


Abstract
Background: Octogenarians with ovarian cancer limited to the abdomen may not be willing or able to undergo systemic chemotherapy. Low-dose pressurized intraperitoneal aerosol chemotherapy (PIPAC) with cisplatin and doxorubicin is a form of intra-abdominal chemotherapy which can be applied repeatedly and potentially prevents from the systemic side-effects of chemotherapy. Case Report: We present the case of an 84-year-old woman with laparoscopically and histologically confirmed ovarian cancer who refused to undergo systemic chemotherapy. She was treated with eight courses q 28-104 days of low-dose PIPAC with cisplatin at 7.5 mg/m2 and doxorubicin at 1.5 mg/m2 at 12 mmHg and 37°C for 30 min. Objective tumor response was noted, defined as tumor regression on histology, and stable disease noted by peritoneal carcinomatosis index on repeated video-laparoscopy and abdominal computed tomographic scan. The treatment was well-tolerated with no Common Terminology Criteria for Adverse Events (CTCAE) CTCAE >2. With a follow-up of 15 months, the patient is alive and clinically stable. The quality of life measured by the European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30 demonstrated improvement over 5-6 months (global physical score, global health score, global quality of live) without cumulative increase of gastrointestinal toxicity. Conclusion: Low-dose PIPAC is a new form of intraperitoneal chemotherapy which may be applied repeatedly in octogenarian patients. PIPAC may be an alternative and well-tolerated treatment for selected octogenarian patients with ovarian cancer limited to the abdomen who cannot be treated with systemic chemotherapy.
- Ovarian cancer
- quality of life
- antineoplastic agents
- adverse effects
- intraperitoneal chemotherapy
- peritoneal carcinomatosis
- octogenarian
- high pressure
The incidence of ovarian cancer (OC) increases with age (1). In an aging population, geriatric patients with OC will, therefore, be an increasing clinical challenge. The geriatric patient population is characterized by a high degree of comorbidities, frailty, and psychodynamic changes, often precluding the application of systemic chemotherapy (2). In a review of chemotherapy-related side-effects, Kayl and Meyers cite hair loss (50%), changes in taste (46%), and fatigue (42%) as the most bothersome symptoms (3). These numbers may even be higher in geriatric populations of patients with cancer. It is of note, however, that there is a lack of literature on the efficacy and side-effects of systemic chemotherapy in geriatric women with OC. In a PUBMED search (search date: July 14, 2014; search terms: ovarian cancer, chemotherapy, systemic therapy, geriatric, octogenarian, side effects, comorbidity), only eight articles reporting on this topic were identified. In summary, geriatric patients with OC are often unable or unwilling to undergo systemic chemotherapy in the frontline situation, and are even less so in the recurrent situation. For example, Harlan et al. reported that only 30.4% to 34.1% of women over 75 years of age received guideline therapies compared to 55% to 75% of younger patients (4). Side-effects are significantly more common among geriatric patients with OC and dose reductions are more often necessary compared to younger patients (4-6).
Therefore, effective and less morbid alternatives to systemic chemotherapy are a therapy need in geriatric patients with OC, which is currently not met. Pressurized intraperitoneal aerosol chemotherapy (PIPAC) is a new form of intraperitoneal chemotherapy (IPC) taking advantage of the physical properties of gas and pressure (7). This approach is based on the observation that application of chemotherapy under pressure significantly enhances tumor drug uptake (8). PIPAC may, therefore, be a way to increase the distribution and infiltration depth of IPC, while at the same time reducing the chemotherapy dose by a factor of 10 as compared to systemic applications. As proof of concept, PIPAC achieved a superior distribution on the peritoneum and a better penetration into peritoneal nodules compared to conventional IPC in an ex vivo model (9). In an in vivo experimental study using five pigs, PIPAC yielded a better distribution of a pressurized test dye within the abdominal cavity and a better penetration into the peritoneum compared to peritoneal lavage (10). Based on these experimental data, PIPAC has been tested in humans with advanced peritoneal carcinomatosis (11, 12). In these preliminary applications, PIPAC induced regression of peritoneal nodules with limited hepatic and renal toxicity (13). In addition, the procedure has been shown to be safe regarding occupational health aspects such as air contamination of operatiing theaters with aerosol chemotherapy particles (14).
As of yet, there are no data describing PIPAC in octogenarian patients with OC. Herein we report eight consecutive successful applications of PIPAC with cisplatin and doxorubicin in an 84-year-old patient with advanced OC. This case report indicates that PIPAC can be applied repeatedly and can induce disease stabilization in selected octogenarian patients with OC. PIPAC may be an alternative therapy for octogenarians with OC limited to the abdomen who are not able or willing to undergo standard systemic chemotherapy.
Case Report
We present the case of an 84-year-old woman with OC, first diagnosed in 2011. Initially, the patient underwent diagnostic laparoscopy with removal of ascites and histological confirmation of OC by peritoneal biopsy. Between 2011 and 2013, repeated abdominal paracenteses were performed. The patient presented to our Clinic in June 2013 with rising serum Cancer Antigen (CA) 125 levels and suspected disease progression on abdominal sonography and abdominal computed tomography (CT). The patient was offered but refused to undergo systemic chemotherapy. After Tumor Board approval, the patient was offered PIPAC with cisplatin and doxorubicin. PIPAC was not administered with research intent. The patient provided written informed consent for this treatment. PIPAC was not standard treatment at our Institution at the time the patient was treated. Approval by the Ethics Committee of the Ruhr University Bochum for PIPAC was obtained.
From June 2013 to June 2014, the patient underwent eight courses q 28-154 days of PIPAC with cisplatin at 7.5 mg/m2 and doxorubicin at 1.5 mg/m2 at 12 mmHg and 37°C for 30 min. The PIPAC procedure was performed as described elsewhere (11). Briefly, in an operating room equipped with laminar airflow, after insufflation of a 12 mmHg CO2 pneumoperitoneum, two balloon safety trocars (5 and 12 mm, Applied Medical, Duesseldorf, Germany) were inserted into the abdominal wall. Video documentation was started and the peritoneal carcinomatosis index (PCI) was determined according to Mazzei et al., based on lesion size and distribution (15). A biopsy was taken for histological confirmation of malignancy during the first and all subsequent procedures in order to ascertain tumor regression. Ascites volume was documented and ascites was removed. A nebulizer (Reger Medizintechnik, Rottweil, Germany) was then connected to an intravenous high-pressure injector (Injektron 82M; MedTron, Saarbruecken, Germany) and inserted into the abdomen. The tightness of the abdomen was documented via a zero-flow of CO2. A pressurized aerosol containing doxorubicin at a dose of 1.5 mg/m2 body surface in 50 ml of 0.9% NaCl solution followed by cisplatin at a dose of 7.5 mg/m2 body surface in 150 ml 0.9% NaCl solution were applied via nebulizer and injector. The dosage used for this patient was based on previous clinical experience in patients with peritoneal carcinomatosis treated with PIPAC using this dosage and formulation (11-13). Injection parameters were set at a flow rate of 30 ml/min and a maximum upstream pressure of 200 psi in the high-pressure injector. The injection was remote-controlled to exclude occupational exposure. The therapeutic capnoperitoneum was maintained for 30 min at a temperature of 37°C. The chemotherapy aerosol was then exsufflated via a closed line over two sequential microparticle filters into the airwaste system of the hospital. Finally, trocars were retracted and laparoscopy ended. No drainage of the abdomen was applied. Adverse events were graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0 (16). Quality of life was measured by the standardized European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30 questionnaire, a validated tool for assessing quality of life in patients with cancer.
Figure 1 shows images of the videolaparoscopy during the first and sixth PIPACs, demonstrating peritoneal carcinomatosis. Sclerosis of peritoneal nodules was observed, as well as reticular scarring of the visceral and parietal peritoneum. Objective tumor response was noted after the first PIPAC, defined as tumor regression on histology. Specifically, pathological tumor response with regressive changes of cancer cells was noted in repeated peritoneal biopsies taken during all PIPAC procedures. Figure 2 demonstrates histopathological specimens taken during the first and sixth PIPAC confirming peritoneal carcinomatosis and regressive changes of the tumor cells. Before the first PIPAC, histology showed peritoneal infiltration of a poorly differentiated adenocarcinoma. Follow-up biopsies showed sustained regressive tumor changes, fibrosis, and acute and chronic inflammation.

Intraoperative findings (macroscopy) during videolaparoscopy before pressurized intraperitoneal aerosol chemotherapy (PIPAC) (A; upper panel: left lower abdomen and pelvis; lower panel: left upper abdomen) and before PIPAC #7 (B). After therapy, sclerosis of peritoneal nodules was observed, as well as reticular scarring of the visceral and parietal peritoneum. The total peritoneal Carcinomatosis Index remained constant, since quantitative parameters (the number and the size of tumor nodes) did not change significantly, although the qualitative aspect of tumor nodes changed after therapy.
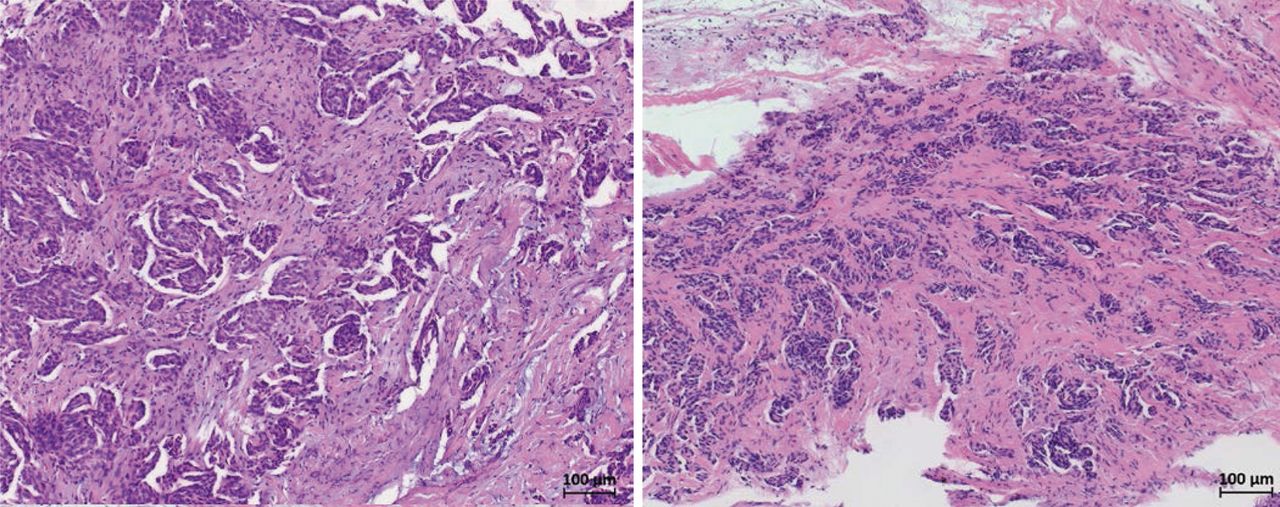
Intraoperative findings (microscopy) before pressurized intraperitoneal aerosol chemotherapy (PIPAC) (left panel) and PIPAC #6 (right panel) confirming peritoneal carcinomatosis. Before PIPAC, histology showed peritoneal infiltration by a poorly differentiated adenocarcinoma. Follow-up biopsies showed sustained regressive tumor changes, fibrosis, and acute and chronic inflammation.

Quality of life scores according to the European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30 questionnaire for global physical status (A), global health status (B), global quality of life (C), and overall score (D) before the first pressurized intraperitoneal aerosol chemotherapy (PIPAC) and throughout treatment courses 1 to 8.
Intraoperative assessment of PCI during repeated video-laparoscopy showed stable disease. The PCI was 31, 27, 36, 16, 28, 32, 27, and 22 at the first and subsequent PIPACs, respectively. The treatment was well tolerated. CTCAE events grade 1 (nausea) and grade 2 (abdominal pain) were noted within 72 h after the PIPAC procedures. No CTCAE even higher than grade 2 was observed. There was no hematological toxicity noted from red and white blood cell counts performed seven days after each PIPAC. There was no acute or cumulative renal or hepatic toxicity, with stable values for creatinine, gamma glutamyl transferase (gGT), aspartate aminotransferase (GOT/ ASAT), alanine aminotransferase (GPT/ALAT), bilirubin, and Quick test (thromboplastin time) throughout all PIPAC procedures. Serial serum CA 125 values during therapy indicated stable disease: 501, 639, 575, 600, 554, 509, 420, and 506 U/ml at PIPACs 1 to 8, respectively.
Figure 3 shows the EORTC QLQ-C30 quality of life scores for global physical status, global health status, global quality of life, and the overall score, indicating an initial improvement of the quality of life during the first five treatment courses and a decline thereafter. Scores for pain, vomiting, and constipation/diarrhea were stable throughout the treatment, suggesting that repeated PIPACs did not result in acute or cumulative gastrointestinal toxicity in this patient.
Discussion
OC in octogenarians is difficult to treat and available treatment options are often not realized because of existing comorbidities or lack of patient consent (2-5). On the other hand, the course of disease in older patients is often prolonged and less aggressive than in younger patients, making limited and less morbid treatment modalities attractive for this patient population. Additional treatment options tailored to the needs of geriatric patients with OC are needed. IPC may be such a treatment option aimed at controlling peritoneal carcinomatosis in women with recurrent OC limited to the abdomen. PIPAC is a variant of IPC using pressurized, aerosolized chemotherapy in order to improve drug distribution and tumor penetration, which has been demonstrated in experimental models (7, 9, 10). Preliminary data in patients with advanced peritoneal carcinomatosis demonstrated good tolerability and objective tumor response (11, 12). PIPAC can be applied repeatedly without cumulative toxicity and a low systemic chemotherapy burden (13). These properties make PIPAC a potentially attractive therapeutic tool in geriatric patients with OC, such as the octogenarian patient described in this case report. In addition, PIPAC may be a way to improve the quality of life of elderly patients with recurrent OC compared to systemic chemotherapy. In our case, under PIPAC, objective tumor response was noted, defined as tumor regression on histology and video-laparoscopy. Abdominal CT scans, serum CA 125 measurements, and PCI assessments during video-laparoscopy showed stable disease.
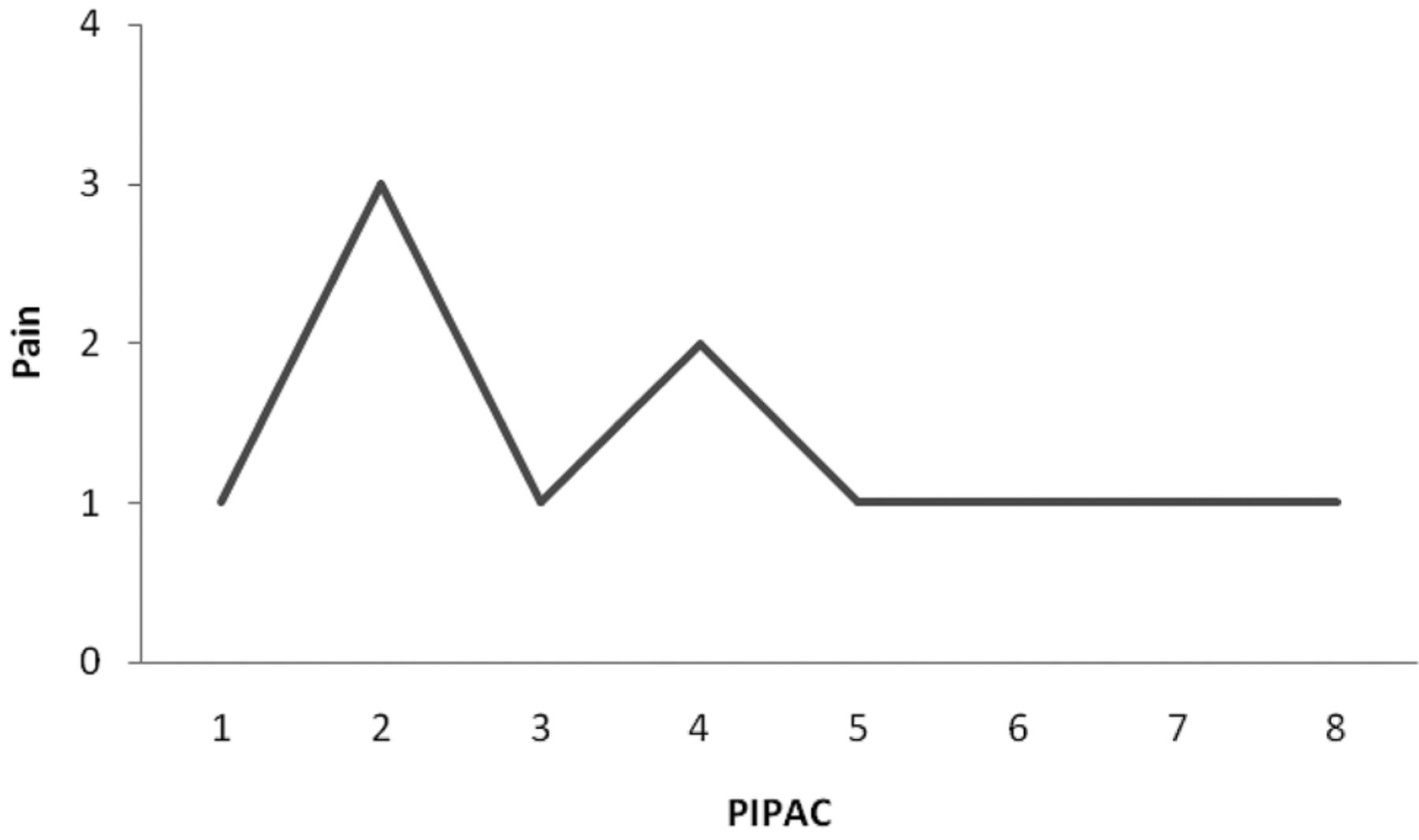
Quality of life scores according to the European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30 questionnaire for pain before the first pressurized intraperitoneal aerosol chemotherapy (PIPAC) and during treatment courses 1 to 8.
Quality of life is a major treatment goal in oncology, especially in palliative and geriatric patients. Thus, we made efforts to document eventual changes in quality of life throughout the treatment using a validated tool, namely the EORTC QLQ-C30 questionnaire. The treatment was well-tolerated and the quality of life initially improved during therapy, with a decline after five treatment courses. However, the quality of life never deteriorated below the initial values recorded before the start of PIPAC. Moreover, gastrointestinal quality of life measures remained stable throughout all PIPAC courses, which indicates that this form of IPC, although repeatedly applied directly into the abdomen, does not result in acute or cumulative gastrointestinal toxicity.
Geriatric patients with OC may have a protracted and indolent disease course (4, 5). Thus, best supportive care may be a valid option in patients such as the one described in this case report. On the other hand, the patient had signs and symptoms of progressive disease before the start of PIPAC, i.e. repeated paracenteses, a rising CA 125 level and abdominal CT scans suggestive of progression. On the basis of a case report, however, to what extent octogenarian patients would benefit from IPC such as PIPAC cannot be concluded. Based on this case experience, we propose to further explore PIPAC as a new and potentially valuable additional treatment in selected geriatric patients with recurrent OC who are not able or willing to undergo systemic chemotherapy.
Conclusion
PIPAC is a new form of IPC, which can be applied repeatedly over a long period of time and may become a treatment complementary to systemic chemotherapy in selected geriatric patients with OC.
Footnotes
-
Conflicts of Interest
MR discloses that he holds a patent for the high-pressure device used to deliver the intraperitoneal chemotherapy described in this article, and that he has received royalties from Reger Medizintechnik GmbH, Rottweil, Germany. The other Authors have no conflicts of interest.
- Received December 3, 2014.
- Revision received December 13, 2014.
- Accepted December 19, 2014.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}