


Abstract
Aim: The aim of the present study was to investigate the efficacy and tolerability of vinorelbine and cisplatin for the treatment of patients with advanced (stage IIIB, IV or relapse) non-small cell lung cancer (NSCLC) with interstitial pneumonia (IP). Patients and Methods: A total of 67 patients treated with vinorelbine and cisplatin as a first-line chemo therapy between January 2002 and December 2013 were retrospectively reviewed. Results: The overall response rate was 34.3% [95% confidence interval (CI)=22.9%-45.7%). The median progression-free survival, median overall survival, and 1-year survival rates were 3.7 months (95% CI=3.1-4.3 months), 7.4 months (95% CI=5.4-9.4 months), and 22.4% (95% CI=12.4%-32.4%), respectively. The incidence of acute exacerbation of IP following first-line chemotherapy was 10.4%. Conclusion: The combination of vinorelbine and cisplatin is a feasible treatment option for advanced NSCLC patients with IP, after careful consideration of the potential risks and benefits on an individual basis.
Idiopathic interstitial pneumonia (IP) is a group of progressive fibrotic lung diseases that appears to be increasing in prevalence in many developed countries (1). The incidence of lung cancer in patients with IP is reported to be higher than in the general population, and IP is considered to be a risk factor for lung carcinogenesis (1-6). The clinical course of idiopathic IP is usually chronic; however, it is often complicated by acute exacerbation of IP, i.e. the sudden acceleration of the disease process or acute lung injury superimposed on an already diseased lung. Since no proven effective therapies have been established for acute exacerbation of IP, this clinical condition is associated with a poor prognosis (7, 8). In patients with lung cancer and pre-existing IP, acute exacerbation frequently occurs during anticancer treatments, including chemotherapy (9-12).
To date, only a few reports evaluating the clinical efficacy and safety of chemotherapy for patients with non-small cell lung cancer (NSCLC) with IP have been published, and the optimal chemotherapeutic regimen remains controversial (13-17). The regimens evaluated in these previous studies were platinum-based doublet regimens, and the selected platinum agent was usually carboplatin. Therefore, whether doublet regimens combined with cisplatin are feasible for the treatment of patients with advanced NSCLC with IP remains uncertain.
To evaluate the efficacy and tolerability of the combination of vinorelbine and cisplatin, we retrospectively reviewed a series of patients with advanced NSCLC with IP who underwent this treatment.
Patients and Methods
Patient selection. Between January 2002 and December 2013, a total of 395 patients with NSCLC were diagnosed as having pre-existing IP at the National Cancer Center Hospital East (Chiba, Japan). Among them, we retrospectively identified patients who satisfied the following criteria: histologically- or cytologically-confirmed advanced NSCLC (stage IIIB, IV, or relapse); underwent combination chemotherapy with vinorelbine and cisplatin as a palliative treatment; and did not undergo thoracic radiotherapy. Out of the 395 patients with NSCLC with IP, 189 patients received some form of chemotherapy as a palliative treatment: 81 patients received combination chemotherapy with vinorelbine and cisplatin, and 108 patients received some other regimen. Out of the 81 patients who received combination chemotherapy with vinorelbine and cisplatin, 67 patients had advanced disease. These 67 patients comprised the presently reported study cohort.
The results were analyzed retrospectively using case and radiographic records. Lung cancer histology was defined based on the World Health Organization pathology classification (18). Clinical staging was decided according to the seventh edition of the tumor node metastasis classification of NSCLC (19). IP was diagnosed based on the radiological findings of pre-treatment chest computed tomographic (CT) images, such as the presence of reticular opacities, traction bronchiectasis, or honeycombing. The presence of IP was independently evaluated by at least two pulmonologists. This study was approved by the Institutional Review Board of National Cancer Center Hospital East (approval number: 2014-212).
Patients' characteristics (N=67).
Treatment method. The treatment regimen consisted of vinorelbine at a dose of 25 mg/m2 and cisplatin at a dose of 80 mg/m2. Cisplatin was administered on day 1, and vinorelbine was administered on days 1 and 8. Each 3-week treatment schedule was designated as one cycle. Dose reduction, omission, and the discontinuation of chemotherapy were performed at the physician's discretion. The therapy was continued for up to four cycles or until disease progression, the appearance of intolerable toxicity, or the patient's refusal to undergo further therapy.
Evaluation of response and toxicity. The objective tumor response was assessed based on the Response Evaluation Criteria in Solid Tumors (RECIST) guidelines, version 1.1 (20). The objective response rate (ORR) was calculated as the total percentage of patients with a complete response (CR) or a partial response (PR). The disease control rate (DCR) was calculated as the total percentage of patients with CR, PR, or stable disease (SD). Toxicity was graded according to the Common Terminology Criteria for Adverse Events, version 4.0 (21). Regarding pulmonary toxicity, acute exacerbation was defined if all of the following criteria were satisfied: unexplained worsening or development of dyspnea within one month; new bilateral ground-glass opacities and/or consolidation superimposed on a background reticular or honeycomb pattern on CT; and exclusion of all obvious causes of these changes, such as infection, pneumothorax, pulmonary embolism or congestive heart failure (8).
Statistical analyses. Data are presented as counts or the median values with ranges. The median progression-free survival (PFS) and overall survival (OS) were estimated using the Kaplan-Meier Method. The PFS and OS were measured from the date of initiation of the first-line chemotherapy until the date of disease progression or death from any cause for PFS and until the date of the last follow-up, death, or the final follow-up day of the study for OS. Survival was assessed up until October 1, 2014.
Response to first-line chemotherapy.
Adverse events other than acute exacerbation of interstitial pneumonia.
Results
Patients' characteristics. The baseline characteristics of the 67 consecutive patients are shown in Table I. The median age was 64 years (range=47-76 years). Male patients (95.5%), and patients with an Eastern Cooperative Oncology Group Performance Status (PS) of 0 or 1 (95.5%) were predominant. All patients were current or former smokers. Histologically, adenocarcinoma, squamous cell carcinoma, and non-small cell lung cancer (not otherwise specified: NOS) were observed in 38.8%, 31.3%, and 25.4% of the patients, respectively. All patients had advanced disease: 20 (29.9%) had stage IIIB disease, 42 (62.7%) had stage IV disease, and 5 (7.5%) had recurrent disease. In none of the patients was IP histologically confirmed.
Treatment efficacy and survival. Table II summarizes the treatment outcome of first-line chemotherapy. Among the 67 patients, 23 had PR and 26 had SD, yielding an ORR of 34.3% [95% confidence interval (CI)=22.9%-45.7%) and a DCR of 73.1% (95% CI=62.9%-83.3%). Regarding treatment delivery, the median number of applied first-line chemotherapy cycles was 3 (range=1-4 cycles). A total of 34 patients had received second-line treatment, and seven patients had received third-line or later treatment. None of the patients had received maintenance chemotherapy.
Comparison to previous reports on chemotherapy for patients with non-small cell lung cancer with interstitial pneumonia.
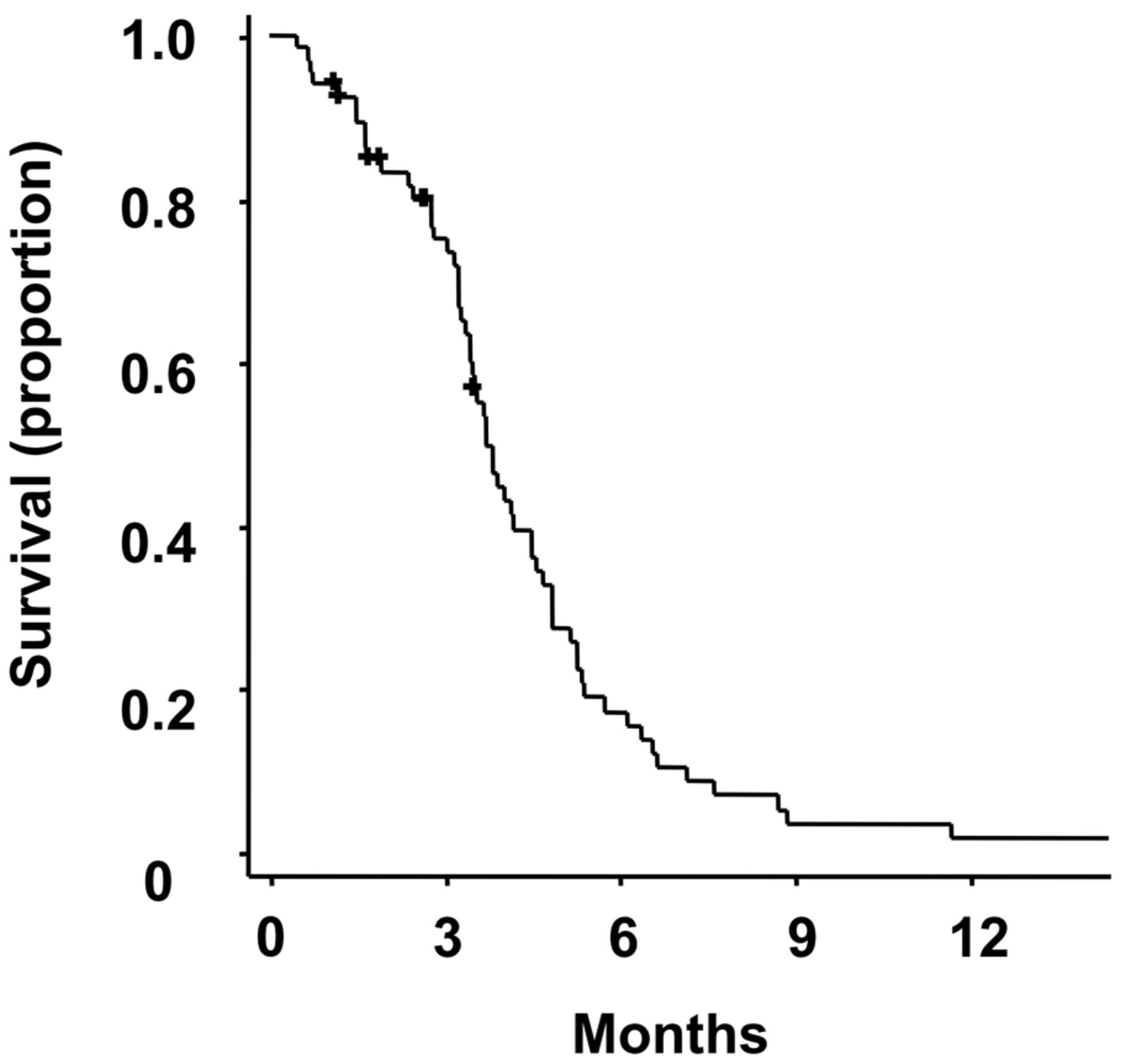
Kaplan-Meier plot of progression-free survival (PFS). The median PFS was 3.7 months (95% confidence interval=3.1-4.3 months).
At the time of analysis, the median follow-up duration for the surviving patients was 7.2 months (range=1.2-63.2 months). The median PFS on first-line chemotherapy was 3.7 months (95% CI=3.1-4.3 months) (Figure 1). The median OS was 7.4 months (95% CI=5.4-9.4 months), and the 1-year survival rate was 22.4% (95% CI=12.4%-32.4%) (Figure 2). A total of 60 patients (89.6%) had experienced disease progression and 60 patients (89.6%) had died at the time of data cut-off.

Kaplan-Meier plot of overall survival (OS). The median survival time was 7.4 months (95% confidence interval=5.4-9.4 months) and the 1-year survival rate was 22.4% (95% confidence interval=12.4%-32.4%).
Toxicity. The toxicities of the treatment other than acute exacerbation are summarized in Table III. The most common hematological grade 3 or 4 adverse event was neutropenia (60%). Infection was the most common non-hematological grade 3 or 4 adverse event, occurring in 16% of the patients.
A total of seven patients (10.4%) developed acute exacerbation of IP during first-line chemotherapy, and all patients died from acute exacerbation of IP. The median time from the final treatment until the development of acute exacerbation of IP was 24 days (range=5-62 days), and the median survival time from the onset of acute exacerbation of IP was 16 days (range=2-55 days).
Discussion
This is the first study, to the best of our knowledge, in which the therapeutic benefit and the tolerability of cisplatin-based chemotherapy regimen for the treatment of patients with advanced NSCLC with IP were evaluated. Vinorelbine was the first third-generation agent to demonstrate a statistically significant survival benefit when combined with cisplatin over a second-generation agent (vindesine) plus cisplatin (22). Therefore, this combined regimen has been one of the established treatment options for patients with advanced NSCLC for a number of years.
In the present study, the ORR to first-line chemotherapy, the median PFS, and the median OS were 34.3%, 3.7 months, and 7.4 months, respectively. These results were similar to those observed in previous studies for patients with advanced NSCLC with IP (Table IV) (13-17). Furthermore, the ORR and the median PFS were equivalent to those of a treatment group that received vinorelbine plus cisplatin in a previous Japanese randomized phase III study of advanced NSCLC without IP [For-Arm Cooperative Study (FACS): ORR=33.1%, median PFS=4.1 months] (23). Nevertheless, the median OS in our study was unsatisfactory for patients without IP. We speculate that the reasons for the difference between the unsatisfactory median OS and the comparatively good ORR in our study might be as follows. Firstly, several patients experienced acute exacerbation of IP, and the prognosis after the onset of exacerbation was very poor. Secondly, the rate of second-line or later treatment was lower than that in the above-mentioned phase III study. Our patients might have had a decreased performance status during chemotherapy because of the functional limitation and respiratory impairment caused by IP. Consequently, the rate of second-line or later treatment might have been lower. Thirdly, the treatment options for patients with NSCLC with IP are limited, compared to those for patients without IP. In particular, the use of epidermal growth factor receptor tyrosine kinase inhibitor is not recommended for patients with IP because of the greater risk of developing acute interstitial lung disease, compared to cytotoxic chemotherapy, despite the fact that this is a well-established therapy for the treatment of NSCLC worldwide (24).
In patients with NSCLC with IP, acute exacerbation frequently occurs during chemotherapy and results in a fatal outcome. Previous studies in patients with NSCLC with IP have found that acute exacerbation is associated with first-line chemotherapy at rates of 5.6% to 26.7% (Table IV) (13-17). In the present study, the rate of patients who developed acute exacerbation of IP associated with first-line chemotherapy (7/67 patients: 10.4%) was equivalent to or lower than the rates of previous studies. Recently, the occurrence of acute exacerbation during the normal course of IP has come to be widely known, with reported incidences ranging between 4.8% and 13.9% within one year in prospective trials (25, 26). In retrospective studies, the 1-year frequency of acute exacerbation of IP was reported to be around 10% (27, 28). Based on the comparable incidence of acute exacerbation of IP to that in the natural course of IP, the combination of vinorelbine and cisplatin might be of acceptable toxicity and feasible for the treatment of patients with advanced NSCLC with IP.
Several limitations of this study should be mentioned. Firstly, the study was a retrospective, non-randomized study performed at a single Institution. Secondly, the diagnosis of pre-existing IP was based on radiographic findings, and not on histological findings. Thirdly, this study included only Japanese patients. Whether our results can be applied to other ethnicities should be investigated.
In conclusion, our current results suggest that the combination of vinorelbine and cisplatin might be a feasible and effective option for the treatment of patients with advanced NSCLC with IP. Considering the fact that the occurrence of acute exacerbation of IP following chemo therapy is a fatal complication, greater care is required when administrating this combined therapy for patients with NSCLC with IP. Further well-controlled prospective studies are warranted.
Acknowledgements
This work was supported in part by a Grant-in-Aid for Cancer Research from the Ministry for Health, Labour and Welfare, Japan.
- Received November 4, 2014.
- Revision received November 11, 2014.
- Accepted November 14, 2014.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Lung cancer in patients with fibrosing interstitial lung diseases: an overview of current knowledge and challenges
- Acute exacerbation of idiopathic interstitial pneumonias related to chemotherapy for lung cancer: nationwide surveillance in Japan
- Re-administration of Chemotherapy in Patients with Advanced Non-small Cell Lung Cancer Who Recovered from Chemotherapy-induced Interstitial Lung Disease