


Abstract
Serum levels of thymidine kinase 1 (TK1), an enzyme involved in the G1-S phase of the cell cycle, have been previously shown to correlate with the prognosis of lymphoid malignancies. We hypothesized that TK1 levels will be higher in aggressive, compared to indolent lymphoproliferative, malignancies and this may serve as a marker of transformation from an indolent to aggressive disease. We analyzed serum from 182 patients and correlated the findings with the type of malignancy and prognosis; we further compared the TK1 levels of 31 patients with a proven transformation and 34 patients with clinically suspected transformation that was eventually deferred. The mean TK1 levels of patients with indolent and aggressive disease was 18.9±3.3 and 39.8±3.3 U/l respectively (p<0.001). Among patients with aggressive disease, low TK1 levels correlated with improved survival (p=0.008). TK1 levels >16.6 U/l predicted transformation from indolent to aggressive disease (sensitivity of 95%, specificity of 76%, negative predictive value (NPV) of 96% and positive predictive value (PPV) of 69%). A regression analysis showed that only TK1 levels were significant (relative risk (RR)=1.03 for each unit, confidence interval (CI)=1-1.05; p=0.015) for diagnosing a true transformation. In conclusion, TK levels are useful in assessing prognosis, especially in aggressive lymphoproliferative diseases. Moreover, TK levels are adequate in discriminating cases of indolent lymphoma that transformed to an aggressive disease from patients with no proven transformations. This tool provides the clinician a novel method to distinguish between symptomatic patients utilizing a simple test and may lessen the need for aggressive or invasive measures of investigation.
Hematological malignancies account for approximately 10% of all cancers. Of these, the lymphoproliferative neoplasms are most prevalent, arising from a transformed B or T lymphocytes, at various stages of the lymphoid lineage differentiation (1, 2). The lymphoproliferative neoplasms are further divided into indolent and aggressive diseases depending on their clinical course. The most common indolent lymphoid tumors are follicular lymphoma (FL), marginal zone lymphoma (MZL) and small lymphocytic lymphoma or leukemia (SLL/CLL). Among the aggressive lymphoid malignancies, diffuse large B cell lymphoma (DLBCL) is the most common, while others, such as T-cell lymphoma (TCL) and acute lymphoblastic lymphoma/leukemia are less common. Prognosis assessment includes various scoring systems and markers for each disease (1, 3-9). However, β2-microglobulin β(β2M) appears uniformly as an established marker correlating with long term survival (4-6, 9-11). Other markers, such as lactate dehydrogenase (LDH) and serum thymidine kinase 1 (TK1), have been reported with various results (1, 3, 6-8, 12), most significantly in CLL (10).
A subset of patients with indolent lymphoma may suffer from a transformation to an aggressive lymphoma, often fatal despite treatment (1, 13, 14). Such a transformation from indolent to aggressive lymphoma is relatively uncommon accounting for 5% of CLL patients and up to 25% of FL lymphomas. It is usually heralded by constitutional symptoms (alias ‘B’ symptoms), which are non-specific and may be difficult to diagnose (13-15). These symptoms may frequently accompany infections and indolent diseases. Differentiating a transformation from a more indolent form is critical as treatment may be diverse and prognosis dismal. A definite diagnosis of transformation is made by a biopsy of a suspected mass or lymph node.
Patients' baseline characteristics.
Cytosolic tyrosine kinase (TK) is a key enzyme for nucleotide synthesis. It is involved in the salvage pathway of DNA synthesis and is activated in the G1/S phase of the cell cycle. Therefore, its activity has been shown to correlate with the proliferative activity of tumor cells (3, 16-19). Measurement of serum TK activity has been applied mainly in hematological malignancies (3, 16-21). Recent studies have provided great information regarding the prognostic utility of TK1 in patients with chronic lymphocytic leukemia (CLL) and non-Hodgkin's lymphoma (NHL) (10, 22-26). It is shown to correlate with the prognosis of indolent and aggressive lymphoproliferative diseases.
Transformations evaluated by serum TK levels.
In this study, a new TK chemiluminescence immunoassay was used to assess serum TK1 levels in patients with various lymphoid neoplasms. Serum TK1 levels were compared to clinical and laboratory parameters and to overall survival. All patients' serum β2M levels were recorded and used as a surrogate marker for assessment. Furthermore, we tested if high TK1 levels are uniquely high in patients with transformation from an indolent to an aggressive lymphoid malignancy. For this reason, we compared the TK1 levels of the patients with transformation to the TK1 levels of patients with indolent disease and constitutional symptoms but with no transformation. This use of TK1 levels in clinical routine has never been before investigated and presents a major clinical value.
Patients and Methods
We included in the study patients with lymphoproliferative malignancies to whom we had serum samples at diagnosis and / or at follow-up, before the initiation of treatment. All patients were older than 18 years and were treated in the Hadassah Hebrew-University medical Center between the years 1997-2012. For reference levels, we obtained serum from 37 healthy controls. We reviewed the medical records of the patients for details of date of birth, gender, specific diagnosis (WHO classification) and date of diagnosis, date of death if occurred or date at last follow-up. We also recorded the stage of disease when the sample was taken. For CLL, we used the Rai staging system(27) and for all other malignancies we used the Ann Arbor staging system (28). We specifically marked if the sample was taken at the time of a clinical suspicion of disease transformation from an indolent to an aggressive disease and whether the suspicion was verified or deferred. The study was performed under the permission of Hadassah IRB committee.
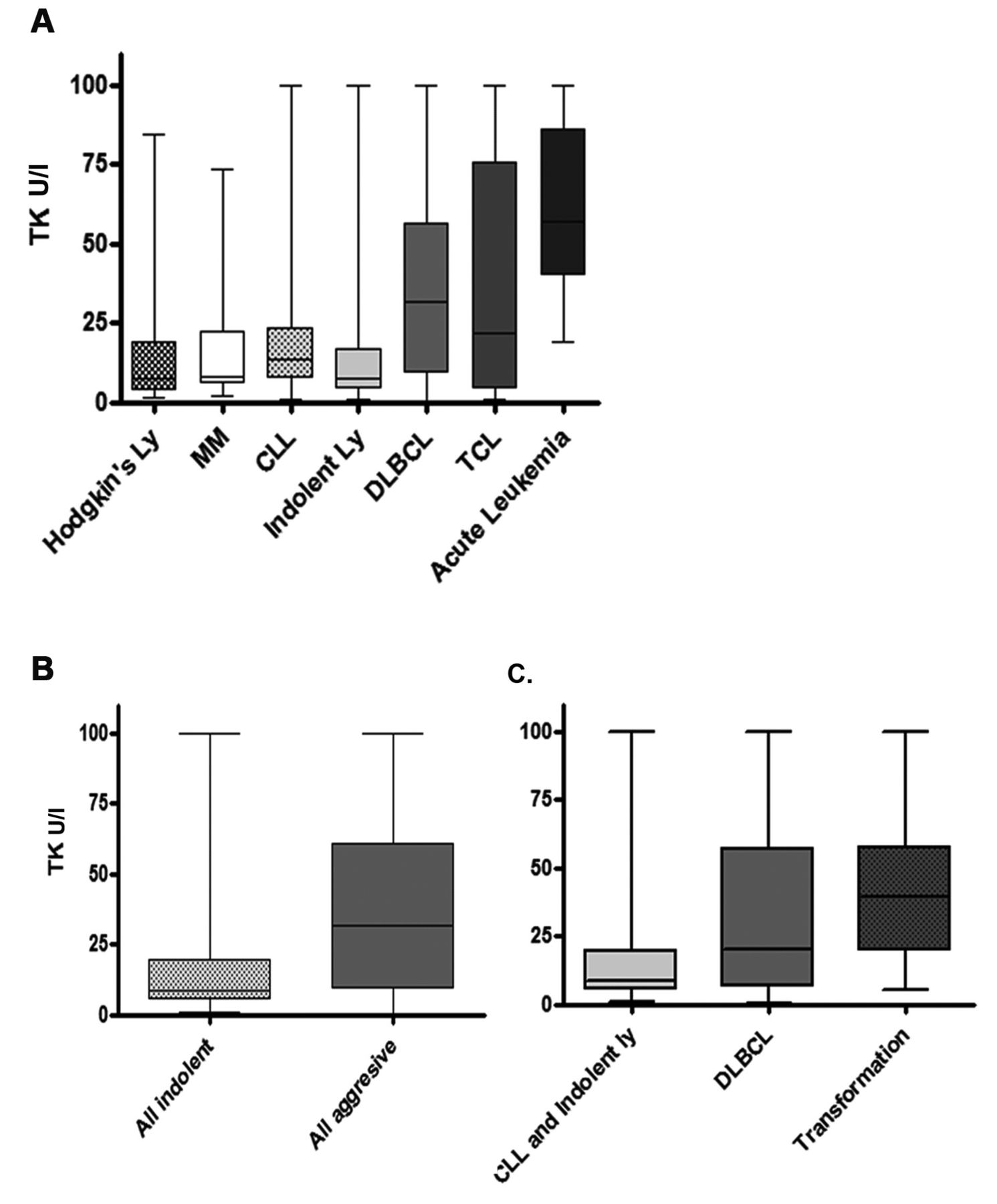
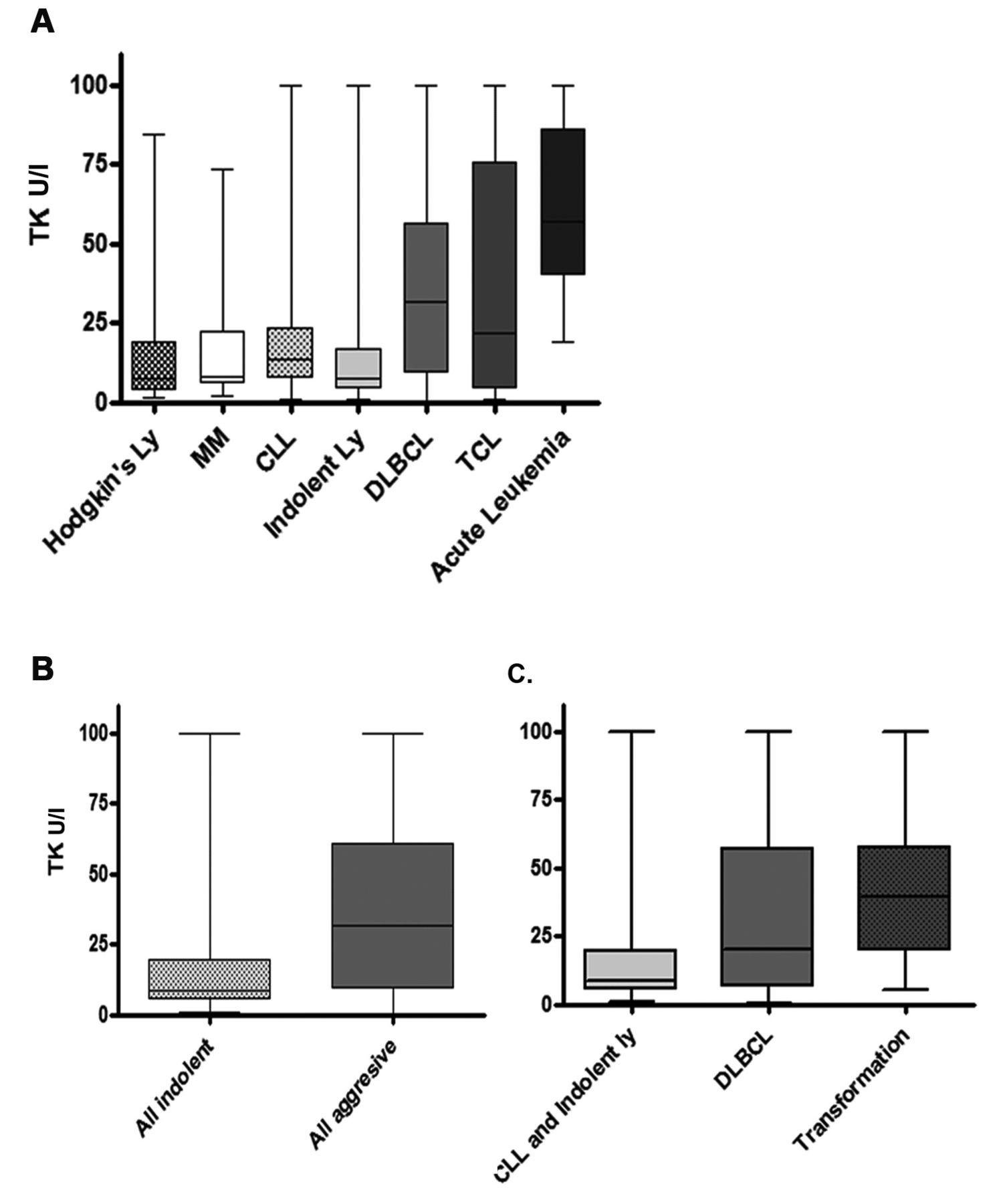
Serum TK levels at diagnosis of hematological malignancies. A. At diagnosis: all patients. B. At diagnosis: Indolent vs. Aggressive. C. At diagnosis: B cell lymphomas: Indolent vs. large B cell vs. transformed from indolent to aggressive.
Evaluation of TK and β2M serum levels. Analyzed serum was thawed and kept at 20°C. We used the Thymidine Kinase and β2M chemiluminescence immunoassay LIASION (DiaSorin, Stillwater, MN, USA) as previously described(11) and followed the manufacturer's instructions (29).
Statistical analysis. Statistical analysis was performed using the SPSS software, version 21.0 (IBM Corp, Armonk, NY, USA) and Graphpad prism 4 software (La Jolla, CA, USA). Categorical data were compared between groups by means of the Fisher's exact test in the case of dichotomous variables and χ2 test for two categorical variables. For significant results, a multivariate model of logistic regression analysis was used and hazard ratio (HR) with 95% confidence intervals (CI) calculated. Overall survival (OS) was calculated from the date of diagnosis of the disease until death or last follow-up. The Kaplan–Meier survival curves were performed for different groups of patients with multivariate analysis using the Cox regression model to assess the survival of patients. Determination of a p-value ≤0.05 was considered as statistically significant.

Survival analysis of indolent and aggressive diseases in correlation to serum TK levels. A. All patients. B. Indolent (TK level cutoff of 16.6 U/l). C. Aggressive (TK level cutoff of 16.6 U/l).
Results
Patients' characteristics. Table I lists the characteristics of the patients from whom the samples were taken at the time of diagnosis or follow-up. There were 75 patients with DLBCL, 36 patients with indolent lymphoma (14 FL, 13 MZL, 3 hairy cell leukemia and 3 lymphoplasmacytic lymphoma), 23 patients with CLL, 20 patients with HL, 13 patients with MM, 9 patients with T-cell lymphoma and 6 patients with acute lymphoblastic leukemia (ALL).
Table II details the characteristics of the 65 patients from whom the samples were taken at the time of clinical suspicion of disease transformation. Histological evidence of transformation was found in 31 patients (12 patients with CLL and 19 patients with other lymphoid malignancies). The most common diagnosis at transformation was DLBCL in 27 patients, followed by HL in 3 and TCL in 1 patient. In all others cases, the clinical suspicion was deferred and another cause for the symptoms was found: 22 had indolent disease-related symptoms, 11 had infection and 1 had drug fever.
For 5 patients with disease transformation, we had serum samples from the time of diagnosis of the indolent disease, as well as from the time of transformation (3 IL, 2 CLL).
Measurements of TK1 levels in controls and in patients with lymphoid malignancies. Considering the relatively new use of the TK1 levels measurement method by ELISA, we first verified its values in normal subjects. Thirty seven subjects, male and female adults were tested. The mean reading revealed normal levels to be 4.06 U/l+/-1.83. We, therefore, set the upper limits of normal to be 7.7 U/l (average+2 standard deviations). These results are comparable to those reported in normal subjects showing levels of 5.1 U/l (CI=1.9-6.9U/l) (29).
The TK levels of patients with lymphoid malignancies at diagnosis or at follow-up are plotted in Figure 1A. Overall, the TK1 levels were lower in 56 patients with indolent disease compared to 98 patients with an aggressive disease (Figure 1B, 18.9±3.3 and 39.8±3.3 U/l, respectively, p<0.001). Figure 1C demonstrates that the average TK1 levels in patients with transformed lymphoid malignancies was higher than in patients with indolent disease (p<0.001) or with de novo aggressive disease (p=0.09).
We further evaluated separately the 23 patients with CLL, since the WBC value in these patients previously correlated with TK1 levels. We found that, indeed, high WBC counts correlated with high TK1 levels (R=0.69, p=0.0002) but not the β2M levels; R=0.18 (p=0.4).
Overall survival (OS) analysis according to histology and to TK1 levels. In Figure 2A, we plotted the OS of patients with indolent (n=28) and aggressive (n=44) disease. Overall, patients with aggressive disease had a worse outcome (p=0.008).
In Figures 2A and 2B, we plotted the OS according to TK1 levels. We used a TK1 value of 16.6 U/l as a cut-off to define high/low TK1 levels as it represents the top 75 percentile of TK1 levels for indolent lymphoproliferative diseases. It is also roughly twice the upper limit of normal. We found that TK1 levels did not correlate with survival in patients with indolent lymphoma (Figure 2B). However, for patients with aggressive lymphoma, high TK1 levels correlated with worse outcome (p<0.008).
Evaluation of β2M levels in patients with lymphoid malignancies. For patients with CLL, the β2M levels did not correlate with WBC count. When measuring β2M levels with a cut-off of 2,000 U/l, we found them to be predictive of OS in both indolent and aggressive diseases.
Disease baseline characteristics.
Multivariate analysis for prediction of suspected transformation.
Utilization of TK level measurements for the diagnosis of transformation, from an indolent to an aggressive disease. Table III details the clinical features and important laboratory tests that were run on patients with suspected transformation. The only clinical and laboratory parameters, which differed significantly between patients with or without proven transformation, are the presence of B symptoms other than fever, high LDH levels and high TK1 levels.
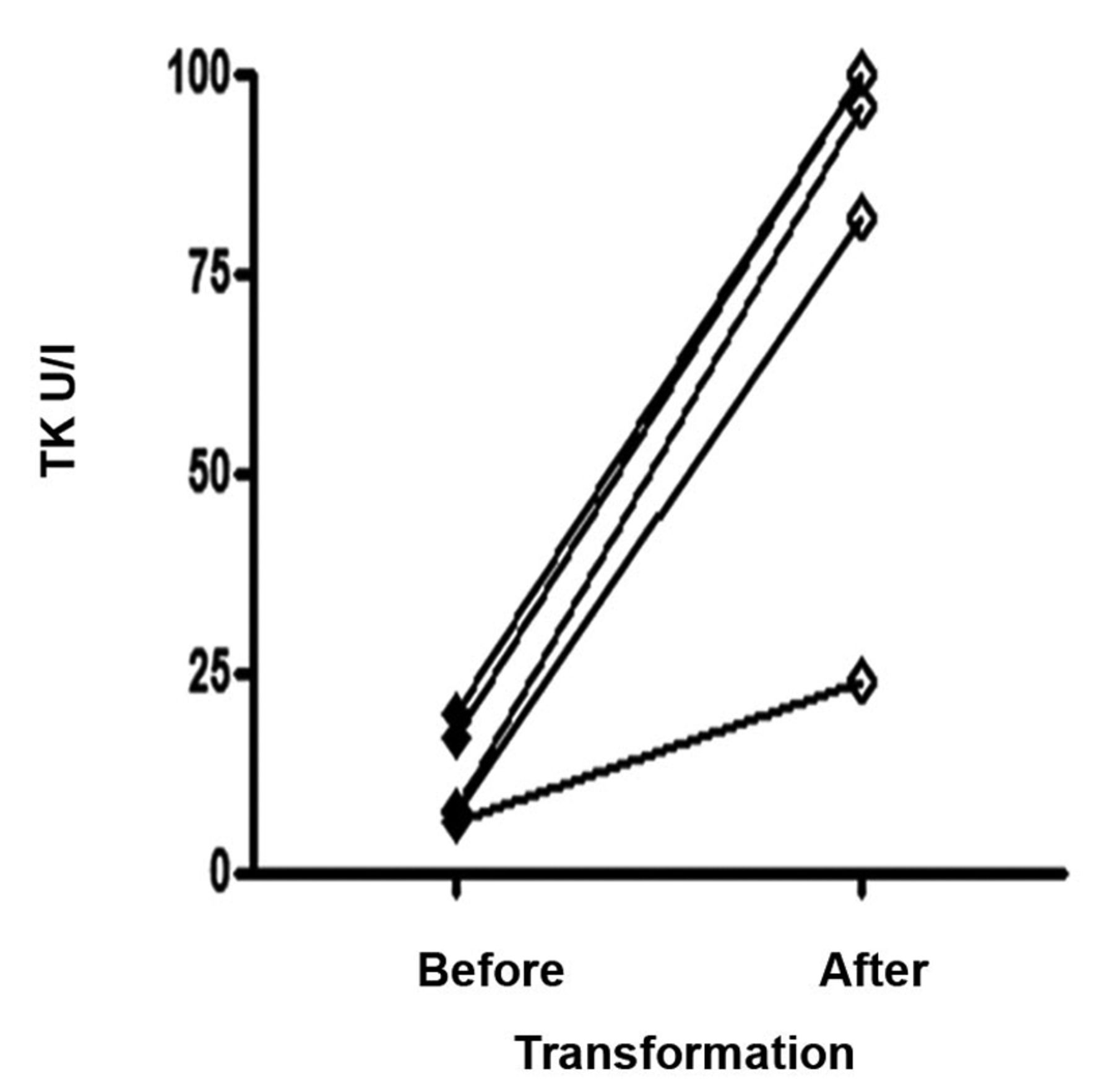
Change in serum TK levels in the same patients between time of indolent lymphoma diagnosis to aggressive transformation.
Part of post-diagnosis assessment (i.e. by biopsy or positron emission tomography-computed tomography (PET-CT) staging) was performed for some of the patients. As expected in aggressive disease, the median percentage of immunohistochemistry for Ki67 proliferation marker was 7.6% (1-19) (N=34) and 41% (26-100) (N=26) for the non-transformed vs. transformed patients, respectively (p=0.01). The median standardized uptake value (SUV) PET was similarly elevated 9.4 (4-13) (N=8) vs. 18 (6-30) (N=15) in the two groups, respectively (p=0.04). Using the cut-off TK level of >16.6 U/l, as determined previously, patients had a sensitivity of 95% and a specificity of 76% for a low to aggressive lymphoma transformation compared to those without transformation. This is further emphasized with a negative predictive value of 96% and a positive predictive value of 69%, respectively. Notably, as the specificity was not as marked as the sensitivity, we reviewed the clinical characteristics of the indolent-untransformed patients with above than 16.6 U/l TK levels. Interestingly, we found that these patients had a bulky disease >7 cm and were actually treated with chemotherapy regimens (data not shown), more commonly used in aggressive lymphoma patients.
In 5 patients who had proven transformation, we could check the TK1 levels at baseline (when they presented with indolent lymphoid malignancy, 3 with IL and 2 with CLL) and at the time of transformation. The mean TK1 level was 11.7+2.8 U/l at baseline and 80.2+11.5 at transformation (Figure 3, p=0.001).
In the univariate analysis “other B-symptoms”, LDH and TK levels proved significantly different between the two groups. However, in a multivariate analysis (Table IV), excluding Ki-67 and PET avid SUV (which are hallmarks of aggressive diseases), only TK1 levels proved to be important for the diagnosis of transformation to an aggressive disease.

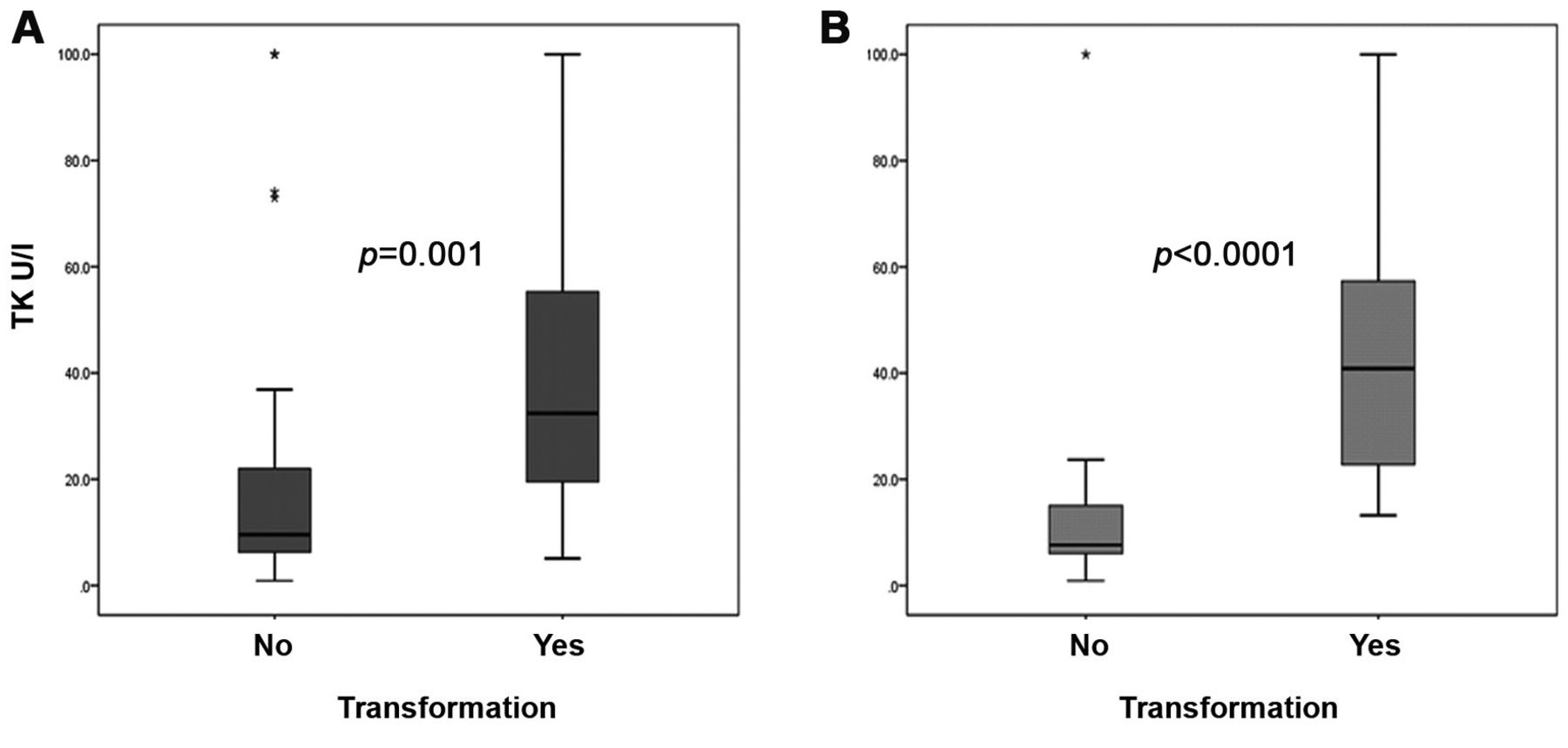
Comparison of serum TK levels between indolent disease patients suspected for transformation and proven transformed to aggressive lymphoma patients. A. All patients. B. Excluding patients with in situ/stage 1 disease.
As shown further (Figure 4A), the true-transformed patients had a marked increase, as hypothesized, of TK levels compared to the indolent-only patients (p=0.001), respectively. Albeit this significance, dissecting the clinical data of patients, we found a small group of true-transformed patients with very low, almost normal TK levels. These patients had a minimal load of aggressive disease (i.e. Ann-Arbor stage 1, in situ transformation within a lymph node or isolated CNS transformation). After censoring for these five patients with limited-stage localized transformations, differences became remarkably apparent (p<0.0001), with a median level of 7.6 versus 48.6 U/l, respectively (Figure 4b).
Discussion
TK1 serum levels were previously shown to correlate with the prognosis of CLL and NHL patients (6-8, 10, 12, 19-21, 23, 25, 26). The lymphoid malignancies are a heterogenic group of diseases with either an indolent or an aggressive course. The role of serum TK1 levels as a prognostic factor in the indolent lymphoma, including CLL, is well established and has been validated (29, 30). However, there is little data on the role of TK1 serum levels for the risk stratification of aggressive lymphoma, specifically DLBCL (31). Moreover, there are no published data of the TK1 levels in the state of transformation of an indolent to an aggressive lymphoid malignancy.
In this study, we included 59 patients with indolent lymphoma and CLL, 44 patients with aggressive lymphoid malignancy and 31 with transformed indolent to aggressive lymphoid malignancy. The TK1 level in these patients was able to correlate with a dismal prognosis when elevated, yet only in the subset of aggressive lymphoma patients. This may be attributed to the generally good prognosis of indolent lymphoma patients where survival differences are more difficult to show. For the purpose of this analysis we used a cut-off of 16.6 U/l, which was the upper limit quartile in the indolent diseases. These levels are similar to cut-offs used for prognostication (14-16 U/l) by most recent reports (22-26), showing TK's predictive ability and are roughly twice the upper limit of normal levels. Herein, aggressive lymphoma patients were discriminated significantly by their survival. Being a proliferative marker, it thus can be used as an adjunct to the traditional prognostic systems and markers for the purpose of prognosis assessment. This finding is in line to what has been reported in NHL patients, FL (24), DLBCL (6, 26) and TCL (25), where levels also correlated with disease stage. TK1 levels were most well characterized in CLL and found to correlate with prognosis and stage (8, 10, 12, 22). Indeed, we found TK levels to well correlate with WBC counts; however, we did not further investigate its role in CLL.
Given these important findings, we further hypothesized that high serum levels of TK will be able to discriminate patients with a proven transformation from indolent to aggressive lymphoma in the context of a clinical suspicion. Although transformations are relatively rare, the diagnosis of transformation is of major importance since it dictates the therapeutic approach. Clinical parameters, such as high LDH serum levels, high Ki67 in a biopsy and high SUV in a PET-CT have been all previously suggested in aiding the physician debating if a transformation has occurred. We, thus, tested these parameters, as well as the TK1 levels, in our patients with transformation and compared the values found to the values in patients with suspected transformation based on the clinical presentation having, eventually, a different diagnosis. Most patients in the no-transformation group had the same occurrence of a bulky mass or constitutional symptom as the group with an aggressive transformation and matched for baseline characteristics. Indeed, we were able to show that TK1 levels differed significantly between the two groups. Using the cutoff TK level of >16.6 U/l, as determined previously, had a sensitivity of 95% and a specificity of 76% for a low- to-aggressive lymphoma transformation patients compared to patients without a transformation. This is further emphasized with a negative predictive value of 96% and a positive predictive value of 69%, respectively. In contrast, we measured the serum β2M levels, which are a well-established serum marker for disease prognosis assessment and progression (4-7, 9) and, although we show it had a prognostic long-term significance in indolent and aggressive diseases, it could not discriminate between the transformed and non-transformed clinically suspected patients. By a logistic regression analysis, only TK1 levels were an independent marker for transformation. Our finding suggests that in the relatively common clinical scenario of an indolent patient investigated for non-specific constitutional symptom or a bulky disease and a transformation from low-to-aggressive lymphoma is suspected, if the serum TK levels are lower than 16.6 U/l, it is unlikely that the patient harbors such a transformation. We do not propose to substitute TK1 level measurements with a conclusive biopsy. However, such a measurement may aid in the decision process of how insistent and intensive a workup for the clinical scenario should be. The only report previously assembling a parallel comparison of patients did not show a significant difference in TK levels between groups of transformed and non-transformed CLL patients (32). However, this was not performed in the clinical context of a suspected transformation and the cutoff used is not validated. Of note that the transformed group consisted of only 16 patients and the control group had a significantly higher percentage of patients in advanced stages.
In summary, serum TK levels are useful in assessing prognosis, especially in aggressive lymphomas. Moreover, TK levels are able to discriminate indolent patients suspected of an aggressive transformation, but eventually having none, from patients with proven transformations. This tool provides the clinician a novel method to distinguish between symptomatic patients utilizing a simple test and may lessen the need for aggressive or invasive measures of investigation.
Footnotes
-
↵* These authors have equally contributed in this study.
- Received February 8, 2015.
- Revision received February 20, 2015.
- Accepted February 24, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}