


Abstract
Aim: To evaluate the clinicopathological features of extraskeletal osteosarcoma (ESOS) and its response to multimodal therapy. Patients and Methods: A nationwide cohort comprising all Norwegian histologically verified ESOS patients between 1975 and 2009 supplemented with clinical reports from all hospitals involved in sarcoma management. Results: Thirty-seven patients were classified as ESOS, mostly elderly people. Seventy-six % had an axial tumour, including nine patients with radiation-induced ESOS. The gender balance was equal. The 5-year sarcoma-specific survival (SSS) was 16 %. Adequate surgical remission had a positive impact on SSS, in contrast to chemotherapy and radiotherapy. Primary metastatic disease, elevated tumour size and elevated serum alkaline phosphatase, serum lactate dehydrogenase and Ki67, respectively, all predicted poor outcome. Conclusion: The relatively poor prognosis of ESOS may relate to both primary chemotherapy resistance and different biologic characteristics of these tumours as compared to conventional osteosarcoma. Hence, new predictive molecular markers and therapeutic approaches for treatment of ESOS are needed.
Extraskeletal osteosarcoma (ESOS) is a rare malignancy, even compared to skeletal osteosarcoma (OS). The former accounts for approximately 1-2 % of all soft tissue sarcomas (1, 2) and only 2-5 % of all OS (3, 4). Morphologically, ESOS resembles undifferentiated pleomorphic sarcoma except for the presence of osteoid and, sometimes, chondroid matrix (5). The phenotypes of ESOS are comparable to those described in skeletal OS (6).
Since first described by Wilson in 1941 (7), few larger series have been published (1-4, 8-15). Most ESOS are high-grade neoplasms (5, 6) and they occur mostly in the deeper soft tissues of elderly patients (2, 3). ESOSs have poor prognosis (8-10), although both surgery (2, 3, 13) and chemotherapy (2, 13) are reported to have a positive impact on survival. However, there is still no international consensus on the optimal chemotherapy combination (16).
The purpose of this study was to describe histopathological and clinical characteristics, as well as survival outcomes, among 37 ESOS patients from an unselected Norwegian ESOS population along with a review of the relevant literature. To our knowledge, no nationwide study on ESOSs has been published since the late 1970s (17).
Patients and Methods
Patient cohort. The reporting of malignant neoplasms to the Norwegian Cancer Registry (NCR) has been compulsory since 1953 and its completeness has been reported to be higher than 95 % (18). To ensure completeness, all ESOS and skeletal OS, as well as spindle cell non-osteosarcomas (SCS) arising from bone tissue reported to NCR during 1975-2009 were re-evaluated and complemented with data from all Norwegian hospitals involved in sarcoma manage ment (19). The gross study material amounted to 702 cases (19). We were not able to scrutinize the very high number of SCS from soft tissue (close to 3.000 cases) as part of this work.
Five hundred and nine OS patients were identified, including 36 ESOS patients. The latter group was supplemented with one extra case identified in a previous publication (20). Skeletal or extraskeletal origin was decided by radiographic images and/or histology from surgical resection, biopsy or autopsy in one case. All excluded cases have previously been presented (19). We have included post mortem diagnosis (one case) and all secondary ESOS; i.e., radiation-induced ESOS (R-ESOS) or patients with other predispositions for ESOS. The database is located at the NCR. The study did not require a formal ethical approval since the data registration was in line with the legitimate mandate of the NCR.
Histopathology. Histological sections from 30 of the 37 cases were retrieved from the files and re-examined by at least two senior pathologists. The latter seven cases were considered eligible based on review of available histological reports, including one patient with a final diagnosis by second opinion at the Mayo Clinic and one case already re-evaluated in connection with a previous study (20). Malignancy grade was recorded together with the histological classification based on the predominant phenotype (Figures 1-2 and Table I). A mixed phenotype was introduced when there was no obviously dominating phenotype.
Immunohistochemistry. Twenty-six cases had paraffin blocks available for immunohistochemistry. The immunohistochemical profile of these tumours was evaluated using 10 different antibodies (Table II). These tumour biomarkers are known to reflect tumour growth, metastatic potential and response to treatment. Positive score was recorded as +, ++, +++, respectively (+, 1% < 33%; ++, ≥ 33% < 66%; +++, ≥ 66%). Normal range was defined as negative or +, otherwise considered as elevated.
Clinicopathological variables. All clinicopathological variables were retrospectively validated based on multiple and partly overlapping data and registry sources supplemented with clinical records from hospitals involved in sarcoma management. These variables are presented in Tables I and III and Figure 3. As expected, we have not reached full completeness regarding clinical information for all patients in the study (Table I).
We defined metastasis within six weeks from primary diagnosis as “primary metastatic disease” (19). “Tumour size” was measured from surgical specimens and/or radiographic images at diagnosis and defined as the maximum length of tumour in cm. “Duration of symptoms” was the interval in months between first symptom and time of biopsy. Normal range for serum alkaline phosphatase (ALP) and serum lactate dehydrogenase (LDH) were measured in international units at time of diagnosis in line with the common Nordic Reference interval from May 2003 (21); i.e., ALP: 0-17 years, < 400 U/l; >17 years, < 105 U/l. LDH: 0-10 years; <400 U/l, 11-70 years, <205 U/l; >70 years, < 255 U/l. Analyses before May 2003 needed a 60 and 50 % reduction in values, respectively, to be compatible with the above mentioned thresholds.
Treatment variables. Relevant treatment variables are presented in Table IV. Best local surgical margins were classified according to Enneking et al. (22) and dichotomised between wide or marginal margins and intralesional or residual macroscopic tumour, respectively. We differentiated between amputation (last surgery performed) and other surgery. Patients with metastatic disease at time of diagnosis were in need for a complete surgical remission for both primary tumour and lung metastases in order to be classified as having received adequate surgery.
Chemotherapeutic agents and the cumulative dose in each patient were recorded for each patient given such treatment (Table V). Radiotherapy in patients treated with a curative aim is also presented.
Statistical analyses. Survival analysis using Kaplan-Meier estimates (23) and log-rank test (24) were used to analyse sarcoma-specific survival (SSS) from relevant clinicopathological variables and molecular markers (Ki67, p53). Overall survival was not used in these analyses due to ESOSs' increased risk for death of other reasons compared to younger patients. Sarcoma-specific death or treatment-related death were the endpoints of SSS. The endpoint for all survivors in the study was set to July 2013 using updated registries (19) to prevent bias due to non-identical follow-up of patients with few or frequent appointments. All survival analyses (Figure 4 and Table VI) were presented with a corresponding 95 % confidence interval (CI) in order to capture the uncertainty of the estimates due to relatively few cases. We have not applied multivariate Cox regression (25) analyses as a consequence of the latter. The statistical analyses were conducted using the SPSS, version 22 (SPSS, Inc., Chicago, IL, U.S.A.) and Stata, version 13.1, software (Stata corporation, College Station, TX, U.S.A.).
Results
Incidence. Thirty-seven patients were diagnosed with ESOS between 1975 and 2009, of whom three cases in the 1970s, 11 in the 1980s, seven in the 1990s and 16 during the 2000s, respectively (Table I). Hence, the average annual incidence for all ESOS was 0.2 per million during this period. ESOS accounted to 7 % of all OS in Norway between 1975 and 2009 (19).
Histopathology. Thirty-six of the 37 cases were of high-grade malignancy (Table I). Most high-grade ESOSs demonstrated varying expression of the major OS phenotypes (6, 19) (Figure 1) but more infrequent variants were also documented (Figure 2). The low-grade case was well-differentiated and located to the left breast in a 24-year-old female, as previously published, including a picture of this tumour (20). The osteoblastic phenotype was the prevailing phenotype, followed by the fibroblastic and the mixed variants (Table I). The telangiectatic and small cell subtypes were not verified in this limited series.
Immunohistochemistry. All tissue specimens had undergone decalcification prior to paraffin embedding. This may explain why nine of the 26 available specimens gave suboptimal immunohistochemistry results and were excluded.
Cell proliferation. Ki67 nuclear immunostaining was performed in all 17 cases. Seven of these tumours had an elevated score (++, +++), otherwise normal score (+/-). Two patients had negative immunoreactivity, including the low-grade case. An elevated Ki67 score was significantly associated with a dismal survival (Table VI).
p53. A nuclear p53 immunostaining was presented in 10 cases, including three cases with elevated score. Each of the latter three cases showed also an elevated Ki67 immunoreactivity.
Patients with normal score had improved survival compared to the latter three cases, but no significant difference in SSS was documented (p=0.11). This calculation, however, cannot be taken for granted due to the small sample size.
Mesenchymal-Epithelial Transition (MET). Most cases extensively expressed N or P cadherin, or both. Only one case was negative for both markers. All cases were negative for E cadherin. In two cases, desmin was observed in a few tumour cells (+) and there was no over-expression. Cytokeratins (AE1/AE3) were present in seven cases, both in the giant cells and in spindle-shaped, fibroblast-like cells, including one case with elevated value.

a-d. Heterogenity in an extraskeletal osteosarcoma (OS) with a dominant osteoblastic phenotype. All pictures from the same tumour in X 200. A-Osteoblastic OS with atypical cells and unmineralized osteoid. B-Osteoblastic OS area with mineralized bone trabequla. C-Chondroblastic OS with cartilaginous tissue with atypical chondroblasts and atypical spindle cells in the periphery. D-Fibroblastic OS with fusiform atypical spindle cells arranged in interlacing fascicles.
Macrophages. All 17 cases were CD68-positive and only one case was associated with elevated score.
Apoptosis. Caspase 3 immunoreactivity and Bcl2 expression was observed in all cases and 11 cases, respectively, all with normal expression.
Clinicopathological data. Ten patients were classified as secondary ESOS with one case arising from myositis ossificans. The remaining nine patients had R-ESOS; two following treatment for breast cancer, four for gynaecological cancer, one for cancer of the oral cavity, one for larynx cancer and one following mantle field irradiation due to Hodgkin's disease, respectively. Seven of these patients developed R-ESOSs from 8-35 years following radiotherapy (median=16 years). We had no exact information regarding time-line for the latter two patients.
We report about the same balance between both sexes for all ESOS patients, in contrast to a male to female ratio of only 0.1 among patients with R-ESOS (Table I). A dominant peak of ESOS among elderly patients was observed (Figure 3). Median age was 68 years for all patients (range=17 to 91 years) and 64 years among the group of R-ESOS (range=33 to 89 years).
Only 9 ESOS were located in an extremity (Table III). Thirty-five of all tumours arose in deep soft tissues with only two cases originating superficially (dermis or subcutis). Median tumour size and symptom length were 10 cm (range=1 to 25 cm) and 4 months (range=1 to 24 months), respectively. The corresponding figures for patients with R-ESOS were 14 cm (range=4 to 20 cm) and 9 months (range=1 to 16 months), respectively.
Clinicopathological variables in 37 patients with extraskeletal osteosarcoma.
Metastasis or local recurrence during follow-up. Information regarding time of metastasis, based on radiographic images and/or biopsy or fine needle aspiration cytology (26), was available in 33 patients. Metastases were present in eight patients at diagnosis, including four patients with R-ESOS (Table I). Six of these patients had lung-metastases only. Among patients without primary metastatic disease, 52 % (13 cases) developed metastases and 28 % (7 cases) experienced local relapse during follow-up, respectively. Five patients in the former group were also represented in the latter. The median time from diagnosis to first metastatic event or local recurrence was 1.2 years (range=two months to 12 years) and 11 months (range=5 months to 9 years), respectively.
Treatment modalities. Table IV outlines the extent of treatment administered to ESOS patients and is further presented below.
Surgery. Twenty-nine patients underwent at least one operation (Table IV). We had only clinical information regarding six of the remaining eight patients. Two of these ESOS patients underwent only palliative radiotherapy in a primary metastatic setting. Another patient died due to complications from neoadjuvant chemotherapy before surgery was attempted. Further, a 53-year-old man died of pulmonary oedema due to acute arrhythmia. In this case, autopsy verified an ESOS of the pharynx region with compression of the 9th and 10th cranial nerve. The latter two patients received neither oncological treatment nor surgical intervention.
Antibodies used for immunohistochemistry in 26 extraskeletal osteosarcomas.
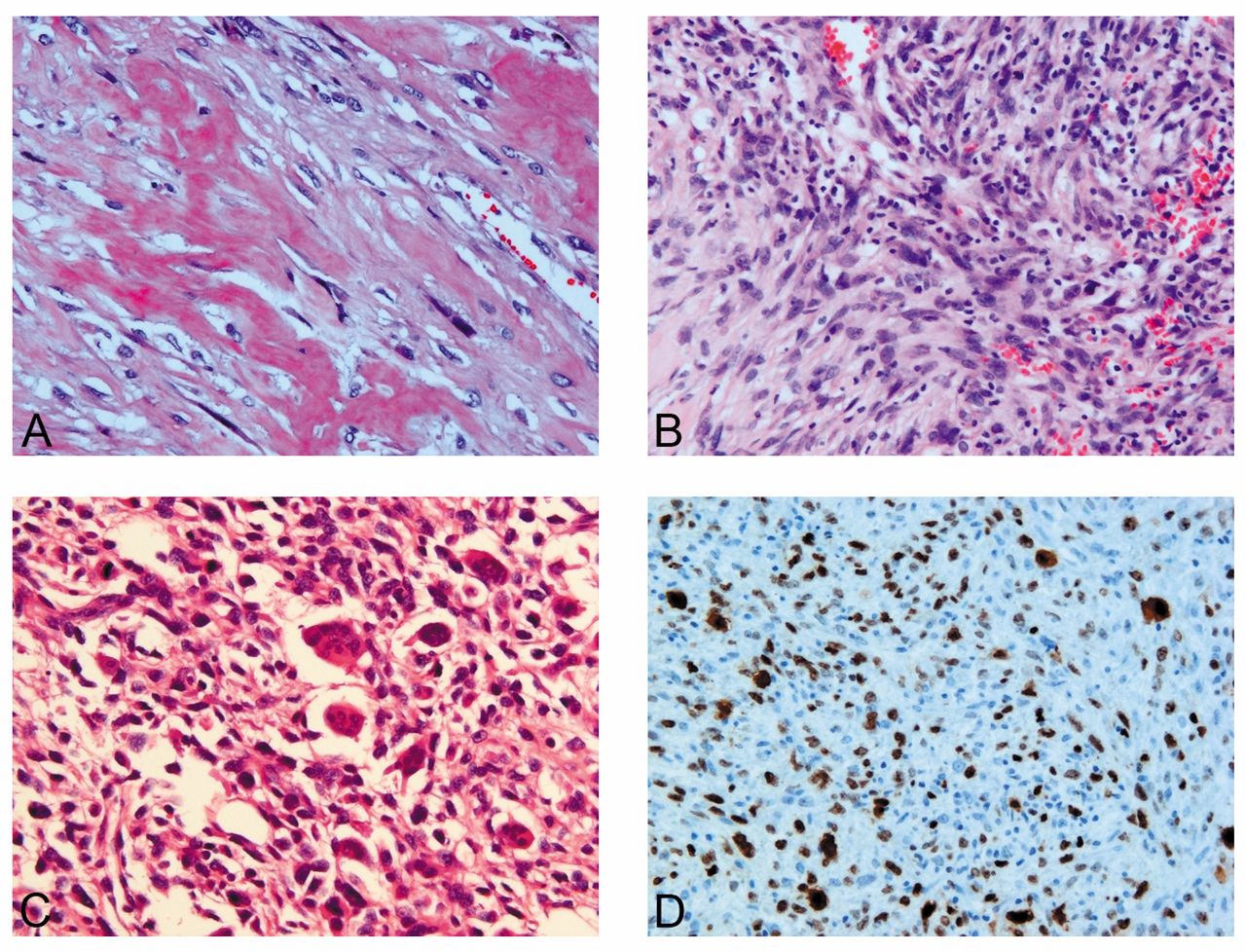
a-d. Heterogenity in an extraskeletal osteosarcoma (OS) with a dominant osteoblastic phenotype. All pictures from the same tumour in X 200. A-Osteoblastic OS with atypical cells and unmineralized osteoid. B-Pleomorphic undifferentiated sarcoma type. Extensive spindling of atypical mononuclear cells arranged in storiform pattern. C-Giant cell rich OS. Cell rich tumour tissue with many atypical giant cells surrounded by sarcomatous spindle cells. D-Positive Ki67 immunostaining in most tumour cells.
Anatomical distribution of 37 patients with extraskeletal osteosarcoma.
Information regarding surgical margins was available in 26 cases (Table IV); 65 % of these patients (17 cases) achieved adequate primary surgical treatment. We observed no difference in SSS (p=0.99) between patients treated with resection and those treated by amputation (Table IV).
Chemotherapy. Eleven patients received chemotherapy with a curative treatment intention in nine of these cases (Table IV). Eight of the latter nine patients were given at least two of the following drugs: doxorubicin, ifosfamide and cisplatin, respectively, although other agents were also used (Table V). We observed large differences in cumulative chemotherapy dosages between these patients (Table V).
Among the 11 patients who received chemotherapy, ten patients were also treated with surgery. Seven of the latter group underwent only postoperative chemotherapy. Five patients were treated with chemotherapy, surgery and radio therapy.

Gender (bar chart, left axis) and age at diagnosis (line diagram, right axis) of 37 patients with extraskeletal osteosarcoma.
Four patients received chemotherapy in a metastatic setting, including three patients with primary metastatic disease. All these patients had rapid tumour progression despite the use of chemotherapy.
Radiotherapy. Six ESOS patients received radiotherapy with curative intention as part of their multimodal treatment (Table IV), shortly presented below. All died later of their sarcoma.
One patient underwent 36 Gy (1.8 Gy×20) as hyper-fractionated/accelerated treatment according to the Scandinavian Sarcoma Group XIII protocol (27) for an ESOS in the left breast (20). The second patient had also an ESOS in the breast and received 50 Gy (2 Gy×25) as postoperative treatment due to marginal primary surgery. She underwent additional palliative radiation (3 Gy×10) towards two metastases in the left lung about 15 months later, after a previous attempt of secondary line chemotherapy and right-sided thoracotomy. Further, a 59-year-old man underwent radiotherapy to 48 Gy (2 Gy×24) as part of pre- and post-operative chemotherapy towards an ESOS of the upper arm. He received additional palliative treatment (3 Gy×13) for skeletal metastasis of lumbal/sacralcolumna roughly 2 years later.
The fourth patient received 54 Gy (3 Gy×18) as postoperative radiotherapy after his third local relapse of an ESOS of the left leg. He underwent additional palliative treatment (3 Gy×10) towards skeletal metastasis in sternum/ clavicle approximately nine years later. The fifth patient received 50 Gy (2 Gy×25) towards her right hip region after surgical resection of a large tumour from the right buttocks region where the sciatic nerve was preserved. She experienced a local relapse 11 months later and died four months later. Lastly, an 80-year-old man received 60 Gy as postoperative treatment for an ESOS of left lung/chest wall but he died three months after initial diagnosis.
Survival analyses. We found a significant difference in survival between ESOS and skeletal OS patients (p<0.001) as presented in Figure 4a, the latter adopted from a recent report (19). One-year SSS was 61 % (95 % CI=43-75 %) for all ESOSs but five-year SSS was only 16 % (95 % CI=6-30 %). We were unable to demonstrate any significant difference in outcome between R-ESOS and the remaining group (p=0.36), although we experienced a slightly poorer survival among the former group (Figure 4b). Table VI presents the results of univariate analyses as one-year SSS according to different characteristics of ESOS. Adequate surgery had a positive impact on SSS, while primary metastatic disease and tumour size above median value were associated with a dismal prognosis. Elevated ALP, LDH or Ki67, respectively, all predicted poor outcome. Neither chemo therapy nor radiotherapy, despite curative treatment intention, reached significance in our analyses (Table VI).

Sarcoma-specific survival (SSS) of extraskeletal osteosarcoma (ESOS). A-SSS of ESOS versus skeletal osteosarcoma (OS) (p<0.001) B-SSS of radiation-induced ESOS (R-ESOS) versus other ESOS (p=0.36).
Discussion
To our knowledge, this is the first large nationwide study of ESOS. Most previous studies are case reports, institutional or multicenter studies, with the largest consisting of 88 cases (8). Recently, however, a study from the SEER database with 256 ESOS patients was published (15).
The present cohort comprises both histopathological and clinical variables, as well as survival data. We assume the completeness of the present database to be close to 100 % of all ESOS cases in Norway from 1975 to 2009 (19). We conducted a total re-evaluation of all histological reports for all ESOS and OS, as well as SCS patients in bone tissue for the given time period (19). Further, 30 of the 37 cases in the present study were re-examined histologically and 26 cases were also examined by immunohistochemistry (see below). Still, we have no guarantee that “all” ESOS cases in Norway are actually included in the present study as histological examination is subjective with poor intra- and interreproducibility (28). Due to the very high number of soft tissue SCS, these cases were not evaluated as part of this work. Hence, our supplemented case from a previous study (20), initially reported as an undifferentiated pleomorphic sarcoma in soft tissue, was not included in our gross material of 702 patients (19).
Summary of treatments in 37 patients with extraskeletal osteosarcoma.
One hundred and fifty-eight cases (194-36 cases) were presented as not verified OS in our previous publication (19), including 112 cases of SCS. The differential diagnosis of ESOS includes carcinosarcoma (29-32), synovial sarcoma (6) and undifferentiated pleomorphic sarcoma (5, 33). ESOS has also been mistaken for myositis ossificans (8, 10). One patient in our study was initially diagnosed with the latter diagnosis several years prior to the former. Similar cases of myositis ossificans transforming to ESOS have also previously been reported (3, 13, 34).
Most tumours in the present study were heterogeneous. Despite variation in histological appearance, consensus in dominating phenotype was achieved in most cases, otherwise reported as mixed phenotype. We have performed immunohistochemical analyses of ESOS, including the epithelial marker AE1/AE3, in order to exclude other diagnostic possibilities as mentioned above. Only Ki67 was significantly correlated to outcome (Table VI). This may relate to a potential damage of tissue or deleted tumour epitopes due to the decalcification. Selection of tissue blocks may also have biased the results. Hence, our experience is in line with the literature stating that ESOS does not reveal any characteristic immunophenotype (4, 35, 36).
We confirm that ESOS mainly is a high-grade malignant sarcoma that commonly affects an older age group than skeletal OS (6). Low-grade ESOSs are extremely rare (37-39); and our cohort comprises only one such case. We observed a slightly higher percentage of ESOS in % of all OS than previously presented (3, 4, 15).
Cumulative dose of chemotherapy in 11 patients receiving chemotherapy for extraskeletal osteosarcoma.
Univariate Kaplan-Meier analyses of one-year sarcoma-specific survival according to different characteristics of 37 patients with extraskeletal osteosarcoma including treatment-related variables.
Previous radiation therapy is well-known to be a predisposing factor to the development of sarcomas (40-42) and several cases of ESOS have also been described (2-4, 8-10). Nine of our patients had received radiotherapy to the area where their ESOS developed (24 % of all cases). This is a substantially higher proportion than previously reported due, perhaps, to differences in the patient base analysed; in our situation, an unselected nationwide cohort. Although the poor prognosis of radiation-induced soft-tissue sarcomas is well-known (14, 43), we were unable to demonstrate any significant difference of outcome in our patients with ESOS (Figure 4b), as found in a recent study (14), probably because of the small sample size.
We report about the same gender balance among all ESOS in line with two previous reports (3, 4). Our findings were influenced by a clear majority of women among the R-ESOS patients (89 %). Although the majority of previous case series (2, 9, 10, 12, 36) found a male to female predominance, two recent reports observed the opposite (14, 15) suggesting that gender distribution varies in each cohort due to chance (14).
Less than 10 % of all ESOS in our study had a superficial origin in agreement with previous publications (6, 44, 45). Nevertheless, with one exception (15), the distribution of anatomical sites (Table II) differs substantially from the present ESOSs literature (6); reported to be most commonly located in the lower extremity, with the thigh being the single most frequent site. This result was partly influenced of the increased proportion of R-ESOS in our study, all with non-extremity localisation. Still, most of our cases from the truncus were not related to previous radiation. For example, seven of our cases were from the breast and lungs. Primary ESOS from these anatomical regions are very rare (20, 46-50).
Tumour size above median value of 10 cm was a negative prognostic factor in our study (Table VI), in line with a previous report (15). A corresponding result regarding tumour size >5 cm was also documented in another study (9), whereas small tumour size did not equate with good prognosis in a different publication (10). Further, anatomical tumour site had no significant influence on survival (Table VI) in contrast to the recent SEER study (15).
Both elevated LDH and ALP were negative prognostic factors based on univariate analyses (Table VI), similar to high-grade OS patients (51, 52). We have not identified information of these two variables in previous studies of ESOS.
About 25 % of all patients in the present study had metastatic disease at presentation, just slightly above a previous study (9) but substantial higher than other reports (10, 13). Primary metastatic disease was a negative prognostic factor for survival (Table VI), in line with the literature for OS (19, 53, 54). A large part of the cases experienced local recurrences and/or distant metastases during follow-up, in line with the available literature (1, 3, 4, 9, 10).
The traditional treatment of ESOS has usually been restricted to local intervention, including surgery alone or a combination of surgery and radiotherapy (55). Treatment consists of amputation or wide surgical resection with no difference in survival between patients treated with resection and those treated by amputation (12, 13). We confirm the latter result. Adequate surgery was a statistically significant favourable prognostic factor in our study (Table VI), in line with a previous report (13). However, the use of radiotherapy did not appear to influence survival (Table VI) probably because of poor marginal status among the patients given such treatment. In general, OS is also known to be relatively resistant to such therapy (56).
ESOS tends to have a poor response to chemotherapy (3, 9, 10, 12, 55), although recent studies (2, 13) have shown that multi-agent chemotherapy may yield good results. As of today, there are no clear guidelines for adjuvant treatment (16). Most of our patients received only postoperative chemotherapy, like in other recent series (12, 13). The use of chemotherapy did not appear to influence survival in the present study. This result may be related to the limited number of patients in the present study and the broad spectrum of drugs used (Table V).
Overall, the prognosis of ESOS is generally poor; older literature states 25 to 50 % in five-year survival (4, 8, 57). However, recent poly-chemotherapy regimens combined with wide surgical margins have described overall survival rates of 66 to 77 % (2, 13). We present a dismal survival in this report, with only 16 % five-year SSS. The poor results may be related to a relatively high median age at diagnosis for the included patients and that one fourth of all cases had primary metastatic disease and/or R-ESOS, respectively. Further, only about half of the population received adequate surgery and neither radiotherapy nor chemotherapy appeared to influence survival. In general, the poor tolerance to adjuvant chemo therapy among elderly represents another hurdle (58).
To our knowledge, this is the first large study addressing clinicopathological features for ESOS patients in a nationwide setting. We confirm primary ESOS as a high-grade malignancy among elderly patients. Three quarters of all patients had ESOS with non-extremity localisation, partly explained by nine cases of R-ESOS. Adequate surgery improved SSS in contrast to chemotherapy and radiotherapy. The relatively poor prognosis of ESOS, due to frequent recurrences or metastases, may relate to primary chemotherapy resistance.
Acknowledgement
The Authors would like to thank professor and senior consultant pathologist Jahn M. Nesland, Department of Pathology, Oslo University Hospital and senior consultant pathologist Per J. Bøhler, Department of Pathology, Oslo University Hospital for their valuable feedback and diagnostic support. Technical support from bioengineer Ellen Hellesylt, Department of Pathology, Oslo University Hospital is also appreciated. This project was supported by the South-Eastern Norway Regional Health Authority Research Program, with a pilot project supported by the National Resource Centre for Sarcomas in Norway.
Footnotes
-
This article is freely accessible online.
-
Conflict of interests
The Authors declare no conflict of interests regarding the publication of this paper. The NCR has approved the use of these data for international publishing. The Authors alone are responsible for the content and writing of the paper.
- Received December 11, 2014.
- Revision received January 14, 2015.
- Accepted January 16, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.