


Abstract
Aim: The present study aimed to investigate the implications of using the analytical anisotropic algorithm (AAA) for calculation of target coverage and radiation burden of normal tissues. Most model parameters, recommendations and planning guidelines associated with a certain outcome are from the era of pencil beam convolution (PBC) calculations on relatively simple assumptions of energy transport in media. Their relevance for AAA calculations that predict more realistic dose distributions needs to be evaluated. Patients and Methods: Forty patients with left-sided breast cancer receiving 3D conformal radiation therapy were planned using PBC with a standard protocol with 50 Gy in 25 fractions according to existing re-commendations. The plans were subsequently recalculated with the AAA and relevant dose parameters were determined and compared to their PBC equivalents. Results: The majority of the AAA-based plans had a significantly worse coverage of the planning target volume and also a higher maximum dose in hotspots near sensitive structures, suggesting that these criteria could be relaxed for AAA-calculated plans. Furthermore, the AAA predicts higher volumes of the ipsilateral lung will receive doses below 25 Gy and smaller volume doses above 25 Gy. These results indicate that lung tolerance criteria might also have to be relaxed for AAA planning in order to maintain the level of normal tissue toxicity. The AAA also predicts lower doses to the heart, thus indicating that this organ might be more sensitive to radiation than thought from PBC-based calculations. Conclusion: The AAA should be preferred over the PBC algorithm for breast cancer radiotherapy as it gives more realistic dose distributions. Guidelines for plan acceptance might have to be re-evaluated to account for differences in dose predictions in order to maintain the current levels of control and complication rates. The results also suggest an increased radiosensitivity of the heart, thus indicating that a revision of the current models for cardiovascular complications may be needed.
- Breast radiotherapy
- dose calculation algorithm
- analytical anisotropic algorithm
- pencil beam convolution
- planning guidelines
Adjuvant radiotherapy is a major treatment modality used in the management of breast cancer to achieve long-term control of local and regional disease and to increase overall survival (1). The quality of the results nevertheless depends on the ability to deliver the prescribed dose to the target volume, with acceptable radiation burden to normal tissues at risk. Equally important is the capacity to homogeneously deliver the dose, especially for patients with multifocal or lobular disease, and to reproduce the relevant dosimetric parameters in individual patients and between treatment Centres. All these depend not only on the irradiation technique used, but also on the accuracy of dose calculations for the target and the normal tissues around it.
Several algorithms are available for treatment planning systems to calculate dose distributions in patients based on various assumptions for radiation transport (2). The pencil beam convolution (PBC) algorithm and the anisotropic analytical algorithm (AAA) are the most widespread algorithms used by the Eclipse treatment planning system (Varian, Palo Alto, CA, USA). The PBC algorithm calculates the dose as a convolution of the radiation field fluence with the dose deposition kernel of a narrow photon pencil beam in water, using a modified Batho method to make corrections for heterogeneities along fan lines (3-5). In contrast, the AAA separately models the contributions of primary photons, extra-focal photons and contaminating electrons, and better takes into account the lateral energy transport (6). Consequently, the AAA provides improved accuracy, especially for calculations in heterogeneous media (2, 7, 8) and would, therefore, be better-suited for dose calculations for treatments of the breast where the anatomy of the patient is a heterogeneous mixture of tissues. Several studies have investigated the dosimetric predictions of the two calculation algorithms for breast radiotherapy and have found significant differences (2, 9). However, the AAA has slowly been adopted for clinical practice slowly, mainly because clinical knowledge and the clinical guidelines for plan acceptance come largely from the era of PBC calculations. Furthermore, the Quantitative Analysis of Normal Tissue Effects in the Clinic (QUANTEC) proposed tolerance levels for the lung (10) and parameters of radiobiological models for the heart (11) are also based on analyses of data from before the routine clinical adoption of the AAA or other convolution-superposition algorithms. Consequently, the direct use of PBC-based criteria and parameters for the evaluation of AAA plans would generate unnecessary uncertainties given the differences in predictions of the two mentioned algorithms. Therefore, it was the aim of this project to investigate the implications of using the AAA for planning calculations from the perspective of clinically relevant parameters for models and recommendations.

Axial section showing the dose distributions calculated with pencil beam convolution (left panels) and the analytical anisotropic algorithm (right panels) for one breast and supraclavicular lymph nodes patient included in the analysis.
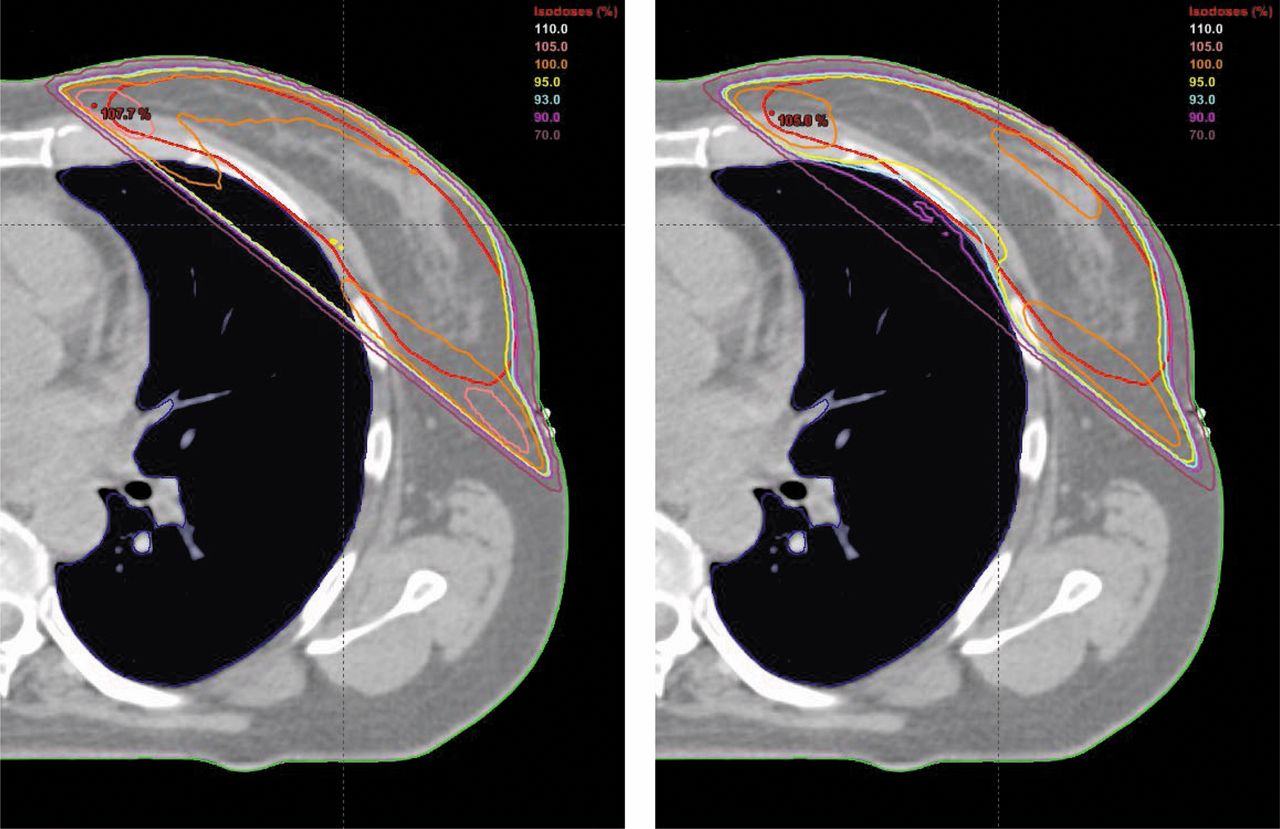
Axial section showing the dose distributions calculated with pencil beam convolution (left panel) and the analytical anisotropic algorithm (right panel) for a whole-breast-only patient included in the analysis.
Patients and Methods
Twenty consecutive patients with left-sided breast cancer receiving treatment to the breast and the supraclavicular lymph nodes (BSC) and 20 patients receiving treatment only to the whole breast (WBO) were planned according to routine practice with PBC in Eclipse TPS (version 10). Preference was given to patients with left-sided breast cancer to investigate the impact of calculations for the irradiation of the heart as an organ-at-risk, an aspect not covered by previous studies.
All patients underwent computed tomographic (CT) scanning for treatment planning with 2 mm slice thickness. The location of the tumour with suitable margins (CTV-T), planning target volume (PTV) and volumes of the ipsilateral lung and the heart as organs at risk were delineated and reviewed by experienced radiation oncologists. Treatment plans were devised with tangential fields and anteroposterior fields for BSC patients, and with tangential fields for WBO patients. A monoisocentric technique was used for BSC patients, with the isocentre placed at the junction between the breast and the supraclavicular region. Energy, dynamic wedges and compensating fields were used as needed. The plans were normalised so that the mean dose to the PTV was equal to 50 Gy in 25 fractions and evaluated according to local practice. The plans were subsequently calculated with the AAA maintaining the same beam configuration and the same number of monitor units. This approach, also used in another study on the topic (12), ensures that dosimetric evaluation is performed on plans that are deemed acceptable according to existing guidelines.
The PBC- and AAA-calculated treatment plans were evaluated in terms of dose to the PTV and the organs at risk. Thus, PTV parameters included the volume receiving at least 93% of the
prescribed dose (V93%) and the International Commission on Radiation Units and Measurements (ICRU) recommended near minimum dose, D98% (the dose to 98% of the PTV), near maximum dose, D2% (dose to 2% of the PTV) and the heterogeneity index (HI) defined as:
 where D50% is the median dose to the PTV (13).
where D50% is the median dose to the PTV (13).
Mean values and standard deviations for the dosimetric parameters considered in the study.
For the organs at risk, clinically relevant parameters were also determined from the dose-volume histograms. These included mean and near maximum dose to the ipsilateral lung and the heart, as well as the volume of lung tissue receiving 10 Gy (V10 Gy) and that receiving 20 Gy (V20 Gy). These are dosimetric parameters used either as constraints in international and national recommendations, or as parameters for radiobiological models for normal complications (10, 14-16).
The statistical significance of the differences between the dose parameters in the plans from the two algorithms was evaluated with a paired, two-tailed Student's t-test.
Results
The AAA calculation of plans led to significant differences of the dose distributions in and near the PTV compared to the PBC-calculated plans, as shown by the data in Table I. Figures 1 and 2 illustrate the differences in dose distributions that could be expected from the two calculation algorithms considered for a BSC patient and for a WBO patient respectively. The most striking differences are for regions near lung-tissue interfaces, where the AAA better takes into account the lateral scatter of radiation leading to an increased concavity of the 90%-95% isodoses extending into the PTV. These also translate into differences of the predicted dose-volume histograms as illustrated in Figure 3.
The results in Table I show that the AAA-calculated plans had significantly different target coverage from the PBC-calculated plans, especially for BSC patients. Thus, V95% for CTV-T was lower for the AAA-calculated plans (p=0.03) and PTV had a significantly worse coverage with the 93% isodose (p<0.0001). These differences translate into increased dose heterogeneity for the AAA-calculated plans compared to PBC-calculated plans as illustrated by the HI. Furthermore, the analysis of individual plans showed that some AAA-calculated plans had higher maximum dose in hotspots sometimes near sensitive structures, such as the brachial plexus.
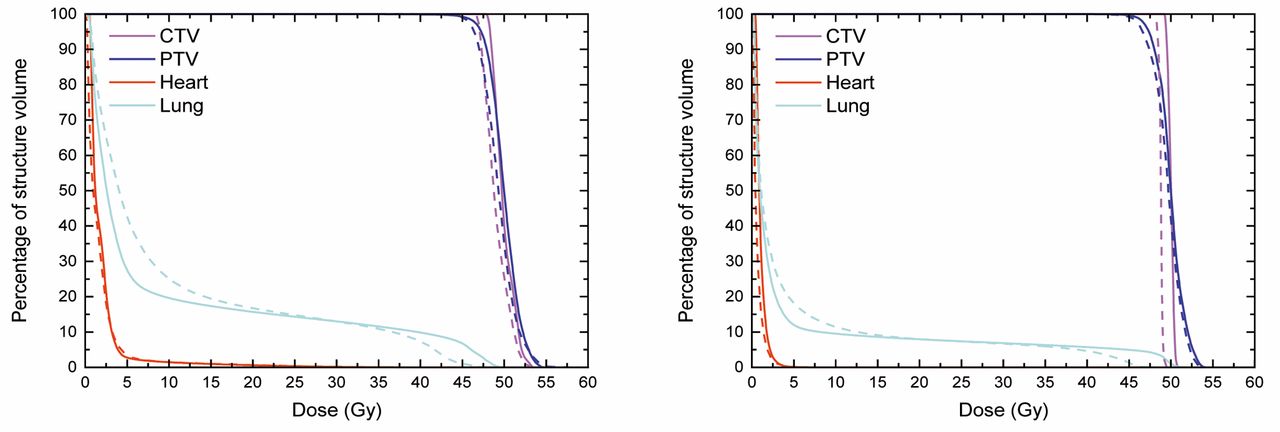
Dose-volume histograms for plans calculated with pencil beam convolution (solid curves) and from plans calculated with the analytical anisotropic algorithm (dashed curves) for the breast and supraclavicular lymph nodes patient (left panel) and for the whole breast only patient (right panel) in Figures 1 and 2.
With respect to the organs at risk, the AAA predicts that higher volumes of the ipsilateral lung receive doses below 25-30 Gy and smaller volumes receive doses above this level. While differences in V20 Gy predictions are rather small, the AAA predicts a significantly large increase in the volume of the lung irradiated with lower doses, as illustrated by the V10 Gy values. More importantly, the AAA also predicts mean doses to the heart to be significantly lower than from PBC-based calculations, indicating an increased radiation sensitivity for this organ.
Discussion
There is a large body of studies showing that the AAA and other convolution-superposition algorithms are better capable of predicting dose distributions in heterogeneous media than the PBC (8, 17-19). These would recommend the use of such algorithms for dose calculations in breast radiotherapy that often includes tangential irradiation of irregularly curved surfaces and inhomogeneous composition of the irradiated tissues with soft tissues, bone and lung tissue. However the clinical adoption of the AAA would require corresponding plan-acceptance guidelines to maintain the current standards-of-care, with high tumor control levels and acceptable complication rates. It was from the perspective of currently achievable standards of care that the present study was concerned with investigating the impact of using the AAA for dose calculations in the radiation treatment of breast cancer.
In the years since the introduction of the AAA, relatively few studies have investigated its impact in clinically relevant breast cases, most of them focusing on few tangential case studies that make the extrapolation of the findings quite difficult. Thus, Knöös et al. compared many calculation algorithms on a single breast cancer case, focusing on the differences in the PTV and the lung (2). Panettieri et al. also looked at one right-sided breast cancer case, finding significant differences in the buildup region of the individual fields (20). Basran et al. compared PBC- and AAA-based predictions against Monte Carlo simulations in 10 patients treated with tangential irradiation and reported no clinically significant changes in doses to the target and the normal tissues included in the analysis (lung, heart and normal breast tissue) (12). More recently, Yoo et al. used data from 20 patients receiving tangential irradiation to study the dosimetric differences between plans calculated with the AAA and PBC and reported significant differences between predictions of the two algorithms for the lung, skin and PTV, but without an analysis for the heart (9).
The present results add to these studies, reporting on the findings from an even larger group of 40 patients, including the irradiation of the supraclavicular nodal area, which has largely been neglected in previous studies, and adding analyses of the doses to the tumor site (CTV-T) and the heart. This latter aspect is extremely important as a recently published large case-control study by Darby and co-workers (21) showed that heart irradiation during breast cancer radiotherapy could increase the risk for major coronary events by 7.4% Gy-1, with no apparent threshold and with relatively early onset. Furthermore, the clinical implications of the AAA have been investigated from the perspective of currently used recommendations for plan and normal tissue evaluation (10, 14-16).
The results of the present study have thus shown that there are several significant differences between the predictions of the two calculation algorithms considered for this study and that these might impact upon the usage of the current evaluation criteria. Thus, while fewer than 10% of the PBC-based cases had difficulties covering the tumour site (CTV-T) with the 95% isodose, about 30% of the plans recalculated with the AAA had poorer CTV-T coverage. Keeping in mind that the AAA predicts closer-to-reality dose distributions, increasing tumour coverage in AAA-based plans will nevertheless account for an increase of the dose homogeneity to the tumour site and an improvement of the patient outcome above the current levels. Similar considerations also apply for the coverage of the PTV. Indeed, the AAA predicts both a decrease in the near-minimum dose and an increase of the near-maximum dose to the PTV, leading to a statistically significant increase of the HI.
Target coverage would also have to be balanced against the effects in normal tissues that might become a limiting factor for breast cancer treatments. Thus, our analysis has shown that the use of the AAA for dose calculations predicts significant differences in the dosimetric parameters for the lung. This is in line with the findings of many studies investigating the AAA, collapsed cone and other convolution-superposition algorithms (2, 9, 12, 22, 23). Furthermore, the AAA was found to predict 5% (range=1-11%) higher mean doses to the ipsilateral lung for BSC and 9% (range=2-21%) for WBO. These findings are similar to those of Aspradakis and colleagues (average 3% increase for collapsed cone vs. PBC) (22) and Yoo and colleagues (average 14% increase for AAA vs. PBC) for tangential breast irradiation (9), and also to the earlier reports of De Jaeger et al. of an average increase of 17% of the dose to the lung when a convolution-superposition algorithm is used instead of a simpler algorithm to calculate the doses from conformal radiotherapy of lung cancer (24). The results also indicate a different trend in BSC versus WBO patients, suggesting that extrapolation of findings from other studies is not straightforward. These results should be analyzed in light of the current recommendations regarding lung tissue response such as those of QUANTEC (10), which are based on analyses of data from before the introduction of the AAA and which favour the use of the mean lung dose to predict complication rates. Their clinical impact would also have to be considered in relation to the variations in clinical dose-response data which might depend on patient selection or the grade of side-effects reported (10). Consequently, care should be employed in extrapolating the findings of analyses of normal tissue complications for this organ and when modelling these complications, one would have to use parameters relevant for the algorithm employed for calculating dose distributions.
More important, however, is the increase in the predicted volume of the lung receiving low doses, which was similar for WBO and BSC patients at 24% (range=11-39%) and 21% (range 14-29%), respectively. In light of the reports of a strong correlation between radiological changes in the lung and regions receiving low doses calculated with the PBC (25), our results suggest that the lung might be less sensitive to these doses and that correlations should be sought with other dose levels in the AAA predictions. In terms of clinically relevant implications, these findings also suggest that current limits for the irradiation of the lung might have to be relaxed for AAA-based plans if the current levels of complications are considered acceptable.
Similar considerations also apply to the risk of complications from heart irradiation, for which it was found that the mean dose predicted by the AAA is 13% (range=4-22%) lower than by PBC-based calculations for BSC and 22% (range=4-44%) for WBO. This is in contrast with the results of Basran and colleagues who used a smaller patient population and concluded that there are no clinically significant differences between the predictions from the PBC, AAA and Monte Carlo model (12). Nevertheless, the highly significant difference in predicted mean dose suggests that the use of AAA-based calculations for doses together with parameters estimated from PBC-based calculations would lead to an underestimation of the risk to this organ and that the increased sensitivity of the heart should be taken into account when modelling the risk for heart complications. Indeed, it should be pointed-out that the PBC has been used for the calculation of reconstructed doses for most of the doses to the heart used by Darby et al. to investigate the risk for ischemic heart disease after breast radiotherapy (21, 26, 27) and our results suggest that the heart doses might have been overestimated, leading to a corresponding underestimation of heart sensitivity.
The AAA also predicts larger maximum dose hotspots than PBC, which can sometimes appear near sensitive structures such as the brachial plexus, thus suggesting that such structures may have a higher tolerance than expected from PBC-based clinical experience. As higher dose hotspots also appear as a feature of AAA planning (9), this topic itself deserves further investigations.
It should be noted that the focus of this study was on comparing clinically relevant parameters in cases which are evaluated according to existing criteria known to lead to high control and low complication rates (1). The quality of AAA-based planning for radiotherapy is a separate topic that has been investigated elsewhere (9). Nevertheless, many of the differences found achieved statistical significance and this suggests that tolerance levels for normal tissues and even recommendations for clinical acceptance of AAA-devised breast irradiation plans would need to be re-evaluated if the aim is to maintain the current level of control and complication rates. Indeed, using for example the AAA-predicted low doses to the heart with the low sensitivity derived from the analysis of clinical data with PBC-predicted doses might induce a false confidence that the expected rate of major coronary events would be low when using AAA-based data. Similar considerations apply for the other parameters. It is also worth noting that the present analysis was performed on what is to our knowledge the largest population of patients with breast cancer to date, thus accounting for interpatient heterogeneity, a factor that was not present in many of the smaller earlier studies.
Conclusion
The AAA should be preferred over the PBC algorithm for breast cancer radiotherapy as it gives more realistic dose distributions. The significantly worse coverage of the targets (PTV and CTV-T) with the AAA and higher lung volumes irradiated with clinically relevant doses, as well as the maximum dose in hotspots near sensitive structures, indicate that the requirements for plan evaluation might have to be re-evaluated to account for the differences in dose predictions in breast radiotherapy planning. Furthermore, the potentially increased radiosensitivity of the heart identified through the AAA-based calculations suggests that revision of the current models for cardiovascular complications would also be needed.
Acknowledgements
Financial support from the LiU Cancer research network at Linköping University and Region Östergötland (Sweden) is gratefully acknowledged.
- Received January 14, 2015.
- Revision received January 30, 2015.
- Accepted February 2, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}