


Abstract
Aim: The aim of the present study was to investigate whether serum markers and clinical factors could be used for preoperative prediction of peritoneal metastasis in gastric cancer (GC) as an indicator for neoadjuvant treatment. Patients and Methods: We enrolled 493 patients with GC for whom preoperative serum tumor markers [carcinoembryonic antigen (CEA) and carbohydrate antigen (CA)19-9], systemic inflammatory marker C-reactive protein (CRP), host immune markers [neutrophil and lymphocyte counts and their ratio (NLR)], albumin as a nutritional marker, and objective preoperative clinical factors were available as indicators of postoperative peritoneal metastasis. Results: Specific clinical factors, including tumor size, histopathology of biopsy sample, and tumor morphology, were significantly correlated with peritoneal metastasis. CA19-9, lymphocyte count and NLR were also predictive factors for peritoneal metastasis. Multivariate analysis identified the clinical factors tumor morphology and histopathology, and laboratory markers CA19-9 and lymphocyte count as independent factors predictive for peritoneal metastasis. A combination of independent predictive factors achieved high predictive accuracy (0.882) for peritoneal metastasis preoperatively. Conclusion: A combination of specific factors is an alternative method to preoperatively discriminate patients with GC with peritoneal metastasis from those without.
One million new cases of gastric cancer (GC) are estimated to have occurred in 2012, making it currently the fourth most common malignancy worldwide (1). Although GC mortality has been reduced by advances in new treatments and in chemotherapy, it still has a poor prognosis and high mortality, second only to lung cancer (1). The prognosis of GC depends on the stage and location (proximal GC has poorer prognosis); when the disease is confined to the stomach mucosa, the 5-year survival rate is near to 95%, but it ranges from 10 to 20% for advanced GC (2). One of the reasons for poor prognosis is that at the time of diagnosis advanced GC with metastatic disease is often detected and it is frequently accompanied by peritoneal metastasis (3, 4). However, an accurate diagnosis of peritoneal metastasis that avoids unnecessary laparotomy or resection is a prerequisite for discussion of treatment strategies.
Imaging studies are frequently used to predict peritoneal metastasis from GC to determine preoperative treatment strategies. Imaging modalities frequently used for the preoperative diagnosis of peritoneal metastasis in GC patients include computed tomography (CT), magnetic resonance imaging (MRI) and positron-emission tomography with 2-deoxy-2-[18F]fluoro-D-glucose integrated with computed tomography (18F-FDG PET/CT). However, a recent meta-analysis revealed that these modalities did not obtain consistently high sensitivity and specificity in assessing peritoneal metastasis of GC (5), making it difficult to assess the efficacy of neoadjuvant protocols in the absence of histopathological confirmation.
Conversely, tumor location, size and morphology, and histopathology in biopsy samples are also objective findings for preoperatively predicting peritoneal metastasis (6). In addition, many serum biomarkers have the potential to act as supplementary tools for further improvement of diagnosis of peritoneal metastasis in patients with GC. For example, studies have demonstrated that preoperative serum tumor markers, including carcinoembryonic antigen (CEA) and carbohydrate antigen (CA)19-9, and laboratory data such as the neutrophil/lymphocyte ratio (NLR), serum C-reactive protein (CRP) and serum albumin, all indices of inflammation, are useful for predicting peritoneal metastasis in GC (7-9).
Thus, in the current study, we evaluated which preoperative objective clinical factors and serum markers reliably predict peritoneal metastasis in GC. Next, we investigated whether the combination of several independent predictors of peritoneal metastasis improved diagnostic accuracy, which may be valuable for treatment planning in patients with GC.
Patients and Methods
Patients. A total of 493 patients (344 men and 149 women) with GC were enrolled at the Mie University Medical Hospital, Japan, between January 1, 2001 and December 31, 2013. No patient received chemotherapy or radiotherapy before surgery and no perioperative mortality was observed. All patients were classified according to the International Union against Cancer TNM Classification (Seventh Edition)(10): 264 patients had stage I disease, 79 stage II, 78 stage III and 72 stage IV. Peritoneal seeding was diagnosed by laparotomy when disseminated nodules were found in the peritoneal cavity, with or without positive cytological results. If ascites was present, a sample of fluid was collected for cytology. In contrast, when ascites was absent, 100 ml saline that was used to wash the peritoneal cavity was collected for cytology. If cytological results were positive, we diagnosed peritoneal metastasis. The Medical Ethics Committee of Mie University Graduate School of Medicine approved this retrospective study (No.2215). The study was conducted in accordance with the guidelines of the 1975 Declaration of Helsinki. The need for informed patient consent was waived because of the retrospective nature of the study.
Preoperative objective clinical factors. The patients' characteristics recorded included age and sex in the current study. Primary tumor data collected preoperatively included the location of the primary tumor (upper, middle or lower stomach), and tumor size and morphology (type 0, I, II, III, IV and V) evaluated by endoscopy (11). Tumor morphological score was defined as follows: superficial type (0), polypoid type (1), ulcerated type (2), local infiltrative type (3), diffuse infiltrative type (4) and mixed type (5). Histopathological diagnosis was evaluated using the preoperative biopsy tissues (well, moderate or poorly differentiated). Histopathological score was defined as follows: well-differentiated adenocarcinoma (0), moderately differentiated adenocarcinoma (1) and mucinous and poorly differentiated adenocarcinoma (2). Peripheral blood samples were collected prior to surgery. Preoperative laboratory data included neutrophil and lymphocyte counts, and albumin, CRP, CEA and CA19-9 levels.
Statistical analysis. The associations between preoperative clinical factors, including CEA and CA19-9, inflammatory status (CRP and albumin), host immune markers (lymphocytes and neutrophils) and clinical peritoneal metastasis, were analyzed using the Mann–Whitney test, Kruskal–Wallis test or χ2 test. Receiver operating characteristic (ROC) analysis was carried out to determine the diagnostic performance of several preoperative clinical factors for distinguishing GC with from that without peritoneal metastasis. Sensitivity versus 1–specificity was plotted at each cut-off threshold and the area under the curve (AUC) values reflect the probability of correctly identifying patients with peritoneal metastasis of GC. The optimal cut-off thresholds for diagnosis were obtained by the Youden's index. Optimal cut-off threshold values were determined at the point on the ROC curve at which the Youden's index (sensitivity+specificity–1) was maximal. A multivariable logistic regression model was used to calculate odds ratios (ORs) associated with peritoneal metastasis according to several preoperative clinical factors. All p-values were two-sided and p<0.05 was considered statistically significant. All statistical analyses were carried out using Medcalc for Windows version 7.2 (Mariakerke, Belgium).
Results
Associations between pre- and postoperative factors and peritoneal metastasis. We examined the relationship between various clinical factors before surgery, including tumor markers (CEA and CA19-9), inflammatory markers (CRP and albumin), immune parameters (neutrophil and lymphocyte counts), and those of intraoperative peritoneal metastasis (Table I). Peritoneal metastasis was significantly associated with large tumor size (p<0.0001), tumor shape (ulcerative/diffuse shape) (p<0.0001), and histopathology (poorly and mucinous adenocarcinoma) on preoperative biopsy (p=0.0005). In addition, levels of preoperative laboratory parameters (higher CA19-9, lower albumin, lower lymphocyte count and higher NLR) were significantly positively associated with peritoneal metastasis in GC (CA19-9, p=0.0002; albumin, p=0.002; lymphocytes, p=0.02; NLR, p=0.007). However, neither age, sex, tumor location nor other serum parameters showed any association with peritoneal metastasis.
We examined the relationship between various postoperative pathological factors and peritoneal metastasis (Table I). As expected, peritoneal metastasis was significantly associated with higher pathological T stage (p<0.0001), higher pathological N stage (p<0.0001), lymphatic duct invasion (p<0.0001), venous invasion (p<0.0001) and higher pathological TNM stage (p<0.0001).
Predictive capacity of peritoneal metastasis in GC using preoperative clinical factors and serum markers. We performed ROC analysis to evaluate the usefulness of preoperative clinical factors and serum markers as convenient biomarkers for the diagnosis of peritoneal metastasis. Cut-off values of each parameter were determined at the point on the ROC curve at which sensitivity+specificity–1 was maximal. ROC analysis demonstrated that tumor size (>47 mm) and shape (score >2) and histopathological findings (score >0) in preoperative biopsies reliably differentiated patients with peritoneal metastasis from those without metastasis (Figure 1), as demonstrated by AUC values of 0.731 [tumor size: 95% confidence interval (CI)=0.690-0.770; p<0.0001], 0.656 (histopathology on biopsy: 95% CI=0.613-0.698; p<0.0001) and 0.852 (tumor shape: 95% CI=0.817-0.882; p<0.0001). In addition, ROC curves revealed that preoperative serum CA19-9 (>24 U/ml), albumin levels (≤3.8 g/dl), lymphocyte count (≤1110×103/ml) and NLR (>2.6423) significantly discriminated GC patients with peritoneal metastasis from those without metastasis (Figure 2), with AUC values of 0.667 (CA19-9: 95% CI=0.624-0.709; p=0.0006), 0.638 (albumin: 95% CI=0.594-0.681; p=0.0016), 0.601 (lymphocyte count: 95% CI=0.556-0.644; p=0.0361) and 0.621 (NLR: 95% CI=0.577-0.664; p=0.0111).
Association between pre- and postoperative clinicopathological findings and peritoneal metastasis.
Independent preoperative predictors of peritoneal metastasis GC. The results from the ROC analysis were strengthened by logistic regression analyses that included variables such as preoperative clinical factors and serum markers. In univariate analysis (Table II), the risk of peritoneal metastasis at laparotomy was significantly higher in patients with large tumor size (>40 mm, p<0.0001); ulcerative, diffuse-type tumor (p<0.0001); higher serum CA19-9 level (>37U/ml, p=0.0002); NLR >2.6 (p=0.0002) and lower lymphocyte count (≤1100×103/ml, p=0.0004). Multivariate analysis revealed that independent preoperative predictors of peritoneal metastases were ulcerative, diffuse-type tumor (OR=16.9251, 95% CI=3.7887-75.6098, p=0.0002), moderate, poorly differentiated, or mucinous adenocarcinoma histopathological findings in biopsy samples (OR=7.6577, 95% CI=1.0-59.6656, p=0.05), higher serum CA19-9 (OR=2.8510, 95% CI=1.2587-6.4576, p=0.012) and lower lymphocyte counts (OR=3.6963, 95% CI=1.4202-9.6199, p=0.0074).

Receiver operating characteristic (ROC) curve analysis using preoperative objective factors for distinguishing patients with and without peritoneal metastasis from gastric cancer (GC). A: Primary tumor size yielded an area under the curve (AUC) of 0.731 (95% Confidence Interval (CI)=0.690-0.770) with 80.49% sensitivity and 64.04% specificity (cut-off value >47 mm) for distinguishing patients with peritoneal metastasis from GC. B: Histopathology in preoperative biopsy samples yielded an AUC of 0.656 (95% CI=0.613-0.698) with 97.73% sensitivity and 27.62% specificity (cut-off value score >2) for distinguishing GC patients with peritoneal metastasis. C: Tumor morphology yielded an AUC of 0.852 (95% CI=0.817-0.882) with 81.82% sensitivity and 77.73% specificity (cut-off value score >0) for distinguishing patients with peritoneal metastasis from GC.
Combination of specific preoperative clinical factors improves prediction of peritoneal metastasis in GC. We performed combined ROC analysis using independent preoperative predictors, such as histopathological type on biopsy and tumor shape, to determine whether this approach can improve the predictive accuracy for peritoneal metastasis in GC. The combination of two preoperative clinical factors successfully identified patients harboring peritoneal metastasis, with a high AUC value of 0.864 (95% CI=0.831-0.893, sensitivity=81.82%, specificity=79.73, p<0.0001; Figure 3A). We added the independent serum markers (CA19-9 and lymphocyte counts) to perform combined ROC analysis. As expected, the AUC value for discriminating peritoneal metastasis increased to nearly 0.9, with high sensitivity and specificity (AUC=0.882, 95% CI=0.850-0.909, sensitivity=84.09%, specificity=82.63, p<0.0001; Figure 3B).
Discussion
The presence of peritoneal metastasis is associated with poor prognosis in patients with GC; therefore, an accurate preoperative diagnosis is necessary to determine the appropriate treatment strategy, since neoadjuvant intraperitoneal and systemic chemotherapy have a positive effect on patients with peritoneal dissemination (12, 13). Although imaging methods such as ultrasonography (US) and CT are the ones most commonly used for prediction of peritoneal metastasis (14, 15), a recent meta-analysis shows that these are not reliable indicators of metastasis (5). Pooled sensitivity for US and CT in detecting peritoneal metastasis was only 0.09 (95% CI: 0.03-0.21) and 0.33 (95% CI: 0.16-0.56), respectively. In contrast, the predictive value of 18F-FDG PET/CT was high in several metastases from GC, including peritoneal metastasis (16); however, it is costly and most patients are unable to afford the procedure. To overcome this problem, recent developments in laparoscopy have made it possible to examine the entire abdominal cavity by staging laparoscopy (17), which has become the main tool for the detection of peritoneal seeding (18, 19). However, it is also costly and time-consuming to perform in all GC patients, because there is no clear indication for the use of staging laparoscopy to detect peritoneal seeding from GC. Further clinical investigation is required to develop the methodologies for the accurate diagnosis of peritoneal metastasis preoperatively.
The most frequently used tumor markers, such as CEA and CA19-9, provide additional diagnostic information in gastrointestinal malignancies (20, 21), but the sensitivity of both markers alone (CEA: 23.91%, CA19-9: 36.96%) (22) is not sufficient for prediction of peritoneal metastasis. In contrast, Hwang et al. demonstrated that preoperative serum CA19-9 levels may provide a predictable value in determining peritoneal metastasis in patients with GC (23). These previous reports are consistent with our data, which revealed that only CA19-9 was significantly associated with peritoneal metastasis. Thus, there exists an urgent need to identify new markers (diagnostic methods) to provide appropriate decision making for the treatment of peritoneal metastasis from GC.
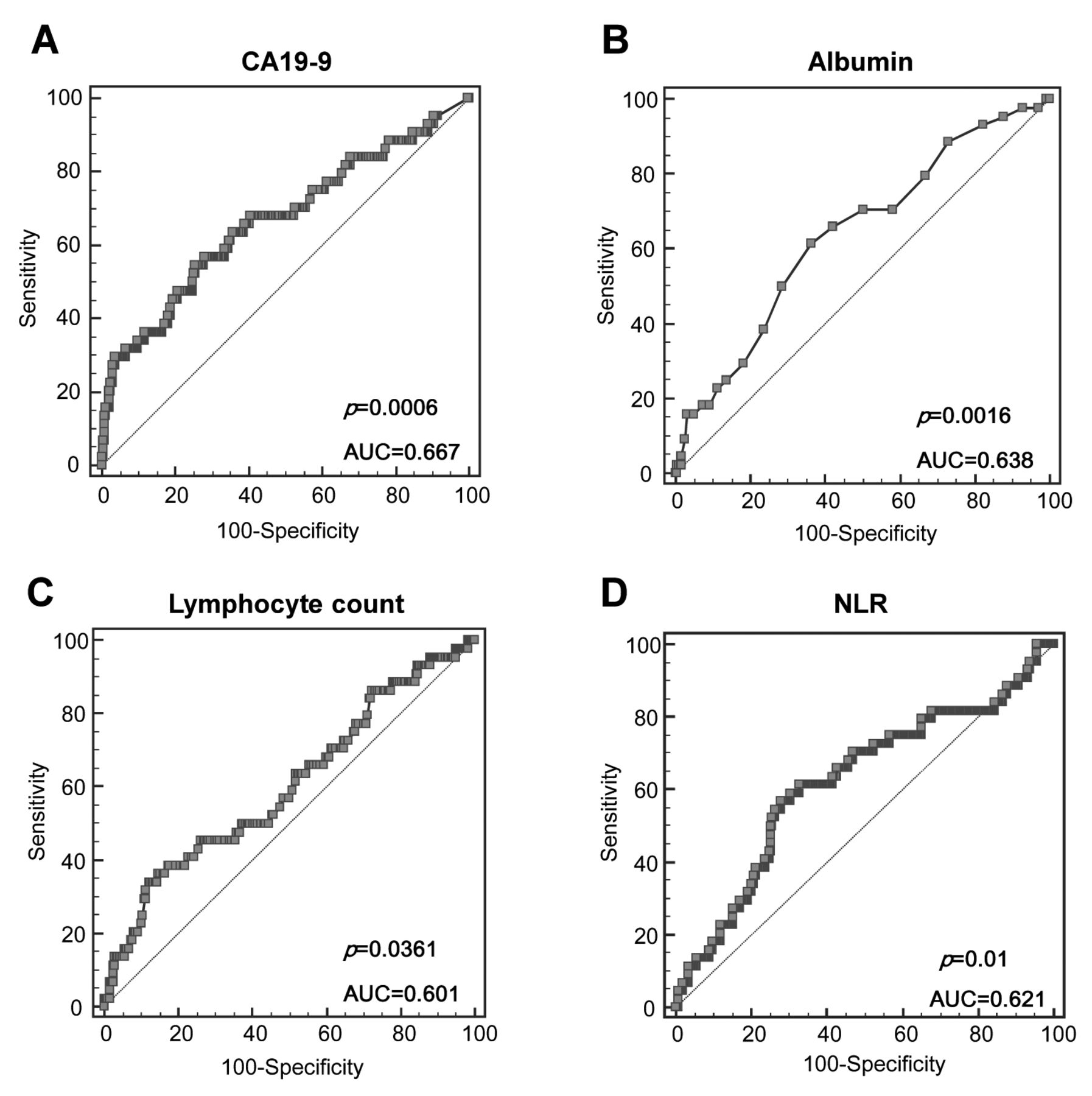
Receiver operating characteristic (ROC) curve analysis using preoperative serum markers for distinguishing gastric cancer (GC) patients with and without peritoneal metastasis. (A) Preoperative serum carbohydrate antigen 19-9 (CA19-9) yielded an area under the aurve (AUC) value of 0.667 (95% Confidence Interval (CI)=0.624-0.709) with 54.55% sensitivity and 74.39% specificity (cut-off value >24 U/ml) for distinguishing GC patients with peritoneal metastasis. (B) Preoperative serum albumin yielded an AUC value of 0.638 (95% CI=0.594-0.681) with 61.36% sensitivity and 63.47% specificity (cut-off value ≤3.8 g/dl) for distinguishing GC patients with peritoneal metastasis. (C) Preoperative lymphocyte counts yielded an AUC value of 0.601 (95% CI=0.556-0.644) with 34.09% sensitivity and 87.75% specificity (cut-off value ≤1110×103/ml) distinguishing GC patients with peritoneal metastasis. (D) Preoperative Neutrophil to lymphocyte ratio (NLR) yielded an AUC value of 0.621 (95% CI=0.577–0.664) with 59.09% sensitivity and 69.71% specificity (cut-off value >2.6423) distinguishing GC patients with peritoneal metastasis.
Changes in the CRP and albumin levels reflect the systemic inflammatory response and immune responses of the host in patients with several cancers. Some studies have indicated a correlation between these laboratory parameters (known as the Glasgow prognostic factor) and prognosis of GC (24-27). However, the association between these markers and peritoneal dissemination has not been fully investigated. In our study, an increase in serum CRP level and decrease in serum albumin levels were correlated with the presence of peritoneal metastasis, which is consistent with a recent study (9). NLR is an easily measurable and simple index of the systemic inflammatory response (28, 29). Increased neutrophils in the blood suppress the host immune reactions, such as the cytotoxic activity of lymphocytes, natural killer cells and activated T-cells (30, 31). In addition, lymphocytes reflect the defensive activity of the host against tumor progression (32). Nakayama et al. recently demonstrated that the NLR is as an independent predictor of peritoneal metastasis in patients with GC, and concluded that its measurement may facilitate the diagnosis of peritoneal metastasis, especially during staging laparotomy (9). Although our results are consistent with their data, our multivariate analysis revealed that using the lymphocyte count alone is a superior marker to NLR for peritoneal metastasis.

Combined Receiver operating characteristic (ROC) curve analysis using preoperative independent predictors for distinguishing gastric cancer (GC) patients with and without peritoneal metastasis. (A) Combined ROC using preoperative independent clinical predictors (tumor type and histopathology in biopsy sample) for predicting peritoneal metastasis yielded an area under the curve (AUC) value of 0.864 (95% Confidence Interval (CI)=0.831-0.893) with 81.82% sensitivity and 79.73% specificity (cut-off value >0.1199) for distinguishing GC patients with peritoneal metastasis. (B) Combined ROC using preoperative independent clinical and serum predictors (tumor type and histopathology in biopsy samples, as well as serum carbohydrate antigen 19-9 (CA19-9) and lymphocyte counts) for predicting peritoneal metastasis yielded an AUC value of 0.882 (95% CI=0.850-0.909) with 84.09% sensitivity and 82.63% specificity (cut-off value >0.1426) distinguishing GC patients with peritoneal metastasis.
Univariate and multivariate analysis of preoperative factors for risk of peritoneal metastasis.
To achieve preoperative detection of peritoneal metastasis from GC, we investigated the diagnostic accuracy for peritoneal metastasis using preoperative features of GC and serum markers, which are objective parameters. Data from our ROC analysis demonstrated that significant predictors included tumor size, histopathology and morphology when endoscopy was performed preoperatively, which is consistent with previous results (6). In addition, preoperative serum CA19-9, albumin, lymphocyte counts and the NLR were also significantly associated with postoperative peritoneal metastasis. However, the diagnostic accuracy of each single parameter was underpowered. Thus, we performed a multivariate logistic regression analysis to identify independent preoperative peritoneal metastatic predictors because a combination of preoperative clinical features and serum molecular features may be able to identify peritoneal metastasis. Several clinical features, including tumor histopathology and morphology, as well as CA19-9 and lymphocyte counts as serum markers, were independent predictors of peritoneal metastasis.
Next, we performed a combined ROC analysis using identified independent clinical predictors including both preoperative tumor features and serum parameters to evaluate whether the diagnostic accuracy of peritoneal metastasis can be increased. As expected, combining independent clinical predictors can increase diagnostic accuracy (AUC=0.882) with high sensitivity (84.09%) and specificity (82.63%). Collectively, we showed that objective evaluation using preoperative predictors of both tumor features and serum markers has the potential to diagnose peritoneal metastasis preoperatively.
In conclusion, we identified that a combination of preoperative tumor features can be a useful detection method for peritoneal metastasis at laparotomy in patients with GC. In addition, adding preoperative serum parameters, which are routinely available, can improve the accuracy of diagnosis of peritoneal metastasis, with high sensitivity and specificity. However, a large prospective study is needed to validate whether our detection method could be used clinically.
Footnotes
↵* These Authors contributed equally to this study.
Conflicts of Interest
The Authors have no conflicts of interest to disclose in regard to this study.
- Received March 13, 2015.
- Revision received March 21, 2015.
- Accepted March 24, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}