


Abstract
Testing for somatic alterations, including anaplastic lymphoma receptor tyrosine kinase gene (ALK) rearrangements and epidermal growth factor receptor gene (EGFR) mutations, is standard practice in the diagnostic evaluation and therapeutic management of non-small cell lung cancer (NSCLC), where the results of such tests can predict response to targeted-therapy. ALK rearrangements, EGFR mutations and mutations in the Kirsten rat sarcoma viral oncogene homolog (KRAS) are considered mutually exclusive in NSCLC. Herein we identified a KRAS Q22K mutation and frameshift mutations in the genes encoding serine/threonine kinase 11 (STK11) and ataxia telangiectasia mutated serine/threonine kinase (ATM) by next-generation sequencing in a patient with ALK rearrangement-positive oligo-metastatic NSCLC, whose disease progressed while on two ALK-targeted therapies. Such a complex diagnostic genetic profile has not been reported in ALK fusion-positive NSCLC. This case highlights the utility of comprehensive molecular testing in the diagnosis of NSCLC.
- Non-small cell lung cancer
- ALK translocation
- ALK inhibitor
- KRAS
- STK11
- ATM
- crizotinib resistance
- genomics
- next-generation sequencing
- case report
Lung cancer is the leading cause of cancer-related mortality both in the United States and worldwide (1). Non-small cell lung cancer (NSCLC) accounts for the majority of these cases, with the main histological subtypes being adenocarcinoma and squamous cell carcinoma (2). Over the past decade, several oncological drivers of NSCLC have been identified, leading to development of targeted-therapies and determination of prognostic and predictive molecular subsets (3). These advancements have led to the integration of several molecular investigations into the routine diagnostic evaluation of advanced NSCLC, including thereputic targets, such as, epidermal growth factor receptor (EGFR), anaplastic lymphoma kinase (ALK) (4), c-ros oncogene 1 (ROS1), and B-Raf proto-oncogene (BRAF) (5).
EGFR gain-of-function mutations are seen in approximately 10-15% of patients with NSCLC, the majority of which are found in exons 19 and 21. Patients whose tumors harbor activating EGFR mutations are most commonly never-smokers, women, Asians and patients with adenocarcinoma. These mutations predict response to small-molecule tyrosine kinase inhibitors (TKIs), including gefitinib, erlotinib and afatinib, and are commonly evaluated by DNA-based molecular assays (6-8).
ALK gene fusions, most commonly partnered with Echinoderm microtubule-associated protein-like 4 (EML4), create a fusion protein with potent oncological potential. ALK gene rearrangements are more commonly seen in younger patients, and, similarly to EGFR mutations, are enriched in those with adenocarcinomas and light or never-smokers. ALK fusions are seen in 2-7% of NSCLC and show dramatic responses to crizotinib, a small molecular inhibitor of ALK and MET proto-oncogene (MET) receptor kinases (9-11). ALK fusions are most commonly evaluated by fluorescence in situ hybridization (FISH) assays, although molecular assays using next-generation sequencing (NGS) are emerging.
Another oncogenic driver of NSCLC is KRAS mutation, seen in approximately one-third of cases, the majority of which are current or former smokers. These mutations are most commonly single nucleotide substitutions at codons 12, 13 and 61. Unlike EGFR and ALK alterations, the prognostic and predictive value of KRAS mutations are less clear, and no proven targeted-therapies yet exist (12-14). However, some molecular laboratories will take advantage of the fact that EGFR, ALK and KRAS genetic alterations are considered mutually exclusive driver mutations (15, 16), by including KRAS mutation profiling as part of an algorithmic approach to tiered testing (4).
Pathogenic somatic mutations discovered by next-generation sequencing panel.
Herein we present a unique patient with a known ALK gene rearrangement whose tumor underwent NGS after failed crizitonib therapy and lack of response to an investigational ALK inhibitor, AP26113, on a clinical trial. A KRAS Q22K mutation, as well as frameshift mutations involving the ataxia telangiectasia mutated serine/threonine kinase gene (ATM) and serine/threonine kinase 11 (STK11), were discovered, which may have accounted for the patient's dismal response to ALK-targeted therapy and highlights the utility of comprehensive testing of NSCLC specimens.
Case Report
The patient is a 65-year-old male former smoker (15-pack-year history), quitting approximately 10 years prior to diagnosis with oligo-metastatic NSCLC, adenocarcinoma subtype (T2aN2M1). He presented two years ago with progressive loss of visual acuity of the left eye, which was initially believed to be secondary to cataract formation. The patient subsequently developed rapid visual loss, which prompted an urgent ophthalmologic examination that demonstrated a lesion on the left choroid. He underwent needle biopsy of the lesion, which revealed evidence of metastatic carcinoma (probably adenocarcinoma) consistent with a lung primary and received brachytherapy for the metastatic lesion.
As part of the diagnostic work-up, a computed tomography (CT) scan of the chest showed a 4.2-cm mass in the left upper lobe (LUL) and a 2-cm lymph node in the aortopulmonary window, both of which were hypermetabolic on positron emission tomography-CT imaging. The patient underwent a lobectomy of LUL; pathology revealed a 4.5-cm grade II adenocarcinoma (Figure 1), metastatic to several mediastinal lymph nodes (levels 5, 6 and 12). The patient was treated with four cycles of adjuvant cisplatin/pemetrexed and laser surgery for a left choroid recurrence, and subsequently had no measurable disease. The lobectomy specimen was sent for outside testing for EGFR exon 19 and 21 mutations, ALK fusion rearrangement and KRAS codon 12/13 mutation analyses; the specimen was reported as ALK fusion-positive.
Approximately nine months after diagnosis, the patient developed metastatic disease and was started on crizotinib. This treatment was discontinued after three months due to disease progression (metastasis to the right parietal lobe). The patient received multiple therapies, including a right parietal craniotomy, laser treatment of a lesion of the right eye, and systemic therapy with paclitaxel, carboplatin and bevacizumab. He was continued on maintenance bevacizumab but had disease progression after three cycles. The patient was then treated on a clinical trial with an investigational ALK inhibitor, AP26113. This treatment was stopped after two cycles due to disease progression.
This perplexing lack of response to both crizotinib and AP26113 prompted an in-house repeat of the ALK assay and a request for NGS solid tumor panel testing on the specimen metastatic to the parietal lobe.
DNA was obtained from a formalin-fixed paraffin-embedded (FFPE) biopsy of a right parietal lobe metastasis. Percentage tumor estimates from pathological review were greater than 25%. Targeted genomic regions were enriched across 47 genes using the Illumina TruSeq Cancer panel and subsequently sequenced on a Miseq with paired end 2 by 185 base pair reads to an average read depth of 4300x (Illumina Inc., San Diego, CA, USA). Using an in-house analysis pipeline, variants in the exonic regions and intron/exon boundaries were detected.
For FISH evaluation, 5-micron sections of FFPE tumor tissue were prepared and an H&E section reviewed to select regions of hybridization that contain a majority of tumor cells. LSI ALK (2p23) Dual-Color Break-Apart Rearrangement probe (Vysis Inc., Abbott Molecular, Abbott Park, IL, USA) was hybridized and used to calculate the number of cells out of 100 scored containing the rearrangement. An ALK rearrangement is reported if more than 15% of cells show split signals or 10% loss of the 5’ALK signal.
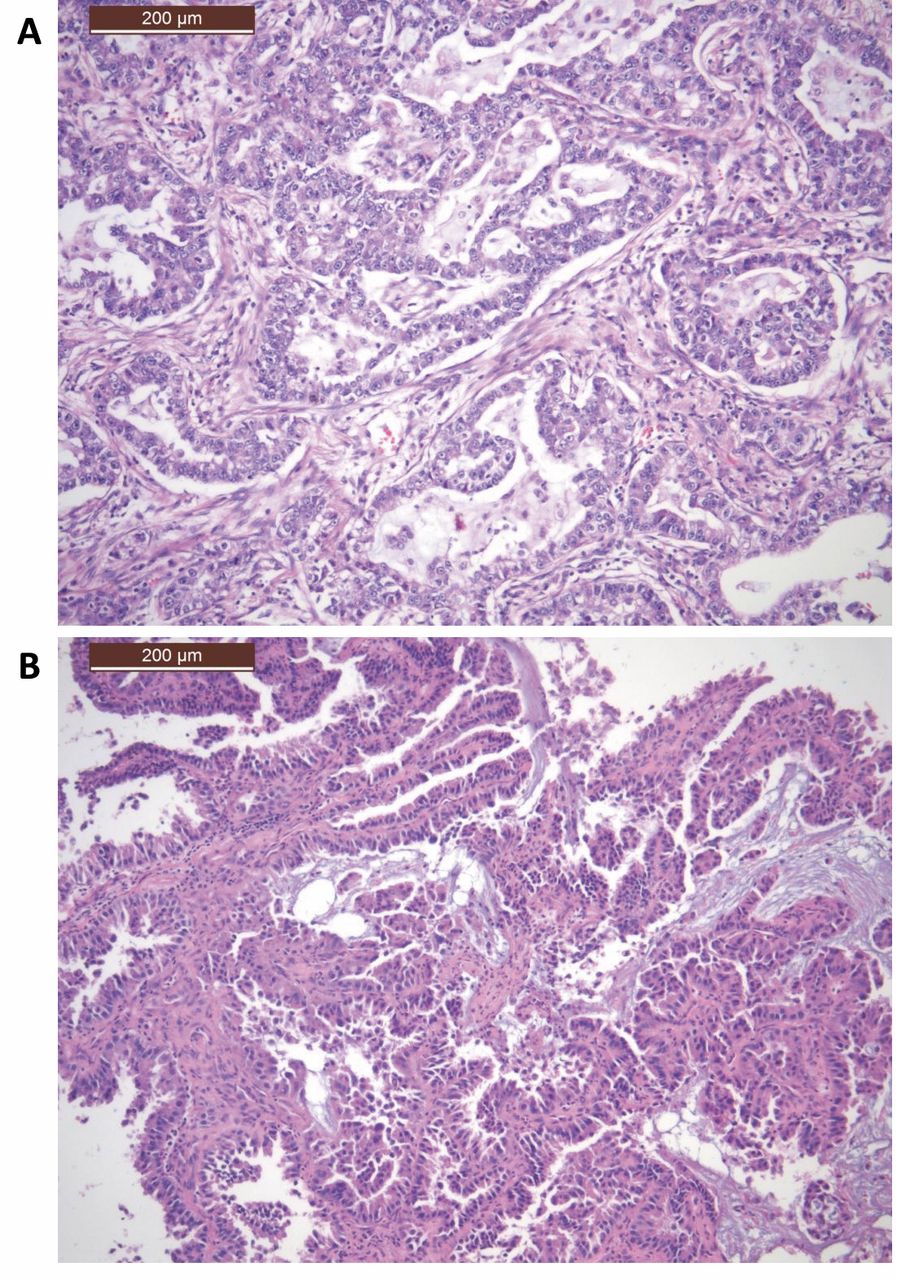
Representative histology (×10) from the diagnostic and metastatic tumor specimens. A: The diagnostic specimen from the left upper lobe lobectomy showing moderately differentiated adenocarcinoma. B: The parietal lobe specimen showing metastatic adenocarcinoma consistent with the lung primary.
The FISH assay was positive for an ALK rearrangement in 70/100 cells (70%) (Figure 2). NGS results revealed a frameshift deletion in ATM, a missense mutation in KRAS (amino acid residue 22) and a frameshift insertion in STK11 (Table I). Due to the patient's history of a poor response to crizotinib and because this unique genomic profile had not been previously reported, we repeated the NGS solid tumor panel testing on the original ALK fusion-positive LUL lobectomy specimen. The same alterations in ATM, KRAS and STK11 were observed at similar allelic frequencies (~25%).
Discussion
We present a case of ALK inhibitor-resistant ALK rearrangement-positive NSCLC with concurrent KRAS Q22K mutation and frameshift mutations in ATM and STK11. To our knowledge, this is the first report of such a complex pattern of genetic alteration in ALK fusion-positive NSCLC at diagnosis. ALK rearrangements in NSCLC are considered mutually exclusive of EGFR and KRAS mutations; however, most studies to date have only evaluated KRAS codons 12, 13 and 61 (16-18). KRAS Q22K has been reported in a variety of tumor types, most commonly colonic cancer (19-25). This activating mutation has been shown to transform NIH-3T3 fibroblasts (26). Functional studies with the Q22R mutant, which is physiologically homologous to the Q22K alteration, suggest that this mutation may confer a milder gain-of-function phenotype than the hot-spot mutations at positions G12, G13 or Q61 (27).

Fluorescence in situ hybridization assay using the Vysis LSI anaplastic lymphoma receptor tyrosine kinase gene (ALK) Dual Color, Break Apart Rearrangement probe (Abbott Molecular, Abbott Park, IL, USA). Two probes flanking the breakpoint of the ALK gene are labeled with orange and green fluorophores, adjacent to the 3’ and 5’ ends, respectively. Normal ALK exhibits adjacent or fused orange and green signals, which may appear as a yellow signal. Rearranged ALK results in split orange and green signals, or single orange signal(s). The cell shown contains two intact copies of ALK and a single orange signal, corresponding to an ALK rearrangement followed by 5’ALK deletion.
STK11, also known as LKB1, is a tumor-suppressor gene that encodes for a protein with serine-threonine kinase activity. Inactivation mutations of STK11, or loss of chromosome 19 where the gene resides, occur in a large proportion of primary lung adenocarcinomas; most somatic mutations are frameshift or nonsense mutations that lead to a truncated protein and tend to co-occur with mutations at other genes important in carcinogenesis, such as KRAS or tumor protein p53 (TP53) (28-30). Mutations in STK11 appear to play an important role in tumor differentiation and metastasis in lung cancer (31). ATM also acts as a tumor suppressor, encoding a cell-cycle checkpoint kinase that regulates p53. Somatic loss-of-function mutations are seen in fewer than 10% of NSCLC cases (32,33).
As the patient progressed quickly on crizotinib, it was hypothesized that some or all the mutations found in the metastatic parietal lobe specimen may have been present in the initial ALK fusion-positive tumor specimen from the lobectomy of the LUL; subsequent confirmation by NGS testing revealed that the same alterations in ATM, KRAS and STK11 were present at diagnosis. As all three mutations were at the same relative allelic frequency (~25%), which correlates well with the percentage tumor estimation, it is likely that these mutations were co-occurring in the same clone. As the patient was initially resistant to crizitonib, it is quite possible that some, if not all, of these alterations may have played a role in the lack of therapy efficacy. Activation of alternative signaling pathways is a mechanism of acquired resistance to crizotinib; the role of developed secondary mutations in KRAS is currently less clear, with conflicting results from rare case reports (34-37). As only limited hotspot analyses of KRAS have been performed in most analyses of ALK rearrangement or EGFR mutation-positive NSCLC, it is possible that a subset of these have less common yet relevant alterations in KRAS (or other genes), which may possibly affect therapy efficacy. This case provides an example of the utility of comprehensive molecular testing in cases of NSCLC and the need for additional research in this area. These described mutations have not been reported together before; this may represent a unique, rare event, or, as tumor sequencing expands in the clinic, similar findings may be seen with some frequency. Ultimately, in the future, knowledge of complex tumor profiles will undoubtedly guide increasingly precise and multi-pronged approaches to therapy.
- Received February 15, 2015.
- Revision received March 1, 2015.
- Accepted March 3, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.