


Abstract
Aim: To identify patients with metastatic renal cell carcinoma (mRCC) who received tyrosine kinase inhibitors (TKIs) in both first- and second-line settings in order to investigate the association of oncological outcomes between the two lines of therapy. Patients with Methods: The study included 76 consecutive patients with mRCC treated with second-line TKI therapy after the failure of first-line TKI therapy. The association of oncological outcomes between first- and second-line therapies was analyzed in these 76 patients. Results: In this series, the objective response rates (ORRs) to first- and second-line TKI therapies were 10.5% and 25.0%, respectively. The ORR to second-line TKI therapy was not significantly different among patients achieving a complete or partial response, stable disease and progressive disease to first-line TKI therapy (37.5%, 21.6% and 29.4%, respectively; p=0.34). The median durations of progression-free survival (PFS) with first- and second-line TKI therapies were 7.9 and 8.1 months, respectively, and there was no significant correlation between them (p=0.78). Out of the examined factors, the pre-treatment C-reactive protein level, number of metastatic sites and Memorial Sloan-Kettering Cancer Center risk classification model, but not the response to first-line TKI therapy, were independently associated with PFS on second-line TKI therapy, based on multivariate analysis. Conclusion: The clinical response to second-line TKI therapy is not dependent on that to first-line TKI therapy in patients with mRCC; therefore, it may not be necessary to switch to an alternative agent with a mechanism different from TKIs as second-line therapy, even if patients do not respond to first-line TKI therapy.
- Tyrosine kinase inhibitor
- metastatic renal cell carcinoma
- first-line
- second-line
- objective response
- progression-free survival
Until recently, immunotherapy using cytokines had been the mainstay of systemic treatment for patients with metastatic renal cell carcinoma (mRCC), yet only limited efficacy can be achieved with this treatment, with a median overall survival of approximately one year (1). To overcome the unfavorable prognostic outcomes of mRCC, a variety of novel agents that target major signaling pathways mediating the progression of RCC have been introduced into clinical practice, and the use of these agents has resulted in marked improvement in the prognosis of patients with mRCC (2). However, it is well-recognized that the majority of patients with mRCC treated with molecular-targeted agents will eventually acquire resistance to these agents and subsequently develop progressive disease. Accordingly, after the failure of the initial molecular-targeted agent, it is generally necessary to continue sequential lines of therapy using a different agent to further maintain disease control (3, 4).
Out of the several types of molecular-targeted agent, tyrosine kinase inhibitors (TKIs), which have been shown to exert antitumor activity by inactivating vascular endothelial growth factor (VEGF)-related pathways, are currently regarded as playing central roles in the treatment of patients with mRCC, particularly as the first-line standard-of-care (5), based on the outcomes of pivotal randomized clinical trials (6-9). Furthermore, favorable clinical outcomes from using TKIs against mRCC were achieved in various studies evaluating the efficacies of these agents in routine clinical settings (10-15). However, limited data have been made available with respect to sequencing therapy for identifying the most effective second-line agent after the failure of initially introduced TKIs. It has always been believed that patients achieving a response to first-line TKI therapy will favorably respond to another second-line TKI therapy, and non-responding patients should switch to an alternative agent with a mechanism of action different from TKIs (16, 17). However, Al-Marrawi et al. recently reported that there was no significant correlation of disease control between VEGF-targeting agents used in first- and second-line settings (18).
Patients characteristics prior to first-line therapy with tyrosine kinase inhibitors.
Considering these findings, we retrospectively assessed the clinical outcomes in a total of 76 consecutive patients with mRCC who were treated with second-line TKI therapy following the failure of first-line TKI therapy, focusing on the association of efficacies between the first- and second-line treatments.
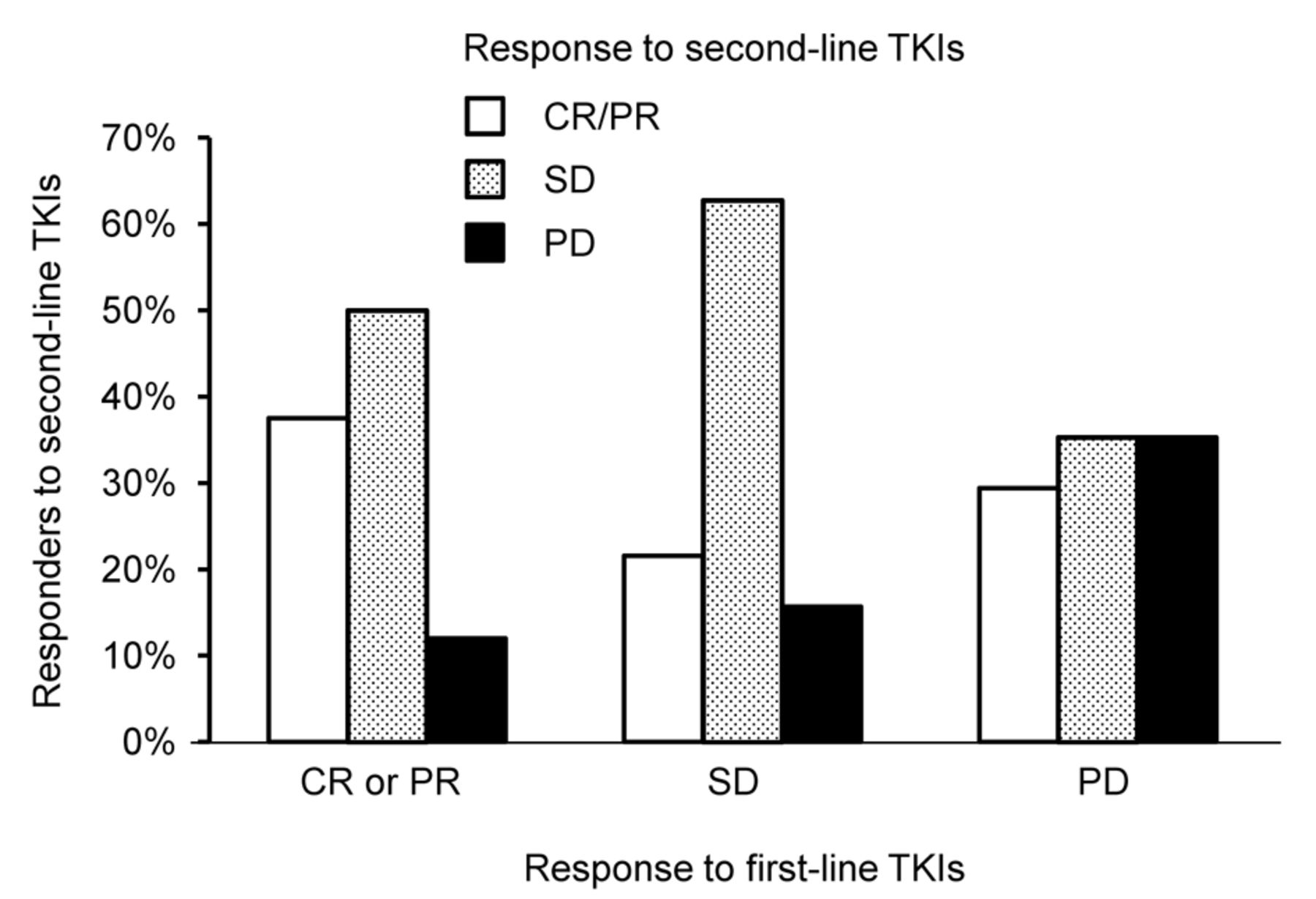
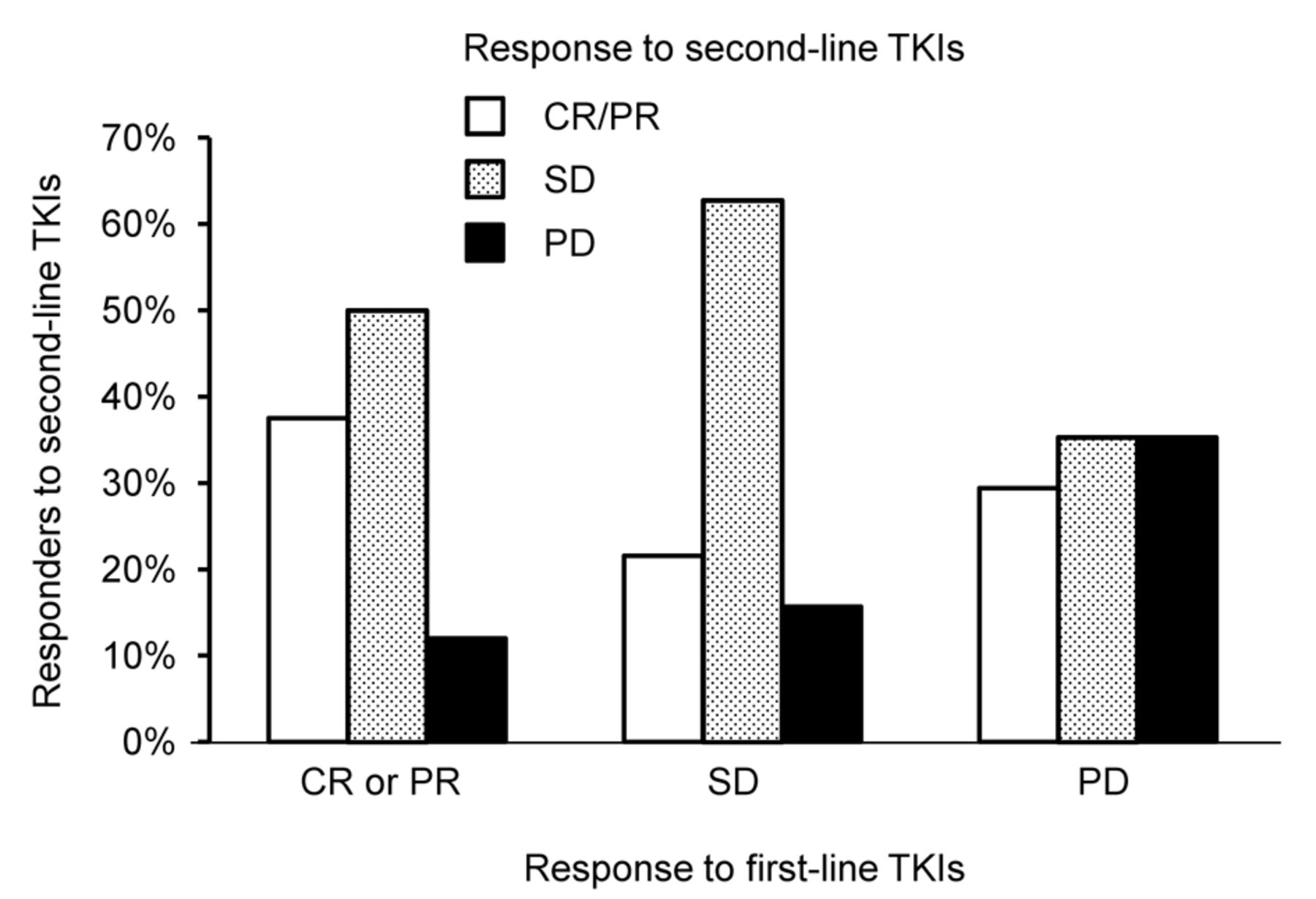
Best response to second-line tyrosine kinase inhibitors (TKIs) according to initial best response to first-line TKIs in 76 patients with metastatic renal cell carcinoma. CR, Complete response; PR, partial response; SD, stable disease; PD, progressive disease.
Patients and Methods
Patients. We retrospectively reviewed data from 354 patients with mRCC treated with molecular-targeted agents in a routine clinical setting at our Institutions between April 2008 and March 2014. Out of these 354, this study included a total of 76 consecutive patients with mRCC who fulfilled the following criteria: clear cell RCC was histopathologically diagnosed in either primary or metastatic lesions; TKI therapy was introduced as initial treatment for mRCC, and failure of this first-line TKI therapy was then noted; a TKI different from that used as the first-line agent was subsequently administered as a second-line agent. Prior to participation in the study, informed consent was obtained from each patient, and the study design was approved by the Research Ethics Committee of our Institution. (No.22002, No.220025)
Administration of TKIs. In this series, TKIs were administered according to the following schedule: sorafenib: 400 mg orally, twice daily; sunitinib: 50 mg orally, once daily in repeated 6-week cycles consisting of 4 weeks on therapy, followed by 2 weeks off; axitinib: 5 mg orally, twice daily. As a rule, TKI dose modification was permitted as follows: sorafenib: dose was reduced from 800 to 400 mg once daily, followed by additional dose reduction to a single 400-mg dose every other day according to adverse events (AEs); sunitinib: dose reduction was from 50 to 37.5 mg once daily, and then to 25 mg once daily based on AEs; axitinib: an increased dose of 7 mg twice daily was allowed for patients who tolerated the standard dose for at least 2 weeks unless the blood pressure was >150/90 mmHg or antihypertensive medication was being administered, and the dose was reduced to 3 mg twice daily and then further to 2 mg twice daily according to AEs.

Progression-free survival on first-line (a) and second-line (b) therapy with tyrosine kinase inhibitors in 76 patients with metastatic renal cell carcinoma.
Evaluation. As baseline evaluations, the clinicopathological examinations and performance status (PS) were assessed based on the TNM classification (24) and Karnofsky PS scale, respectively, while risk classification was conducted using both Memorial Sloan-Kettering Cancer Center (MSKCC) (19) and Heng et al.'s risk classification systems (20). Before the introduction of first- and second-line line TKIs, the radiological evaluation of all patients was performed by computed tomography (CT) of the brain, chest and abdomen with/without radionuclide bone scan. As a rule, tumor measurements were repeated by CT every 12 weeks during treatment with TKIs. Responses and AEs were evaluated by the treating physician based on the Response Evaluation Criteria in Solid Tumors 1.1 (25) and National Cancer Institute Common Terminology Criteria for Adverse Events version 3.0, respectively.
Statistical analysis. All statistical analyses were performed using Statview 5.0 software (Abacus Concepts, Inc., Berkley, CA, USA), and p-value less than 0.05 was considered significant. Differences in the response to second-line TKIs were compared according to that to first-line TKIs by the chi-square test. Pearson's correlation coefficient analysis was performed to assess the association of progression-free survival (PFS) between first- and second-line TKI therapies. The PFS rates were calculated employing the Kaplan–Meier method, and differences were determined by the log-rank test. The prognostic significance of certain factors was assessed using the Cox proportional hazards regression model.
Results
Table I summarizes the characteristics of the 76 patients with mRCC who were treated with TKIs as both first- and second-line therapies. As shown in Table II, 54 and 22 received sorafenib and sunitinib, respectively, as first-line agents, while 49, 22 and 5 were treated with sunitinib, axitinib and sorafenib, respectively, as second-line agents. The objective response rates (ORRs) for first- and second-line therapies were 10.5% and 25.0%, respectively. The ORR in patients receiving first-line sunitinib was significantly higher than that in those receiving first-line sorafenib (p=0.0021); however, there were no significant differences in the ORRs according to the TKIs administered as second-line agents (Table II).
Figure 1 shows the best response to second-line TKIs grouped by the initial best response to first-line TKIs. The ORRs to second-line TKIs in patients who achieved a complete response (CR) or partial response (PR), stable disease (SD) and progressive disease (PD) as the best response to first-line TKIs were 37.5%, 21.6% and 29.4%, respectively. There was no significant correlation of the best response between first- and second-line TKIs (p=0.34).
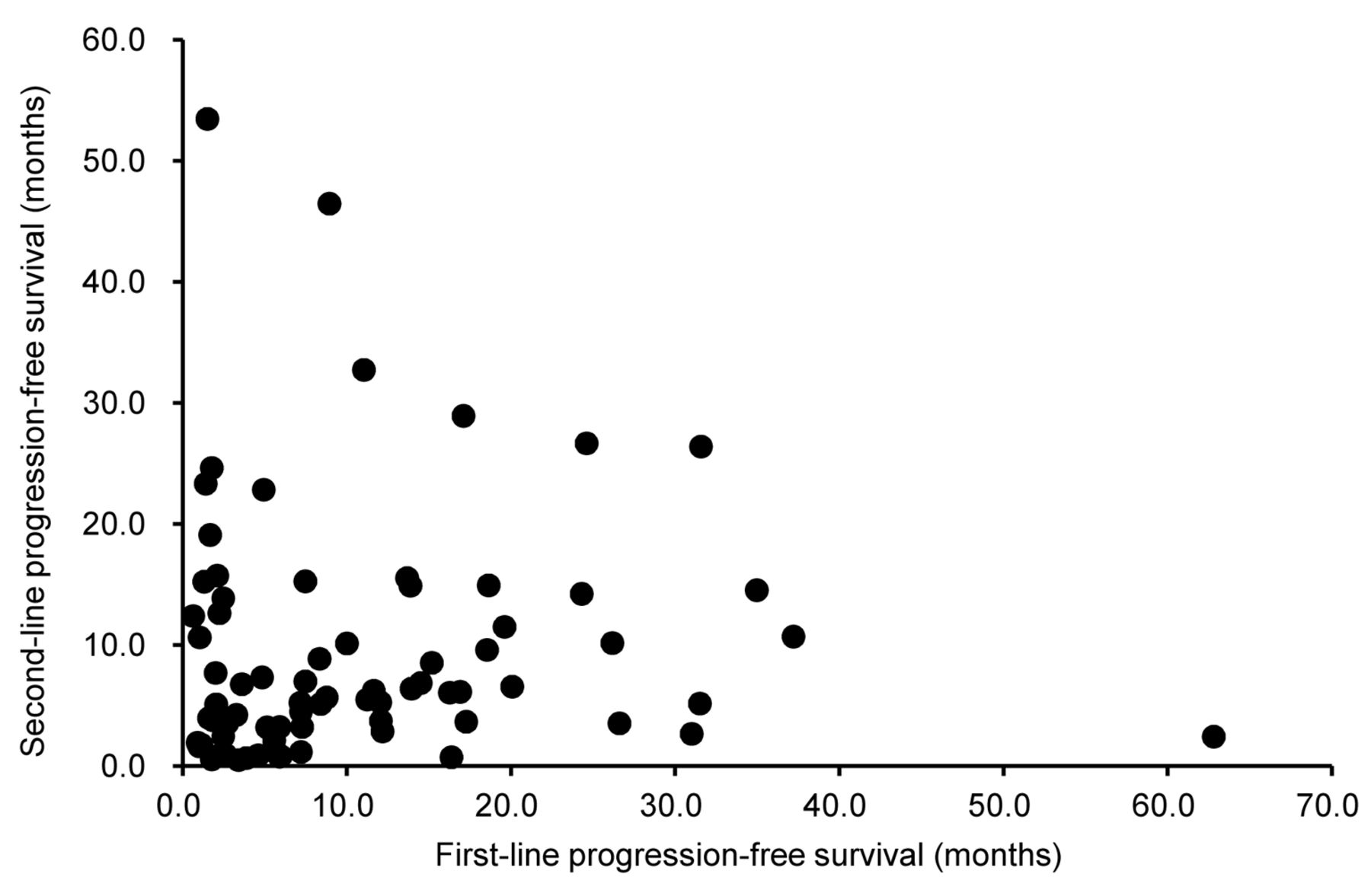
As shown in Figure 2, the median durations of PFS following the introduction of first- and second-line TKIs were 7.9 and 8.1 months, respectively. No significant correlation of PFS was noted between first- and second-line TKIs (Pearson correlation coefficient=0.033, p=0.78). Uni- and multivariate analyses were then performed to assess the impacts of several factors, including the response to first-line TKIs, on the PFS on second-line TKI therapy (Table III). Univariate analysis identified C-reactive protein (CRP) level, number of organs with metastases, liver metastasis and MSKCC classification (p=0.0032, 0.027, 0.024 and 0.011, respectively), but not the response to first-line TKIs (p=0.97), as predictors of the PFS on second-line TKI therapy, of which only the CRP level, number of organs with metastases and MSKCC classification appeared to be independently associated with the PFS on second-line TKI therapy on multivariate analysis (p=0.0049, 0.026 and 0.011, respectively).
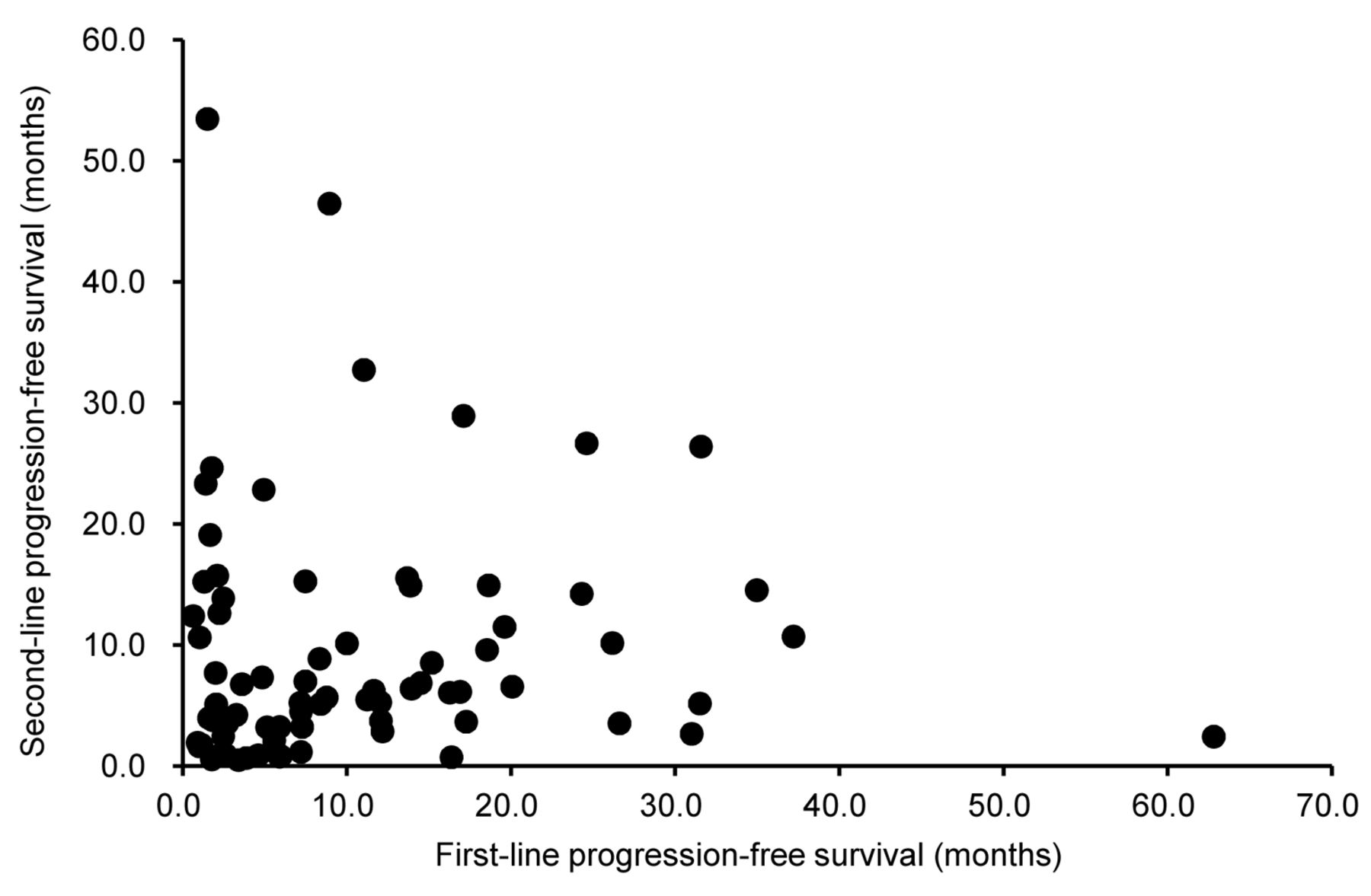
Correlation of progression-free survival between first- and second-line tyrosine kinase inhibitor therapies in 76 patients with metastatic renal cell carcinoma.
Discussion
As a result of the pivotal randomized phase III clinical trials (7, 9), TKIs are currently regarded as a new reference standard-of-care for the first-line treatment of mRCC, except for patients classified into the poor risk group (5). In addition, the therapeutic efficacies of TKIs shown in the clinical trials were subsequently confirmed in various studies targeting mRCC in patients treated with TKIs in routine clinical practice (10-15). However, the selection of second-line agents following the failure of first-line TKI therapy remains controversial; therefore, second-line agents tended to be chosen based on responses to first-line TKIs (16, 17), but with few data to support this practice. Considering these findings, we conducted the retrospective assessment of clinical outcomes in a total of 76 patients with mRCC who were treated with both first- and second-line TKIs in order to evaluate the association of the efficacies between the first- and second-line TKI therapies.
In this series, no significant correlation of the ORRs was noted between first- and second-line TKIs, that is, patients who were refractory to treatment with first-line TKIs still achieved an approximately 30% ORR to second-line TKIs. In addition, based on the data from the International mRCC Database Consortium, Al-Marrawi et al. also reported that the ORR to second-line VEGF-targeted therapy was 11%, with ORRs of 14%, 10% and 11% in patients with mRCC who were judged to have CR or PR, SD and PD, respectively, as the best response to first-line VEGF-targeted therapy (18). Considering these findings, it may not be necessary to consider the response to first-line TKIs when determining agents which will subsequently be administered as second-line therapy.
We then assessed the PFS on treatment with both first- and second-line TKIs, and showed the absence of a significant correlation in the PFS between these two lines of TKI therapy. With respect to the association of the PFS between first- and second-line VEGF-targeted therapies as well, Al-Marrawi et al. reported an outcome similar to that of our study (18). In fact, we also showed that there was no significant impact of the response to first-line TKIs on the PFS while on second-line TKI therapy, while the CRP level, number of metastatic organs and MSKCC classification were identified as independent predictive factors for PFS on second-line TKI. Collectively, these findings suggest that PFS following first-line TKI may not be indicative of PFS while on another TKI subsequently introduced as a second-line agent.
It is of interest to select an optimal second-line agent for patients with mRCC following the failure of first-line TKI based on the present findings. Currently, two agents are recommended, showing a high level of evidence for the treatment of mRCC after the failure of initial VEGF-targeted therapy (8, 21). Everolimus is an orally available inhibitor of the mammalian target of rapamycin and is an approved agent after the failure of one or more VEGF-targeted therapies (21), while axitinib, a potent inhibitor of VEGF receptors, has also been shown to improve PFS over sorafenib in patients who previously received one prior systemic therapy against mRCC (8). To date, there has been no randomized trial directly comparing the efficacies of these two agents as second-line therapy for mRCC patients refractory to first-line VEGF-targeted therapy; however, based on the present outcomes, second-line axitinib may be a reasonable candidate for the majority of patients with mRCC, irrespective of the clinical course with the first-line VEGF-targeted-agent.
Best response to first- and second-line therapies with tyrosine kinase inhibitors.
Uni- and multivariate analyses of several parameters as predictors of progression-free survival.
We would also like to emphasize several limitations of the study. Firstly, this was a retrospective study, and the sample size was not large enough to draw definitive conclusions. Secondly, due to the timing of the approval of molecular-targeted agents, a significant proportion of patients were not treated based on the currently recommended therapeutic strategy for mRCC. In addition, the number of patients who were treated with first-line sunitinib and second-line sorafenib was small, therefore the effect of sequential use of sorafenib following to sunitinib may be uncertain. Finally, this study included only Japanese patients with mRCC, who have been shown to exhibit profiles associated with the use of molecular-targeted agents different from those of Western populations (22, 23); therefore, it may be difficult to apply the present findings to all patients with mRCC.
In conclusion, the present study found no significant correlation of disease control between first- and second-line TKIs as measured by the best response or PFS in a total of 76 consecutive patients with mRCC who were treated with second-line TKI therapy after the failure of first-line TKI therapy. Therefore, the efficacy of first-line TKI therapy was not a useful criterion upon which to select a second-line agent for mRCC. However, further study with a prospective setting is necessary to identify reliable clinical parameters that predict the response to second-line therapy to achieve the optimal sequencing of TKI therapy for patients with mRCC.
- Received January 28, 2015.
- Revision received February 10, 2015.
- Accepted February 13, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}