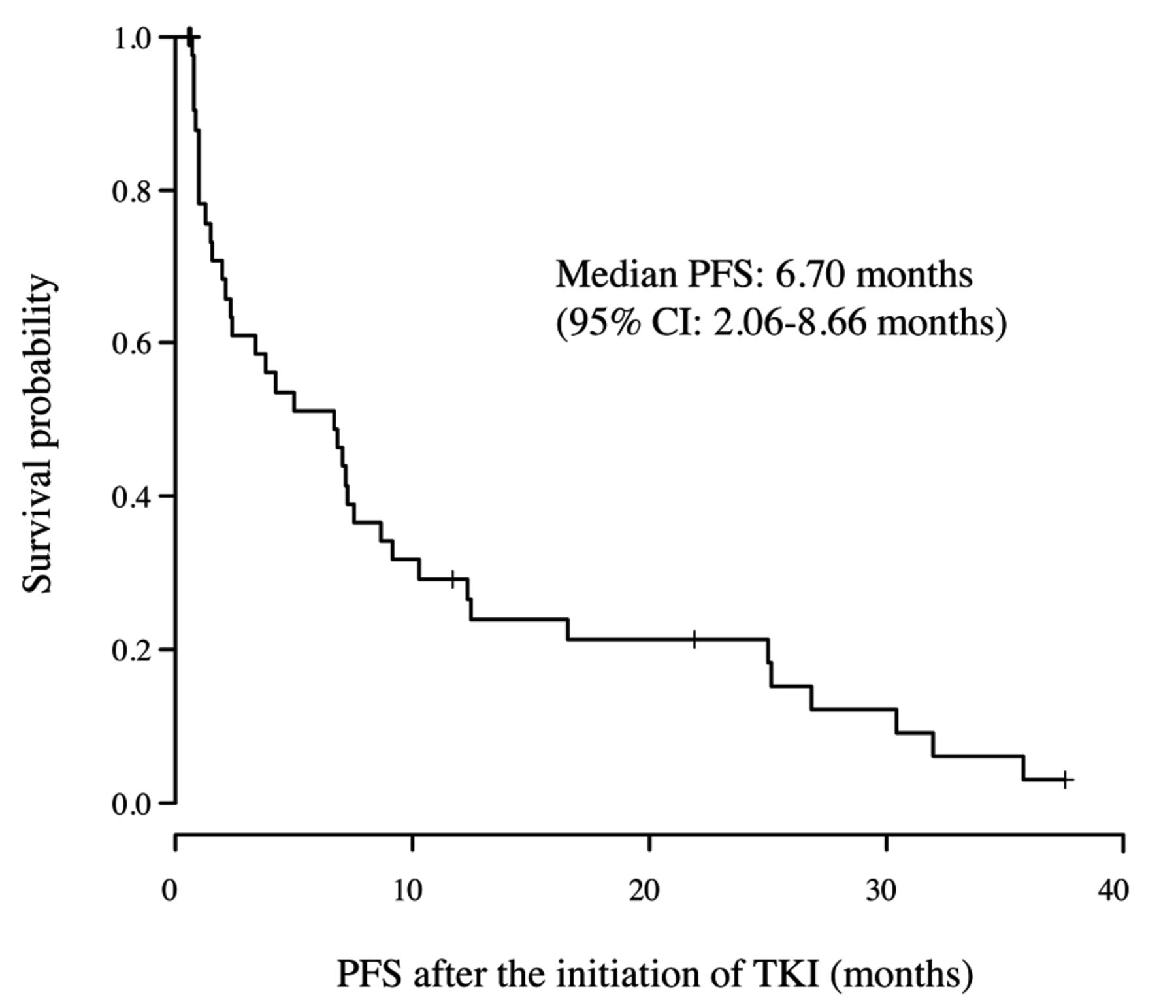
Progression-free survival (PFS) curve after the initiation of tyrosine kinase inhibitor (TKI) treatment.
Among the 44 patients treated with EGFR-TKIs, 13 had a partial response (PR), 15 had stable disease (SD), and 11 had progressive disease (PD). Data from five patients were non-evaluable. The response rate (RR=CR+PR) was 29.5% (13 of 44 patients), and the disease control rate (DCR=CR+PR+SD) was 63.6% (28 out of 44 patients). In patients with the G719X mutation, the RR was 25.0% (8 out of 32 patients), and the DCR was 59.3% (19 out of 32 patients). In patients with the L861Q mutation, the RR was 37.5% (3 out of 8 patients), and the DCR was 87.5% (7 out of 8 patients; Table II). Among the 35 patients treated with gefitinib, the RR was 28.6% (10 out of 35 patients), and the DCR was 62.9% (22 out of 35 patients). For the nine patients treated with erlotinib, the RR was 33.3% (3 out of 9 patients), and the DCR was 66.7% (6 out of 9 patients) (Table I).
Survival times from the initiation EGFR-TKI treatment are shown in Figures 1 and 2. The median PFS for all 44 patients was 6.70 months [95% confidence interval (CI)=2.06-8.66 months], with a longer median PFS for those treated with erlotinib than gefitinib (7.50 versus 5.83 months; log-rank p=0.32) (Figure 2). The PFS was 7.2 months (95% CI=4.23-12.3 months) in 32 patients with NSCLC who received first- or second-line treatment with EGFR-TKIs, whereas it was 1.57 months (95% CI=0.73-3.8 months) in 12 treated with EGFR-TKIs as third-line or later treatment (log-rank p=0.14) (Figure 3).
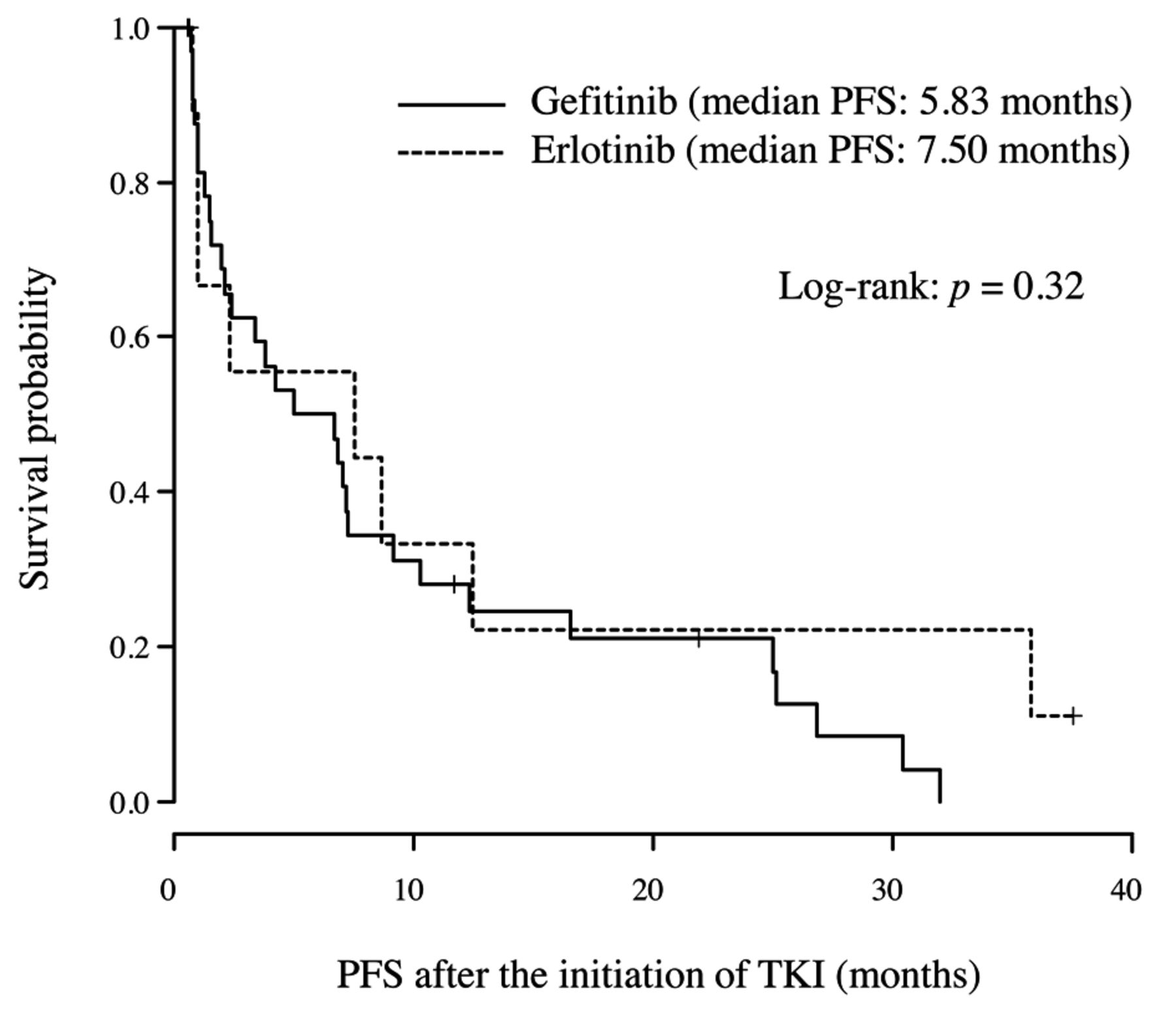
Progression-free survival (PFS) curves after the initiation of tyrosine kinase inhibitor (TKI) treatment with either gefitinib or erlotinib.
Univariate analysis revealed no correlation between PFS and patient characteristics, including treatment regimen (gefitinib or erlotinib), age, gender, histology (adenocarcinoma or squamous cell carcinoma), EGFR mutation status (exon 18 or exon 21), treatment line (first plus second or third plus later), ECOG performance status (0-1 or 2-3), and smoking history (yes/no; Table III). On the contrary, multivariate analysis revealed that erlotinib treatment was associated with a longer PFS than gefitinib treatment (p=0.025) (Table III). Other co-variables, including gender, EGFR mutation status (exon 18 or exon 21), treatment line (first plus second or third plus later), and smoking history, were not associated with PFS. In this regard, however, three patients with both G719S (exon 18) and L861Q (exon 21) mutations of EGFR were excluded from univariate and multivariate Cox analysis to evaluate the differences between exon 18 and exon 21.
Discussion
The present study aimed to evaluate the efficacy of EGFR-TKIs in patients with NSCLC with minor mutations of the EGFR gene such as G719X, L861Q and G874S. Among such patients, EGFR mutations G719X and L861Q are found in approximately 3% and 2%, respectively, while G874S is seldom detected (18, 19).

Progression-free survival (PFS) curves after the initiation of tyrosine kinase inhibitor (TKI) treatment as a first- or second-line, or third-line or later.
Prior to the present study, several retrospective reports have discussed the clinical significance of minor EGFR gene mutations in patients with NSCLC (20-22). In a post-hoc analysis of the NEJ002 study which included five patients harboring minor mutations who were treated with gefitinib, the median PFS was 2.2 months and the RR was 20% (21). Another retrospective analysis of 61 patients with minor mutations demonstrated that the median PFS was 5.0 months and the RR was 47.5% (20). In a retrospective study that included 16 patients with a minor mutation, the median PFS was 1.5 months and the RR was 25.0% (22).
In the present study, the RR to EGFR-TKIs in patients with NSCLC with minor mutations of the EGFR gene was 29.5%. This rate is similar to those described in previous studies (20.0% and 47.5%) (20-22). With respect to major mutations of the EGFR gene, the RR to EGFR-TKIs ranged from 62% to 83% (4-7). Taking into account these previous studies and the present study, minor mutations appear to be associated with a lower RR than major mutations.
The PFS of patients with NSCLC with minor mutations of the EGFR gene was 6.7 months in this study. This is also similar to other studies of response to EGFR-TKIs in patients with NSCLC with minor mutations in the EGFR gene (1.5 months and 5.0 months). With respect to major mutations of the EGFR gene, PFS was previously described to be 9.2 to 13.7 months (4-7). Thus, in patients harboring minor EGFR gene mutations, PFS is considered to be shorter than in patients with major mutations.
The PFS of the patients with EGFR gene minor mutations was considered to be relatively good for those who received first- or second-line EGFR-TKI treatment compared to third-line or later, in this study. However, the number of cases was small, and there was not found a statistically significant difference. Indeed, previous reports also suggest that PFS of patients with NSCLC receiving as third or later treatment lines is very short (23-25). Therefore, treatment of NSCLC with EGFR-TKIs as a first- or second-line treatment is considered an appropriate option for patients with minor mutations of the EGFR gene.
This study compared the PFS of NSCLC patients treated with either EGFR-TKI. In multivariate Cox analysis, erlotinib treatment was associated with a longer PFS than gefitinib treatment (p=0.025). An in vitro study by Kancha RK et al. demonstrated that a higher concentration of gefitinib than erlotinib was required to inhibit the growth of cells expressing G719X or L861Q EGFR mutations (26). The in vitro information may suggest the superiority of erlotinib to gefitinib.
Recently, afatinib was approved as a new EGFR-TKI. Afatinib is an irreversible inhibitor of the erythroblastosis oncogene B (ERBB) family that is able to inhibit the kinase domains of EGFR, human EGFR receptor 2 (HER2), HER4, and the transphosphorylation of ERBB3. Three clinical trials assessing the efficacy of afatinib in patients with advanced NSCLC (LUX-Lung 2, LUX-Lung 3, and LUX-Lung 6) included 38 patients harboring minor mutations of the EGFR gene. Among these 38 patients with minor mutations (L861Q, G719X, S768I), the objective RR was 71.1%, the median PFS was 10.7 months, and the median OS was 18.6 months (27). These data suggest that afatinib may have greater efficacy than gefitinib or erlotinib in patients harboring minor EGFR mutations.
The present study has limitations such as its retrospective design, and the inclusion only of Japanese patients. In addition, for most patients, the presence of EGFR gene mutations was confirmed by the PNA-LNA PCR clamp method. The particular methods used may have affected the frequency and positivity rate of mutations identified.
Even under these limitations, our results suggest that EGFR-TKIs represent a beneficial treatment for patients with NSCLC patients harboring minor mutations of the EGFR gene.
Conclusion
Patients with NSCLC harboring minor mutations in the EGFR gene exhibited a modest response to EGFR-TKI treatment. Treatment with first-generation EGFR-TKIs, in particular erlotinib, may be considered a first- or second-line option for patients with NSCLC with minor EGFR mutations.
Acknowledgements
The Authors would like to express their gratitude to the participating patients and to the members of the HANSHIN Oncology Group.
Footnotes
Conflicts of Interest
The Authors have no conflicts of interest.
- Received April 14, 2015.
- Revision received May 13, 2015.
- Accepted May 14, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}