


Abstract
Background/Aim: Despite an excellent prognosis, certain patients with thyroid cancer suffer from locally invasive disease that cannot be controlled by conventional therapy. Our previous study suggested that hypoxia inducible factor-1-alpha (HIF1α) might be an important marker for the identification of and a treatment target of intractable thyroid cancer. Therefore, in the present study, we established an orthotopic mouse surgical model of thyroid cancer that mimics the clinical setting, and evaluated the effect of perioperative treatment with a HIF1α inhibitor. Materials and Methods: Seven thyroid cancer cell lines (SNU-790, BCPAP, KTC1, TPC1, TPC1-M, KTC2, and FRO) and four HIF1α inhibitors (echinomycin, LAQ824, temsirolimus, and vorinostat) were used in the present study. Expression of HIF1α and related proteins was evaluated in all cell lines; immunoblotting and cell proliferation assays were conducted; and echinomycin was validated in an orthotopic surgical mouse model. Results: Nuclear expression of HIF1α increased in tumorigenic cell lines, while HIF1α inhibitors inhibited proliferation and colony formation. In the orthotopic surgical model, the group treated with surgery and the echinomycin-treatment group showed a highly significant survival gain (p=0.001) compared to the control group. Conclusion: The highly significant survival gain resulting from their use in perioperative adjuvant treatment in vivo and their anticancer effect in vitro suggest that HIF1α inhibitors might be candidates for perioperative adjuvant chemotherapy for thyroid cancer. Combining adjuvant HIF1α inhibitor chemotherapy with surgery might be an effective therapeutic strategy for thyroid cancer that is refractory to conventional treatments.
- Thyroid cancer
- HIF1α inhibitor
- orthotopic mouse model
- molecular targeted therapy
- echinomycin
- adjuvant chemotherapy
Thyroid cancer is one of the most common malignancies and its incidence has steadily increased during the past decade in most countries including South Korea (1). Differentiated thyroid carcinoma has a favorable prognosis following conventional treatment with surgery and radioactive iodine therapy. Conversely, the treatment of poorly differentiated or undifferentiated thyroid carcinoma is still disappointing. Recent articles have suggested that improved survival can be achieved by surgical treatment, even in anaplastic thyroid carcinoma, for which ‘no treatment’ is considered the best option due to the grave prognosis, irrespective of treatment modality (2, 3).
In our previous study of an orthotopic model of papillary thyroid carcinoma (PTC), a more tumorigenic clone (TPC1-M) was established from the original cell line (TPC1) (4). Microarray analysis of these two PTC cell lines revealed that hypoxia inducible factor-1-alpha (HIF1α) was associated with the invasiveness of the tumorigenic cell line (5). These findings suggest that HIF1α might play an important role in tumorigenesis or tumor initiation of PTC.
In cancer cells, HIF1α is induced in response to hypoxia, growth factors, and genetic abnormalities (6). A high level of HIF1α expression has been reported to be associated with low survival rate, aggressive tumor behavior, angiogenesis, and metastasis in various types of cancers (7). In thyroid cancer, it has been demonstrated that HIF1α is expressed in thyroid tumors but not in healthy thyroid tissues (8-10) and expression of a high level of HIF1α protein significantly correlated with a high TNM stage and lymph node metastasis (11).

Tumorigenicity and immunoblotting analysis of hypoxia inducible factor-1-alpha (HIF1α) and related proteins of thyroid cancer cell lines.
As surgery has a key role in the treatment of thyroid carcinoma, we investigated the possibility of adjuvant targeted-therapy in the perioperative period. On the basis of our results from a previous study (4, 5), we hypothesized that HIF1α could be an effective molecular target for inhibiting the initiation of thyroid carcinoma. Therefore, we established an orthotopic surgical mouse model of thyroid cancer, mimicking the clinical setting, and evaluated the role of perioperative treatment with HIF1α inhibitors in this model.
Materials and Methods
Culture and preparation of cell lines. Seven thyroid cancer cell lines were used in the study; these comprised PTC cell lines (SNU-790, BCPAP, KTC1, TPC1, and TPC1-M) and anaplastic thyroid carcinoma cell lines (KTC2 and FRO). SNU-790 was obtained from the Korean Cell Line Bank (KCLB, Seoul, Korea). BCPAP was acquired from the German Collection of Microorganisms and Cell Cultures (DSMZ, Braunschweig, Germany). SNU-790 and BCPAP both harbor a BRAF (proto-oncogene B-Raf) mutation (12). TPC1, carrying the rearrangements of RET/PTC1 (the RET oncogene in PTC), was a kind gift from Dr. Jerome Hershman (VA Greater Los Angeles Healthcare System, Los Angeles, CA, USA) (13, 14). TPC1-M, a subclone of TPC1 with in vivo tumor growth and metastatic potential, was developed and provided by Dr. Gary Clayman (The University of Texas MD Anderson Cancer Center, Houston, TX, USA) (4). KTC1 and KTC2 were established at the Kawasaki Medical School in Japan, and were kindly offered to us for the present study. FRO was kindly provided by Dr. Minho Shong (Chungnam National University, Daejeon, Korea). Cells were cultured in RPMI-1640 medium (Invitrogen, Carlsbad, CA, USA), supplemented with 10% fetal bovine serum, 2 mM L-glutamine, and antibiotics, in an incubator at 37°C with 5% CO2.
Compounds. The HIF1α inhibitor echinomycin (quinomycin A; Santa Cruz Biotechnology, Dallas, TX, USA), the HIF1α and histone deacetylase (HDAC) inhibitor LAQ824 (Dacinostat; Selleckchem, Houston, TX, USA), the HIF1α and mammalian target of rapamycin inhibitor temsirolimus (LC Laboratories, Woburn, MA, USA), and the HIF1α and HDAC inhibitor vorinostat (LC Laboratories) were used in this study. HIF1α inhibitors were dissolved in dimethyl sulfoxide and diluted with RPMI-1640 medium to the desired concentration for in vitro experiments.
Cell proliferation assay. Proliferation analysis of each cell line was carried-out using a water-soluble tetrazolium (WST) assay. TPC1-M, SNU-790,and BCPAP cells were plated in triplicate at a density of 2×103 cells/well in 96-well plates, and cell viability was determined at 24 h intervals using the WST-8-based Cell Counting Kit-8 (Dojindo Molecular Technologies, Rockville, MD, USA), according to the manufacturer's instructions.
Colony-forming assay. For the colony-forming assay, 2,500 cells/well were seeded in 6-well plates and incubated in an incubator at 37°C with 5% CO2. After two days of culture, HIF1α inhibitors or control vehicle were administered in culture medium. When the number of colonies in the control reached more than 50, control and treated cells were fixed in ice-cold methanol for 30 min and stained with 0.005% crystal violet for 1 h. Colonies were counted in triplicate plates for each treatment.
Orthotopic mouse model of thyroid cancer. The orthotopic thyroid cancer model was developed in 8- to 12-week-old female nude mice, as previously described (4). All experimental studies involving the mice were carried out in accordance with a protocol approved by the Institutional Animal Care and Use Committee (IACUC) of Seoul National University Bundang Hospital (ICAUC no. 63-2012-037). For injection, TPC1-M cells were diluted to a final density of 2×105/μl in phosphate-buffered saline. Following anesthesia of each mouse, a 1 cm vertical incision was made on the anterior neck, and 1×106 cells (5 μl) were injected through the exposed strap muscles into the thyroid gland. The retracted submandibular glands were returned to their normal position, and the skin incision was closed.
Treatment groups in the orthotopic mouse model. Two weeks after the orthotopic cell implantation, 60 mice were divided into four groups in a random manner and treated as follows: the control group underwent a sham operation and treatment with the control vehicle; the surgery group underwent excision of tumors and treatment with the control vehicle; the echinomycin group underwent a sham operation and treatment with echinomycin (0.05 mg/kg); and the surgery plus echinomycin group underwent excision of tumors and treatment with echinomycin (0.05 mg/kg).
Treatment and surgery in the orthotopic mouse model. Treatment started two weeks after orthotopic cell implantation. Echinomycin (0.05 mg/kg) or the control vehicle was intraperitoneally administered at 0, 2, 4, 7, 9, and 11 day from the treatment, and surgery (excision of the tumor or sham operation) was performed on the seventh day post-treatment. Mice were sacrificed when they exhibited any signs of morbidity or distress, experienced a weight loss >20% of pre-injection body weight, or bore tumors that had grown to >1 cm diameter, or were culled after six months of follow-up observation.
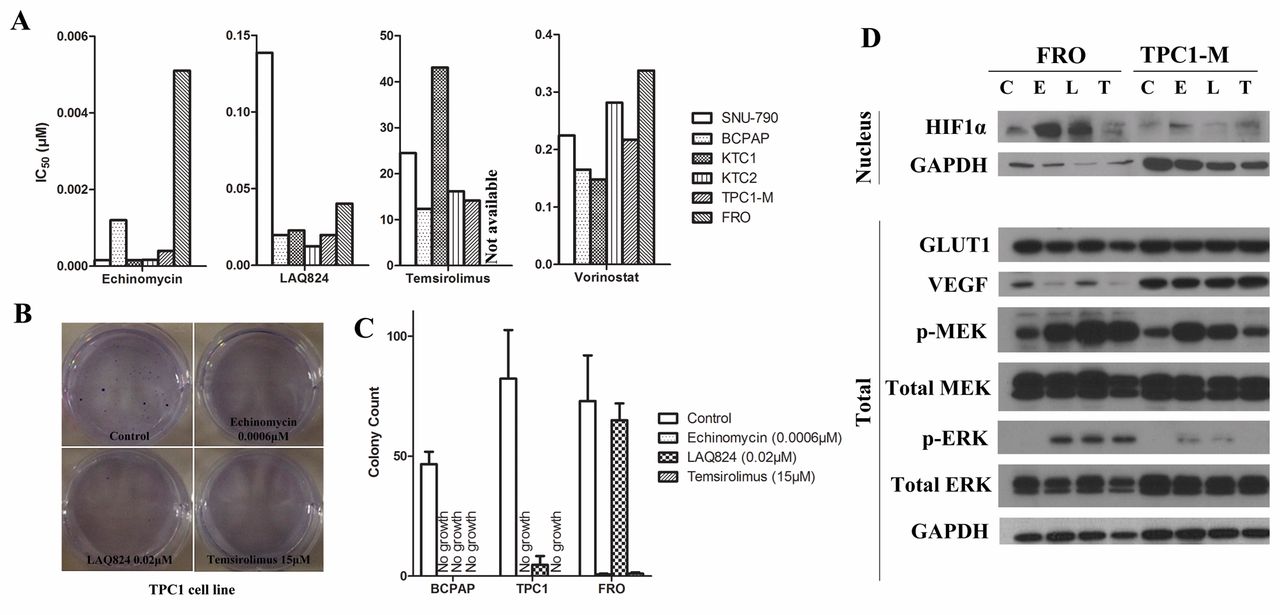
Inhibition of cell proliferation by hypoxia-inducible factor-1-alpha (HIF1α) inhibitors (echinomycin, LAQ824, temsirolimus, and vorinostat) and regulation of HIF1α and related-pathway proteins by HIF1α inhibitors in thyroid cancer cell lines. A: The half-maximal inhibitory concentration (IC50) values for HIF1α inhibitors for each of the three cell lines tested. B: Colony-forming assays performed in TPC1 cell line. C: Counting of colony according to the cell lines and drugs tested. D: Expression of HIF1α and related pathway proteins. C. Control, E. echinomycin, L. LAQ824, T. temsirolimus.
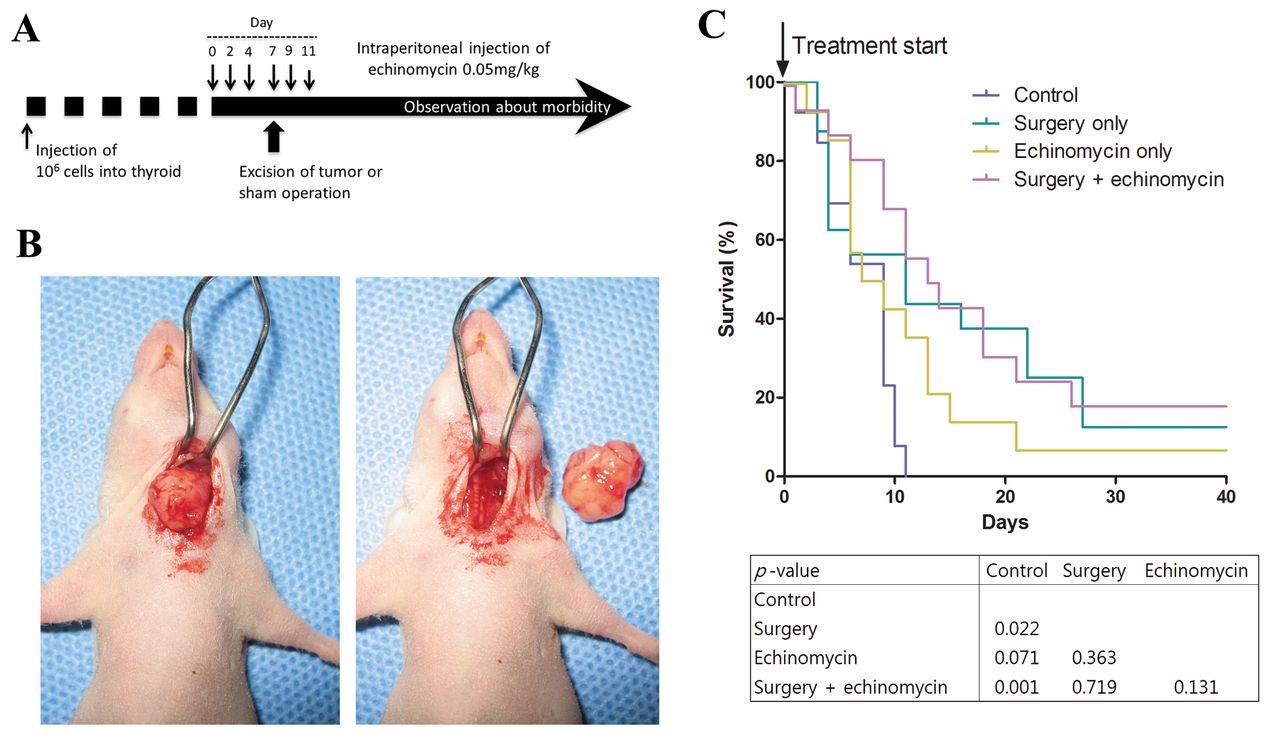
In vivo animal study using echinomycin. A: Schedule for perioperative treatment with hypoxia-inducible factor-1-alpha (HIF1α) inhibitor in the orthotopic mouse model of thyroid cancer. B: The procedure for surgical resection of tumors. C: Survival of mice in the differently-treated groups. The box below the graph indicates the p-value of log-rank test.
Immunoblotting. The following antibodies were used for immunoblotting of cell lines: HIF1α (BD Biosciences, San Jose, CA, USA), von Hippel-Lindau tumor suppressor (VHL; Abcam, Cambridge, UK), glucose transporter 1 (GLUT1; Abcam), MAPK/ERK kinase (MEK; Cell Signaling Technology, Danvers, MA, USA), vascular endothelial growth factor (VEGF; Abcam), phosphorylated MEK (p-MEK; Cell Signaling Technology), extracellular signal-regulated kinase (ERK; Santa Cruz Biotechnology), phosphorylated ERK (p-ERK; Cell Signaling Technology), and glyceraldehyde phosphate dehydrogenase (GAPDH; AbFrontier, Seoul, Korea).
Statistical analysis. The half maximal inhibitory concentration (IC50) value, at which 50% of the cell growth is inhibited compared to the control, was calculated by non-linear regression analysis using GraphPad Prism 4 software (GraphPad Software Inc., San Diego, CA, USA).
Survival of mice in the various treatment groups was analyzed using the Kaplan–Meier method, and results were compared using the log-rank test. The level of statistical significance was set at p<0.05. All statistical analyses were conducted using SPSS 12.0 (SPSS Inc., Chicago, IL, USA) and Graph-Pad Prism 4 (GraphPad Software Inc.) software programs.
Results
Tumorigenicity of thyroid cancer cell lines in vivo and expression of HIF1α and related proteins. Four cell lines, KTC1(15), KTC2(16), TPC1-M(4), and FRO(17), are known to be tumorigenic in nude mice. In the seven cell lines tested, increased nuclear expression of HIF1α was highly correlated with tumorigenic potential in three (KTC2, TPC1-M, and FRO) cell lines; two cell lines (SNU-790 and TPC1) that were not tumorigenic showed faint expression of HIF1α; and in two cell lines (KTC1and BCPAP), tumorigenicity did not correlate with expression of HIF1α. Cytoplasmic expression of VEGF was not dependent on nuclear HIF1α expression, and all cell lines, except for TPC1, had a high level of VEGF expression. Cytoplasmic expression of GLUT1 showed no variation between any of the cell lines. Furthermore, cytoplasmic expression of VHL showed no correlation with tumorigenesis (Figure 1).
Inhibition of cell proliferation by HIF1α inhibitors in thyroid cancer cell lines. All four HIF1α inhibitors (echinomycin, LAQ824, temsirolimus, and vorinostat) inhibited proliferation of the six cell lines tested, with different IC50 values (Figure 2A). The concentrations corresponding to the IC50 of echinomycin (0.0006 μM), LAQ824 (0.024 μM), and temsirolimus (15 μM) were used in colony-forming assays; vorinostat was excluded from the colony-forming assay because of its high IC50 value. All three drugs effectively inhibited colony formation of the BCPAP and TPC1 cell lines; echinomycin and temsirolimus, but not LAQ824, inhibited colony formation of the FRO cell line (Figure 2B and C).
Regulation of HIF1α and related proteins by HIF1α inhibitors in thyroid cancer cell lines. In the FRO cell line, expression of HIF1α was up-regulated by treatment with echinomycin or LAQ824, but it was unaffected by treatment with temsirolimus. In the TPC1-M cell line, expression of HIF1α was not significantly affected by treatment with any of the HIF1α inhibitors. GLUT1 expression was unaffected by treatment of any of the cell lines with HIF1α inhibitors. In the FRO cell line, expression of VEGF was suppressed by treatment with HIF1α inhibitors, especially echinomycin and temsirolimus. In the TPC1-M cell line, expression of VEGF was unaffected by treatment with HIF1α inhibitors. The expression of p-MEK and p-ERK was moderately up-regulated by treatment of both cell lines with HIF1α inhibitors, with stable expression of total MEK and ERK (Figure 2D).
Perioperative treatment with an HIF1α inhibitor in the orthotopic mouse model of thyroid cancer. The effect of perioperative treatment was evaluated with an HIF1α inhibitor in the orthotopic model of thyroid cancer, following the schedule shown in Figure 3A; the procedure for surgical resection of tumors is shown in Figure 3B. The echinomycin group had a higher survival rate than did the control group, but this failed to reach a statistically significant survival gain compared to the control group (p=0.071). In the surgery group, a survival gain was observed, and reached statistical significance (p=0.022). The surgery-plus-echinomycin group showed the highest survival rate, which was significantly higher (p=0.001) than that of the control group (Figure 3C).
Discussion
Novel agents are being assessed in phase II trials as molecular-targeted therapies for undifferentiated or poorly differentiated thyroid carcinoma, and most of these drugs (sorafenib, axitinib, motesanib, sunitinib, pazopanib, lenvatinib, cabozantinib, vandetanib, gefitinib, and selumetinib) are kinase inhibitors. However, the overall response rate to these drugs ranges between 0 and 53% (18). Phase III trials of vandetanib, cabozantinib, and sorafenib are now complete, and response rates of the drugs are 37%, 28%, and 23%, respectively (6); sorafenib (Nexavar®) is the most promising among these and a phase III trial of this drug was recently reported (19). However, these trials are carried-out in palliative settings where a large tumor is already established. Furthermore, the purpose of these drugs is to stabilize or shrink existing tumors. However, recent results suggest that even in anaplastic thyroid carcinoma, surgical treatment can improve patient survival (2, 3). Therefore, targeted-therapy that inhibits tumor progression from the microscopic remnant following surgery could be a more effective means of treatment. Based on the results from previous studies (4, 5), HIF1α was selected as a novel target for the treatment of thyroid carcinoma. We hypothesized that HIF1α may have a role during the development of clinically significant disease from the microscopic surgical remnant, since it is believed to play a major role in tumor initiation.
Various thyroid cancer cell lines (SNU-790, BCPAP, KTC1, KTC2, TPC1, TPC1-M, and FRO) were investigated in the present study. KTC2 and FRO, aggressive cell lines from undifferentiated carcinoma and TPC1-M (a more tumorigenic clone derived from TPC1) have high expression of HIF1α (Figure 1). However, there exists certain variation in that the tumorigenic KTC1 cell line had low expression of HIF1α and the non-tumorigenic BCPAP cell line high expression. The reason for this may be the presence of numerous molecules involved in the commitment to tumorigenesis and expression of HIF1α cannot be the only determinant. However, these results still show that those cell lines with nuclear expression of HIF1α have a higher potential for tumor formation in nude mice.
We also evaluated the molecules that regulate or are regulated by HIF1α. The VEGF and GLUT1 proteins are representative of molecules that are influenced by HIF1α but their expression did not correlate with the expression of HIF1α. VHL has an important role in the degradation of HIF1α but its expression did not correlate well with the level of HIF1α. Thus, we concluded that the tumorigenic potential of HIF1α might be unrelated to the expression of VEGF or VHL.
Four HIF1α inhibitors (echinomycin, LAQ824, temsirolimus, and vorinostat), with different mechanisms of action, were evaluated for anticancer effects on the thyroid cancer cell lines. Although all the agents inhibited cell proliferation and colony formation, echinomycin was selected for the in vivo study because it had the lowest IC50 and the strongest inhibition of colony formation in all the cell lines tested. The FRO and TPC1-M cell lines exhibited somewhat different results for protein expression following inhibitor treatment. In the FRO cell line, nuclear HIF1α expression was increased and VEGF expression was reduced by treatment with the HIF1α inhibitors. Currently, there exists no drug that can directly inhibit the expression of HIF1α itself. The available drugs inhibit HIF1α via many different mechanisms related to the action of HIF1α (7), and the level of HIF1α can vary with drug treatment; this could explain the results in the FRO cell line. In contrast, the TPC1-M cell line showed no change in HIF1α or VEGF expression. Thus, the TPC1-M cell line was selected for the animal study because the effect of HIF1α inhibitors in this cell line is at least unrelated to VEGF. Furthermore, the TPC1 and TPC1-M cell lines are closer to poorly-differentiated thyroid carcinoma that originates from papillary thyroid carcinoma rather than differentiated thyroid carcinoma (4). Therefore, the orthotopic model using the TPC1-M cell line can recapitulate poorly differentiated thyroid carcinoma.
We attempted to recapitulate aggressive thyroid cancer in patients using an orthotopic surgical mouse model of microscopic residual tumor (R1 resection). At two weeks post-tumor cell injection, we confirmed tumor formation by palpation and started the drug treatment. After one week of treatment (three injections of echinomycin) in a neoadjuvant therapy setting, an R1 resection was performed, sparing the trachea and the esophagus. Since this surgery was performed as a capsular dissection, it would not be a curative procedure and microscopic disease could remain. Following surgery, the inhibitor treatment was continued as adjuvant therapy for a further week. The survival analysis of this animal model showed significant survival gain for mice treated with combined surgery and echinomycin. Furthermore, surgery alone also improved survival in this model. A recent review of anaplastic thyroid carcinoma cases by the Korean Head and Neck Surgery Society found that patients for whom aggressive treatment (including surgery) was possible showed improved survival (unpublished data). This animal model may indicate that survival could also be improved in patients by gross removal of a tumor and treatment with echinomycin to further improve the surgical outcome.
Barriers still exist to the therapeutic use of HIF1α inhibitors for thyroid carcinoma. LAQ824 was tested in the animal model but was very toxic, and the mice were unable to tolerate the drug toxicity. Echinomycin also had considerable toxicity in mice and daily treatments made mice cachexic (data not shown). Although HIF1α is considered as a good candidate molecule for targeted therapy, especially in an adjuvant setting to reduce recurrence from microscopic remnants, new drugs are needed that can inhibit HIF1α more effectively and with less toxicity.
In summary, the highly significant survival gain resulting from their use in perioperative adjuvant treatment in vivo and their anticancer effect in vitro, suggest that HIF1α inhibitors might be good candidates as perioperative adjuvant chemotherapeutic agents for thyroid cancer; further studies are required to validate their efficacy and safety.
Conclusion
Adjuvant HIF1α inhibitor chemotherapy combined with surgery might be an effective therapeutic strategy for thyroid cancer that is refractory to conventional treatments.
Acknowledgements
This work was supported by grant number 03-2012-013 from the Seoul National University Bundang Hospital Research Fund.
Footnotes
-
Conflicts of Interest
None.
- Received November 9, 2014.
- Revision received January 16, 2015.
- Accepted January 20, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}