


Abstract
Background/Aim: Colorectal cancer (CRC) is one of the most common causes of cancer-related deaths worldwide. DNA double-strand breaks (DSBs) are deleterious lesions that can lead to chromosomal anomalies, genomic instability and cancer. The histone H2AX plays an important role in response to DNA damage and phosphorylation of H2AX (p-H2AX) is evidence of DSBs. The aim of this study was to evaluate the clinical significance of p-H2AX expression in CRC. Patients and Methods: p-H2AX expression in CRC tissues was analyzed by immunohistochemistry and correlated with clinicopathological variables using the chi-square test. The prognostic value of p-H2AX for distant metastasis-free survival (DMFS) and overall survival (OS) was evaluated by Kaplan-Meier estimates and the individual prognostic components were analyzed with Cox regression analysis. Results: A high p-H2AX expression in CRC tissues was associated with tumor stage and perineurial invasion. Furthermore, a high p-H2AX expression was associated with poor DMFS and OS. Cox regression analysis also revealed that p-H2AX was an independent predictor of DMFS and OS. Conclusion: A high p-H2AX expression in CRC tissues is associated with a more malignant cancer behavior, as well as poor patient survival. p-H2AX may, therefore, be an independent prognostic predictor for CRC, as well as a potential therapeutic target.
Colorectal cancer (CRC) is one of the most common and preventable forms of cancer worldwide. Its incidence varies among different populations, with the highest being reported in Western and industrialized countries (1), including Taiwan. The traditional evaluation of the prognosis of CRC has relied, as with most other malignant tumours, on the stage of disease at the time of clinical presentation. Other factors currently commonly considered include performance status, weight loss and the presence or absence of symptoms at diagnosis, as well as pathological parameters, including tumour size, tumour differentiation and histological subtype (2-4). It is important to discover prognostic factors as well as therapeutic targets for CRC.
DNA damage response (DDR) is an important cellular guard that protects genetic material from a constant barrage of genotoxic agents. To ensure their survival after genomic insult, cells orchestrate a signalling cascade that leads to checkpoint-mediated cell-cycle arrest and the repair of damaged DNA (5-7). Failure of this process can lead to catastrophic cellular consequences, including the development of numerous disorders, such as cancer (8, 9). Because of its intimate connection with human health, deciphering the molecular mechanisms of DDR is of great interest (7, 10).
Clinicopathological characteristics in colorectal carcinoma.
Phosphorylation of the H2AX histone (p-H2AX) is an early indicator of DNA double-strand breaks (DSBs) and resulting DDR (11). When DSBs occur, a PI3-like kinase and DNA-dependent protein kinases become activated and phosphorylate H2AX on a carboxyl serine residue (Ser139) to generate γ-H2AX (7, 11, 12). The expression of p-H2AX plays a critical role in controlling both DNA repair and checkpoint activation in a variety of organisms from yeast to humans (13). Detection of p-H2AX foci has been used as a biomarker for aging and cancer, as a biodosimeter for drug development and radiation exposure, and for clinical trials, for cancer chemo- and radiotherapy (14, 15). Furthermore, emerging uses for p-H2AX include detection of toxic environmental agents and chronic inflammation (16).
The overexpression of p-H2AX has been observed in multiple types of cancer, including lung (3), cervical (17), breast (18), renal and bladder (19) cancer. Although accumulating evidence suggests that p-H2AX plays an important role in tumourigenesis, its role in CRC remains unclear. In this study, the expression of p-H2AX in CRC tissues was determined and its association with clinicopathological variables and prognosis of patients with CRC was analysed. Our results showed that p-H2AX expression was elevated in CRC tissues and was associated with a more malignant cancer behaviour and poor prognosis.
Correlation of p-H2AX expression with clinicopathological characteristics in colorectal carcinoma.
Patients and Methods
Tissue sample collection. From 2006 to 2007, cancer tissue samples from 92 patients with newly diagnosed and surgically treated CRC were collected at Kaohsiung Medical University Hospital. This study was reviewed and approved by the Institutional Review Board of Kaohsiung Medical University Hospital (KMUH-IRB-20130167). Staging was performed according to the American Joint Committee on Cancer tumour-node-metastasis staging system (20) and the patholo gical grade was classified according to World Health Organization histological criteria (21). Distant metastasis-free survival (DMFS) was defined as the period of time from the date of surgery until the date of first distant metastasis. Overall survival (OS) was defined as the period of time from the date of surgery until the date when the patient died of cancer.
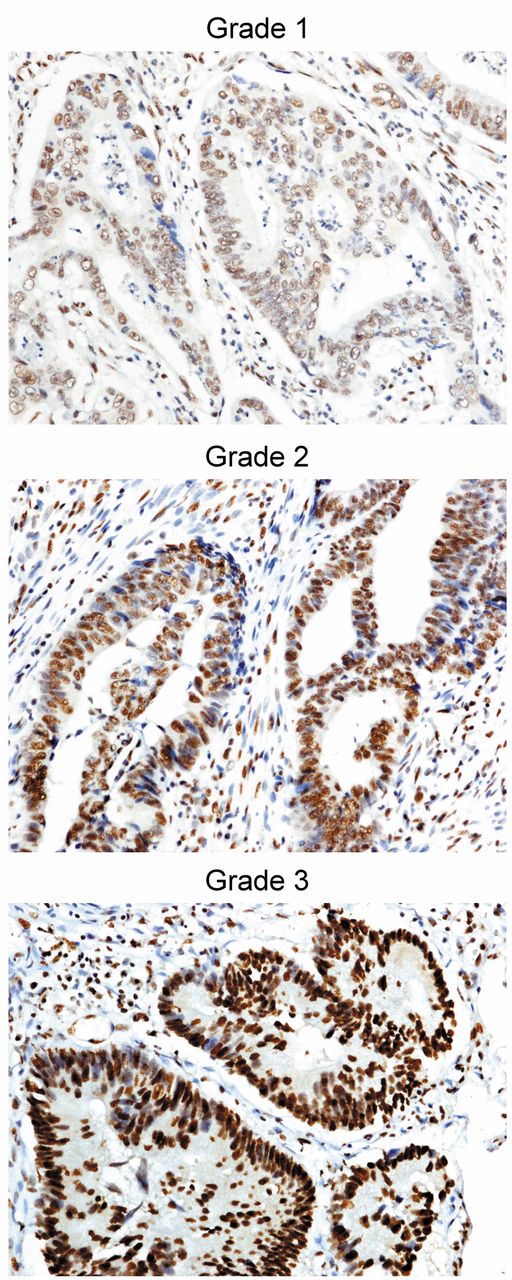
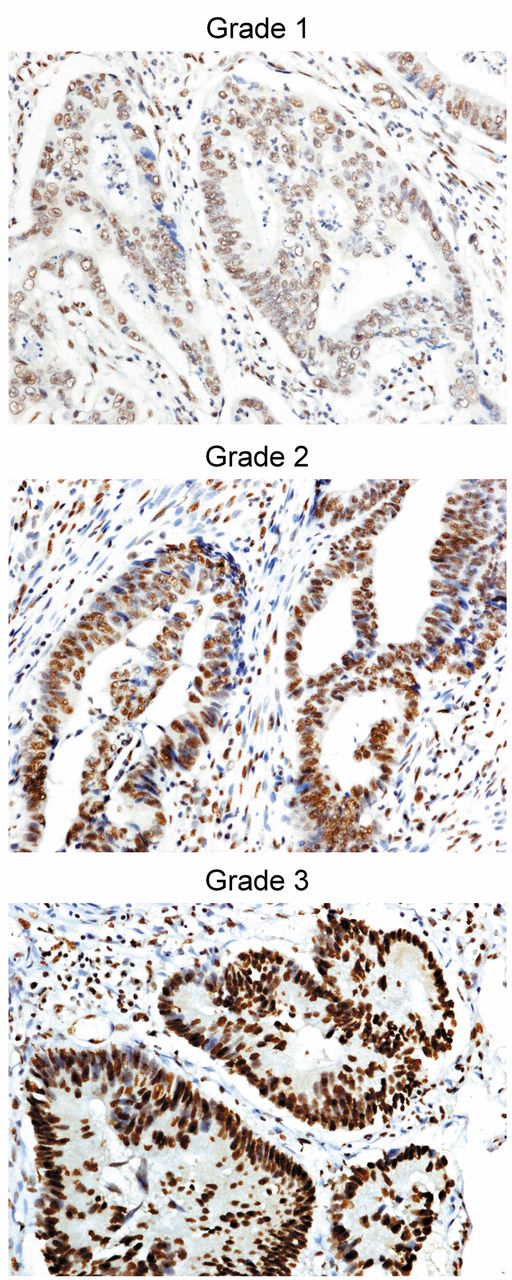
The expression of phospho-H2AX in colorectal cancer tissues, determined by immunohistochemistry, was stratified into the following categories based on the nuclear intensity grade: grade 1, negative and weak staining of tumour cells; grade 2, moderate staining of tumour cells; and grade 3, strong staining of tumour cells (original magnification ×200).
Immunohistochemistry. Immunostaining for p-H2AX on Ser139 (Bioybyt, Ltd., Cambridge, UK) was performed using a fully automated Bond-Max system (Leica Microsystems, Wetzlar, Germany). Slides containing tissue sections cut from formalin-fixed, paraffin-embedded tissue microarray blocks were dried for 1 hour at 60°C. The slides were then covered by Bond Universal Covertiles and placed into the Bond-Max instrument. All subsequent steps were performed by the automated instrument according to the manufacturer's instructions (Leica Microsystems) as follows: (i) deparaffinization of the tissue on the slides by rinsing with Bond Dewax Solution at 72°C; (ii) heat-induced epitope retrieval (antigen unmasking) with Bond Epitope Retrieval Solution 1 for 20 minutes at 100°C; (iii) peroxide block for 5 minutes at room temperature; (iv) incubation with rabbit polyclonal anti-p-H2AX antibody at a dilution of 1:200 for 30 minutes at room temperature; (v) Bond Polymer treatment for 8 minutes at room temperature; (vi) colour development with DAB 3,3’-diaminobenzidine tetrahydrochloride as a chromogen for 5 minutes at room temperature; and (vii) haematoxylin counterstaining for 5 minutes followed by mounting of the slides and examination by light microscopy. All images were captured using a Nikon E-800M microscope and then processed using PhotoImpact X3 (Ottawa, Canada). A negative control was obtained by substituting the primary antibody with the immunoglobulin fraction of non-immune rabbit serum in each staining run.
Evaluation of immunohistochemical staining. The scoring of p-H2AX staining was based on intensity grade representing the estimated average nuclear staining intensity of positive tumour cells as follows: grade 1, negative and weak immuno staining; grade 2, moderate immunostaining; and grade 3, strong immunostaining. Only the staining in tumour cells (approximately 1,000 cells in 3-4 high-power fields) was calculated. Two independent pathologists (Y-TC and C-YC) without prior knowledge of each patient's clinical information determined the immunostaining of p-H2AX for each specimen separately, whereas the rare cases with discordant scores were re-evaluated and scored based on a consensus.
Statistical analysis. All statistical analyses were performed using the SPSS 19.0 statistical package (SPSS, Inc., Chicago, USA). For p-H2AX expression, an intensity grade of 1 was categorized as a low expression and grades 2 and 3 as a high expression. The chi-square test was used to compare the high and low p-H2AX expression groups with regard to gender, age at diagnosis, tumour stage, tumour grade, vascular invasion, perineurial invasion and carcinoembryonic antigen (CEA) level. Survival curves were generated using Kaplan-Meier estimates and the significance of differences between curves was evaluated by the log-rank test. Hazard ratios (HRs) and 95% confidence intervals (CIs), computed from univariate and multivariate Cox regression models, were used to investigate the relationship between clinicopathological characteristics and survival. All p-values less than 0.05 were considered to be statistically significant.
Results
The expression profile of p-H2AX in CRC tissue samples. The expressions of p-H2AX in CRC tissues and the clinicopathological characteristics of the patients are summarized in Figure 1 and Table I. The localization of p-H2AX expression was predominantly nuclear in the staining of the CRC lesions. The p-H2AX expression in the cancer tissues was classified into three scores as shown in Figure 1. For further statistical analysis, an intensity of grade 1 (negative and weak) was categorized as a low p-H2AX expression (39.1%) and grade 2 (moderate) and 3 (strong) as a high p-H2AX expression (60.9%) (Table I).
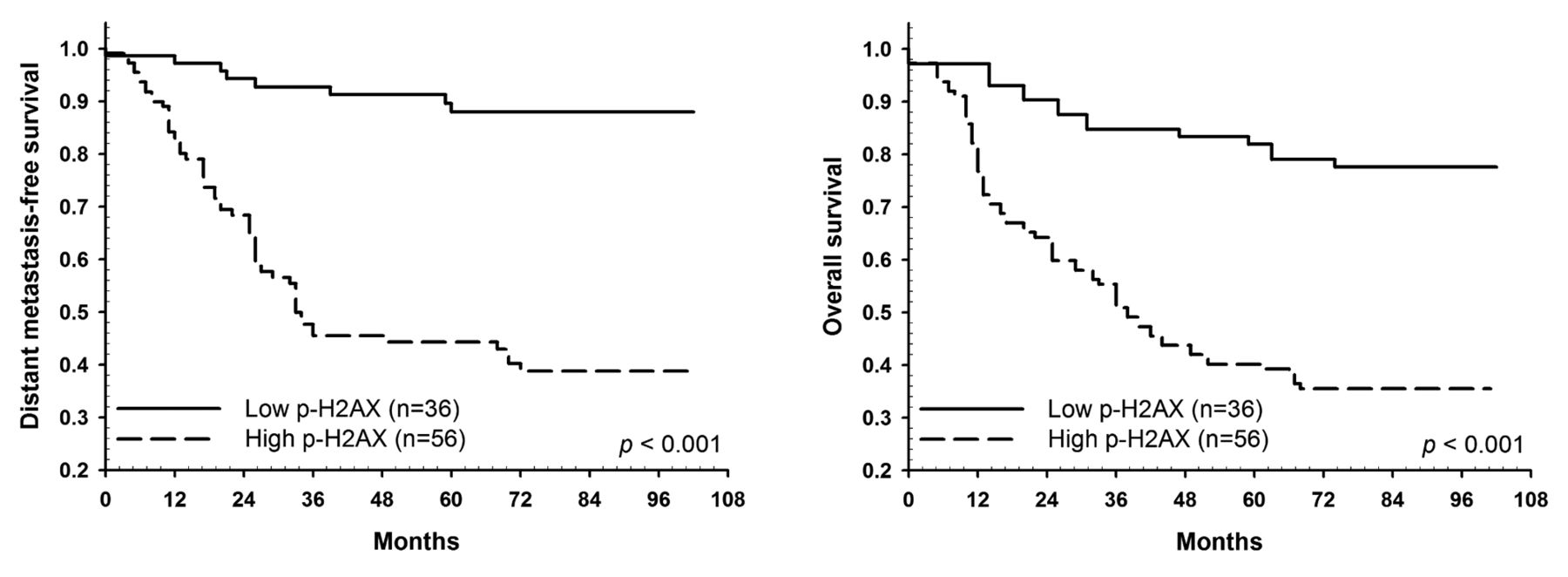
Kaplan-Meier survival curves generated for metastasis-free and overall survival rates of patients with colorectal cancer with low and high p-H2AX expressions as determined by immunohistochemistry.
Correlation of p-H2AX expression in CRC tissues with clinicopathological characteristics. To explore the potential role of p-H2AX in CRC, the expression patterns of p-H2AX were correlated to clinicopathological variables including gender, age at diagnosis, tumour stage, tumour grade, vascular invasion, perineurial invasion and CEA level (Table I). A high p-H2AX expression in CRC tissues was significantly associated with advanced tumour stage and positive perineurial invasion (p<0.001 and p=0.016, respectively; Table II). However, p-H2AX expression was not associated with gender, age at diagnosis, tumour grade, vascular invasion or CEA level (Table II).
Univariate and multivariable analysis of metastasis-free survival for colorectal carcinoma.
Univariate and multivariable analysis of overall survival for colorectal carcinoma.
Survival analysis. The expression patterns of p-H2AX in CRC tissues were further correlated with the DMFS and OS of the patients by Kaplan-Meier estimates. Lower DMFS and OS rates were observed in the high p-H2AX expressing group (intensity grades 2 and 3; p<0.001 and p<0.001, respectively) as determined by the log-rank test (Figure 2).
To evaluate the risk factors associated with CRC, HRs were estimated by univariate and multivariate Cox regression as shown in Table III and IV. In the univariate analysis, the factors associated with DMFS included tumour stage (p<0.001), vascular invasion (p=0.004), perineurial invasion (p=0.011), CEA level (p=0.017) and p-H2AX expression (p<0.001) (Table III). However, after adjusting for gender, age at diagnosis, tumour stage, tumour grade, vascular invasion, perineurial invasion and CEA level, only tumour stage (p=0.015) and p-H2AX expression (p=0.005) were independent predictors of DMFS in multivariate Cox regression analysis (Table III).
The factors associated with OS included tumour stage (p=0.004), vascular invasion (p=0.040), perineurial invasion (p=0.007), CEA level (p=0.021) and p-H2AX expression (p<0.001) (Table IV). However, after adjusting for gender, age at diagnosis, tumour stage, tumour grade, vascular invasion, perineurial invasion and CEA level, tumour grade (p=0.013) and p-H2AX expression (p=0.001) were the only independent predictors of OS in multi variate Cox regression analysis (Table IV).
Discussion
To the best of our knowledge, this is the first study to evaluate the prognostic significance of p-H2AX expression in CRC. Our results showed that p-H2AX levels may reflect endogenous genomic instability in cancerous tissues. Increasing staining of p-H2AX was associated with unfavourable risk factors, including higher tumour stage and perineurial invasion. In addition, a statistically significant association between high p-H2AX expression levels and worse DMFS and OS were noted in the patients with CRC. However, low p-H2AX expression levels may be indicative of a slowly proliferating, less aggressive tumour phenotype with good prognostic features. Such tumours may provide enough time to allow for DNA repair, which requires low p-H2AX levels. In contrast, high p-H2AX expression levels may indicate a more aggressive, highly proliferating tumour phenotype, leading to massive DNA defects and a worse prognosis, suggesting that p-H2AX signalling plays an important role in CRC tumourigenesis.
Before genomic instability and malignant conversion, human cells activate a DDR network correlated with DNA damage. In the later stages of DDR, the γ-H2AX foci become larger and, thus, a higher concentration of repair proteins can be measured (3). Recently, Jumonji domain containing protein 2B (JMJD2B) knockdown has been shown to increase the γ-H2AX level in CRC cell lines in both normoxia and hypoxia. In addition, γ-H2AX levels in tumour tissues harvested from a xenograft model were found to be markedly increased in JMJD2B-silenced tumours (22, 23). Two distinct kinase signalling cascades, the ATM-CHK2 and ATRCHK1 pathways, which are activated by DSBs and single-stranded DNA, respectively, have been shown to primarily orchestrate cellular responses to DNA damage and lead to the phosphorylation of H2AX (Ser139) (24). In addition, RhoB-deficient cells have been shown to accumulate endogenous p-H2AX and chromosomal abnormalities suggesting that RhoB loss increases DSB-mediated genomic instability and tumour progression in osteosarcoma and colon cell lines (25). Numerous studies have suggested that miRNAs play a crucial role in regulating the DNA damage pathway in cancer development. miR-138 and miR-24 have been shown to modulate the DNA damage response by targeting H2AX directly in cancer cell lines (26, 27), whereas miR-383 has been shown to reduce the abundance of the phosphorylated form of H2AX at the Ser139 site by inducing cell cycle arrest at the G1 phase (28, 29).
In conclusion, using a cohort of 92 CRC patients, we observed a positive association between p-H2AX expression and malignant CRC behaviour. A high p-H2AX expression was found to be independently associated with poor DMFS and OS in multivariate Cox regression analysis. Further investigations are required to explore the detailed mechanisms by which the p-H2AX signalling pathway is involved in CRC tumorigenesis and to establish new diagnostic and therapeutic strategies using p-H2AX as a target.
Acknowledgements
The study was supported by grants from Kaohsiung Medical University Hospital (KMUH100-0M12 and KMUH101-1M24).
Footnotes
-
Conflicts of interest
All Authors declare that they have no conflicting interests.
- Received December 16, 2014.
- Revision received January 10, 2015.
- Accepted January 16, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Loss of cyclin A2 in murine colonic epithelial cells disrupts colon homeostasis by triggering DNA damage and dysplasia and high cyclin A2 expression is a good-prognosis factor in patients with colorectal cancer
- Hyperthermia Suppresses Post - In Vitro Proliferation and Tumor Growth in Murine Malignant Melanoma and Colon Carcinoma
- Forecasting Survival Probabilities After Radiotherapy of Metastatic Epidural Spinal Cord Compression from Colorectal Cancer in the Elderly