


Abstract
Aim: To investigate potential fluctuations in prostate cancer antigen 3 (PCA 3) scores in castration-resistant prostate cancer (CRPC) patients treated with docetaxel and investigate the assay as a potential prognostic factor. Patients and Methods: This was a prospective observational cohort study. Inclusion criteria included patients on hormonal treatment who were recently diagnosed with CRPC. Exclusion criteria included patients previously having radical treatment (surgery or radiotherapy) and patients who have completed the first cycle of chemotherapy. All urine samples were collected and analyzed using the Progensa® assay. Samples were collected before starting chemotherapy and at 12 months. A prospective database was created including routine blood tests, prostate staging and prostate-specific antigen (PSA) levels throughout the study period. The effects of chemotherapy were also recorded. Results: Between January 2010 and February 2013, 12 patients were included in the study out of an initial cohort of 23 patients with CRPC. Mean follow-up was 14.8 months. Mean age at CRPC diagnosis was 73.8 years (±3.6 SD). Mean Gleason score was 8, with PSA 84.23 ng/ml (±158 SD). Mean duration of androgen deprivation treatment (ADT) was 45.16 months (±34.9 SD). Mean time to castrate-resistant state was 46.58 months (±35.3 SD). All twelve (n=12, 100%) patients had non-assessable PCA 3 scores at baseline and at 12 months follow-up. As a direct consequence, statistical analysis was not performed as the anticipated change in PCA 3 scores was not identified and correlation between measurable differences was not possible. All patients tolerated chemotherapy and completed the scheduled cycles with no serious adverse effects. Conclusion: To our knowledge, this is the first prospective study to demonstrate lack of expression of PCA3 in CRPC, with the result apparently not influenced by chemotherapy. There appears to be a strong association between hormonal treatment and lack of PCA 3 expression. It is still unknown whether disease progression per se affects PCA 3 scores. The gradual reduction and eventual complete non-expression of PCA 3 with ongoing treatment and disease progression provide an insight towards molecular pathways that may be connected to castration-resistant state.
- Castration-resistant prostate cancer (CRPC)
- PCA 3
- androgen deprivation treatment (ADT)
- prognostic factor
- docetaxel
Prostate cancer antigen 3 (PCA 3) is a segment of non-coding messenger ribonucleic acid (mRNA) from chromosome 9q21-22 and is over-expressed by a median of 66 times in prostate cancer tissue relative to benign tissues (1). It is not detected in extraprostatic tissues and, unlike prostate-specific antigen (PSA), it is not affected by age, prostate volume or other prostatic diseases (e.g. prostatitis) nor affected by PSA (2, 3). At a cut-off score of 35, PCA 3 has a sensitivity of 64% and specificity of 76% for detecting prostate cancer and presently is used to help determine the need for repeat prostate biopsies in men who have had a previous negative biopsy(4). Several studies have shown the superiority of PCA3 score to PSA in predicting biopsy outcome as increasing scores correspond frequently to a positive biopsy (5, 6). In 2012, the US Food and Drug Administration approved PCA 3 as a diagnostic adjunct to aid clinicians in decision-making regarding repeat biopsies (7). Furthermore, several studies have investigated the relation of PCA 3 to tumor volume and aggressiveness with mixed results (8-10). A pooled analysis of two multi-center European trials that evaluated the significance of PCA 3 in predicting biopsy and prostatectomy specimen characteristics by van Poppel et al. showed a relationship of higher PCA 3 scores with more significant cancers with respect to indolent ones. The authors concluded that PCA 3 should be included in the decision-making process for active surveillance (11).
Criteria for definition of castation-resistant prostate cancer (CRPC).
Overall, there exists a large body of evidence to substantiate the integration of PCA 3 in risk stratification models for prostate cancer diagnosis (12). However, to this day, very little is known about the usefulness of PCA 3 as a marker of treatment response and its role in advanced disease. In this article, we present our study of PCA 3 in a population of patients with advanced prostatic malignancy aiming to identify any correlation with disease progression and treatment response.
The primary end-point of our study was to investigate potential fluctuations in PCA 3 scores in patients with castration-resistant prostate cancer (CRPC) treated with docetaxel and investigate the assay as a potential prognostic factor. Secondary outcome measures included correlation of PCA 3 with laboratory and cancer staging parameters in disease progression during chemotherapy.
Materials and Methods
This was a prospective observational cohort study conducted in compliance with all relevant institutional, scientific and ethical committee review boards and local regulatory requirements. Informed consent was obtained from all patients. Inclusion criteria included adult patients diagnosed with locally advanced or metastatic prostate cancer (T3) who have not had any treatment other than androgen deprivation therapy (ADT), recently diagnosed with CRPC, as defined in Table I, who were suitable for chemotherapy with docetaxel. Other inclusion criteria were Eastern Cooperative Oncology Group (ECOG) score less than 2 and expected survival of more than 12 months. Exclusion criteria included patients previously having radical treatment (surgery or radiotherapy) and patients who have completed the first cycle of chemotherapy, as well as patients with other concomitant malignancy (urological extraprostatic, skin, liver, lung, gastrointestinal tract, brain, muskuloskeletal). Patients were recruited from the existing pool of follow-up appointments at our academic centre. All patients underwent digital rectal exam (DRE) and prostatic massage to obtain urine samples that were collected and analyzed using the Progensa® assay (Gen-Probe, San Diego, CA, USA) at baseline (i.e. before starting chemotherapy) and at 12 months. PCA 3 scores were calculated as 1,000 × (PCA 3 m RNA copies/PSA m RNA copies) and all the samples were processed in the same accredited laboratory (Genekor SA®, 45 Lavriou Ave, 15354, Athens, Greece). A PCA 3 score cut-off of 35 was determined as diagnostically significant. Non-assessable or non-informative PCA 3 results were also considered. Baseline routine blood function tests and biochemistry, PSA and PSA ratio, prostate volume (assessed by transrectal ultrasonography (TRUS)), prostate cancer diagnosis and staging information (initial biopsy PSA and Gleason score, nodal status and evidence of visceral and bone metastases), as well as duration of androgen deprivation and side effects of chemotherapy were collected on presentation and included in a prospective database, which was updated at 12 months follow-up.
Docetaxel chemotherapy was administered as the standard regimen of intravenous 75 mg/m2 three times weekly along with prednisolone 10 mg/day. Up to 10 cycles of treatment were planned. Dose reduction was offered to patients with serious neutropenia and/or sepsis, along with granulocyte colony-stimulating factor. Adverse effects and additional management were recorded.
For statistical analysis, a repeated measure ANOVA test was selected in order to correlate PCA 3 scores pre- and post-chemotherapy and also with variables that prognosticate disease response to treatment (i.e. post-chemotherapy PSA, extent of visceral and bone metastases and worsening of symptoms). Level of statistical significance was considered as p<0.05.
Results
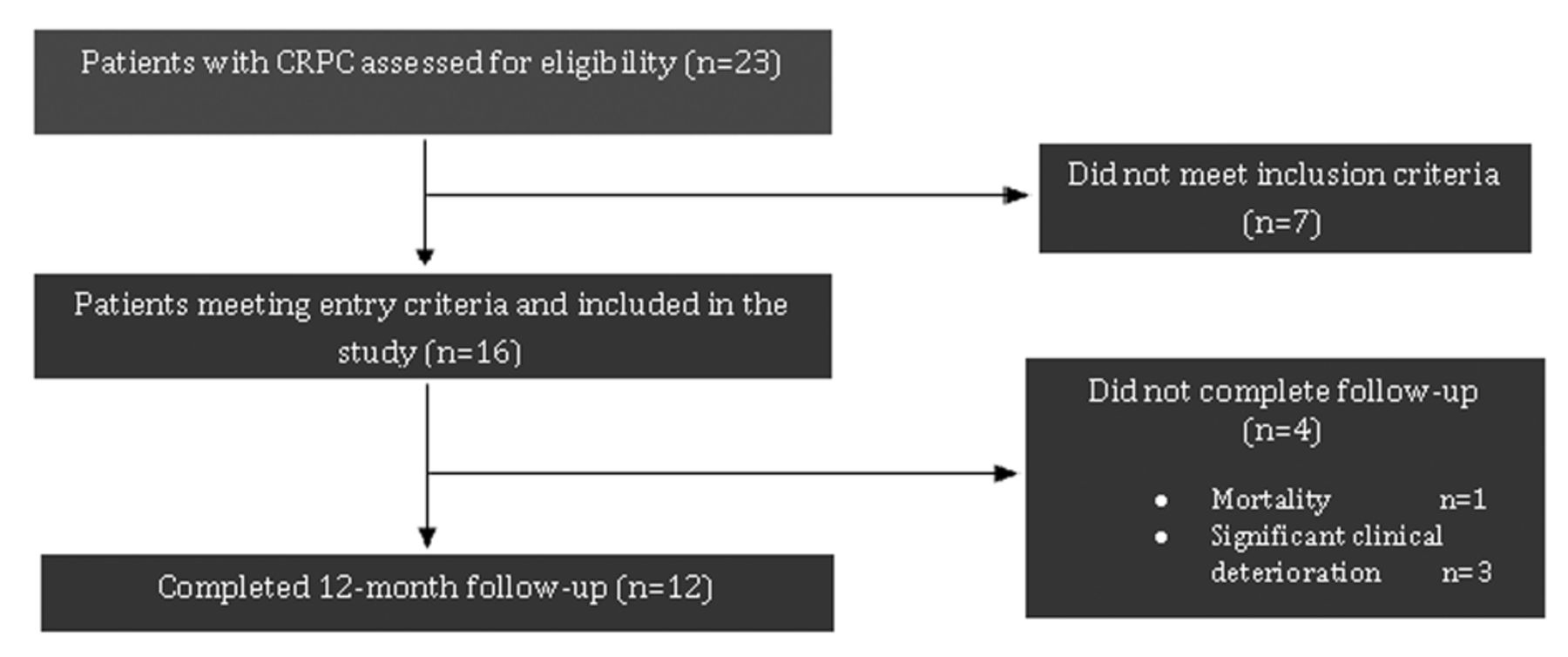
Between January 2010 and February 2013, a total of 23 patients were identified with CRPC. Out of those, 16 patients met the inclusion criteria and were originally included in the study. During the initial follow-up period one patient unfortunately passed away and three more deteriorated significantly and could not continue the study. The remainder 12 patients who met the inclusion criteria completed the initial 12 months and were followed up until disease progression (Figure 1). Mean age at CRPC diagnosis and inclusion in the study was 73.8 years (±3.6 SD). Mean Gleason score at initial diagnosis was 8, with mean PSA 84.23 ng/ml (±158 SD). ADT consisted of luteinizing hormone-releasing hormone agonist (8 patients goserelin acetate, 5 patients leuprorelin acetate, 3 patients triptorelin) in combination with a non-steroidal anti-androgen for the first four weeks in all patients. Mean duration of ADT was 45.16 months (±34.9 SD). Mean time to castrate-resistant state from original diagnosis was 46.58 months (±35.3 SD). Mean PSA at CRPC diagnosis was 230.51 ng/ml (±296.75 SD), with free PSA 58.6 ng/ml (±90.3 SD) and PSA ratio 0.26 ± 0.11 SD. Mean prostate volume, as measured by TRUS, was 40.1 cc (±17.6 SD). Mean ECOG score was 1. Mean overall follow-up was 14.8 months. Post-chemotherapy PSA at 12 months follow-up was 181.98 ng/ml ± 306.2 SD, free PSA 66.55 ng/ml ± 142.0 SD and PSA ratio 0.34±0.1 SD. A summary of the results is provided in Table II.
Results of the major study parameters per patient and mean values.
All twelve (n=12, 100%) patients had non-assessable PCA 3 scores at baseline and at 12 months follow-up. Of note, PCA 3 score was non assessable due to PSA mRNA levels below the level of detection in all sixteen (n=16) patients at baseline. As a direct consequence, statistical analysis did not take place as the anticipated change in PCA 3 scores was not identified and correlation between measurable differences was not possible. Integration of a time-to-event model was also not possible again because there was no measurable difference to begin with.
All patients tolerated chemotherapy well for the first three months, with no adverse effects, and bone pain improved significantly. In the following cycles, one patient experienced neutropenic sepsis that was successfully treated, three patients experienced low-grade fever, malaise and anorexia, which did not alter treatment, and two patients experienced anorexia, diarrhea and vomiting. All patients completed the scheduled treatment cycles with significantly improved symptoms and no new metastases during the study follow-up period.

Process of patient selection into the study. CRPC, castration-resistant prostate cancer.
Discussion
Early efforts to identify the influence of medical intervention on PCA 3 scores have produced equivocal results. In their pilot study, van Gils et al. investigated the effect of dutasteride on the PCA3 score to find a variable and unpredictable response, albeit in a small, mixed cohort of patients with benign prostatic hyperplasia and localized prostate cancer (13). The only other study to date that investigated the prospective role of PCA 3 as a prognostic marker for advanced disease and treatment response was The Triptocare study. It consists of a prospective, open-label, multicentre, single-arm phase III study of triptorelin 22.5 mg in men with locally advanced and/or metastatic disease who were previously naive to ADT and results were recently published (14). The study assessed PCA 3 and TMPRSSG-ERG scores at baseline and after 1, 2 and 6 months of treatment with triptorelin. In a population of 322 patients, 39 (12.1%) had non-assessable PCA3 at baseline. The frequency of non-assessable PCA 3 increased with time on androgen deprivation, namely 109 patients at 1 month (33.9%), 215 patients (68.7%) at 3 months and 232 patients (77.9%) at 6 months of treatment. Of great interest is the finding of the proportion of hormone-naive individuals who never expressed PCA 3 at baseline (n=39, 12.1%). This sub-group was not further investigated, however, as it was not part of the initial objective. As the majority of these patients had a Gleason score of equal or greater than 8, the paucity of PCA 3 detection could be attributed to higher grade and/or more advanced disease. In their assessment of PCA 3 expression in radical prostatectomy specimens, Robert et al. have demonstrated lower PCA 3 scores in high-grade cancers (15). Furthermore, high Gleason score at baseline was the only factor significantly correlating to non-assessability of PCA 3 at 6 months in the Triptocare study (14). On the other hand, the investigators also point-out that in the remainder of the study group, lower PCA 3 scores expression correlated significantly with higher baseline PSA values (>200 ng/ml). This is somewhat contradictory, as it was shown in the early research by Partin et al. that patients with advanced disease and higher grade and volume tumors are more likely to produce less PSA per gram tissue as a consequence of decreased differentiation (16).
The disruption of prostatic architecture in higher-grade tumors has also been postulated as an explanation for low PCA 3 scores. The loss of glandular pattern in higher Gleason score cancer leads to obliteration of the ducts and lumen, thus making it difficult to disseminate prostatic cells in the urine in order to achieve a measurable result (17). Histopathological changes in hormonally treated prostate cancer cells are mainly characterized by cellular shrinkage with little cytoplasm that translates to glandular shrinkage and an overall reduction in size. DRE in these patients often reveals a small, hard prostate. However, this hypothesis is contradicted by the fact that, although PCA 3 score was not assessable, prostate cells were identified in the urine of all patients in our study suggesting a molecular rather than a mechanical mechanism.
According to our findings, another possible mechanism would be an ablative effect of androgen deprivation to PCA 3 expression, something also shown in the Triptocare study. Continuation of ADT in CRPC patients throughout the chemotherapeutic period constitutes common practice and probably relates better to our results than any effect of docetaxel treatment. In our study, PCA 3 was non assessable both at baseline and at 12 months follow-up after the completion of chemotherapy. Based on the above findings, further research is required to answer the questions of the true nature of PCA 3 mRNA in prostate cancer molecular pathogenesis pathways and its expression during the various stages of progression. The Triptocare investigators point out, in addition, that hormone-naive patients with metastases produced significantly lower PCA 3 scores than men without metastases(14) In our study of exclusively metastatic patients, non-assessable PCA 3 score was the rule, which substantiates further the hypothesis of declining PCA 3 expression with ADT and advancing disease.
In both studies, PCA 3 score failed to prove as a marker for disease prognostication and treatment response. Nevertheless, paucity of PCA 3 expression with ADT has never been demonstrated previously and this discovery may have yet to reveal its full potential. In retrospect, the evident gradual decrease in PCA 3 score detection with ongoing ADT and the eventual complete non-assessability demonstrated in our cohort appear to be sequential events. The EFFECT trial is another prospective open label, single arm, multicentre trial that is currently ongoing and investigates the effect of leuprorelin acetate at 6 months on PSA, PCA 3 and TMPRSS2-ERG-mRNA amongst other markers. In our cohort, 8 patients received goserelin acetate, 5 patients leuprorelin acetate, 3 patients triptorelin previously and continued throughout chemotherapy. The trial aims to recruit 50 patients and compare testosterone and PSA with the newer biomarkers to provide more evidence and much needed answers in the field of advanced prostatic malignancy (18).
Conclusion
To our knowledge, this is the first prospective study to demonstrate a lack of expression of PCA 3 in CRPC, with the result apparently not influenced by chemotherapy. There appears to be a strong association between hormonal treatment and non-assessable PCA 3 score, probably by means of an ablative effect to gene expression. Although preliminary evidence from other studies supports this theory, it is still unknown whether disease progression per se affects PCA 3 scores. The ongoing EFFECT trial will add to the existing evidence. The gradual reduction and eventual complete non-expression of PCA 3 with ongoing treatment and disease progression provide an insight towards molecular pathways that may be connected to events leading to castration-resistant state.
Acknowledgements
This study constitutes part of the PhD thesis of Mr. Andreas Bourdoumis and was funded by Sanofi-Aventis® regarding PCA 3 assay and sample collection and processing. Genekor SA®, which is the main collaborating laboratory of Gen-Probe® in Greece, assisted with assay and sample shipping, handling and processing. All the authors contributed in study design, patient recruitment and collection of data.
- Received January 29, 2015.
- Revision received February 22, 2015.
- Accepted February 24, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.