


Abstract
Background/Aim: Although targeted-therapy (TT) for patients with metastatic renal cell cancer (mRCC) has shown an improved outcome, their prognosis is still very poor. Immunotherapy with dendritic cells (DC) as one promising new treatment tries to fight cancer by boosting the patient's own immune system. The present analysis matches two different methods of treatment against mRCC, namely sequential TT versus DC vaccine therapy, by comparison of long-term overall survival (OS). Patients and Methods: Data of patients treated with DC vaccines (N=30) in three clinical phase I/II trials (1999-2003) and patients treated with clinical standard targeted-therapy (N=30) at the University Hospital of Bonn (2010-2013) were analyzed regarding their OS, as well as specific characteristics such as number and localization of metastatic sites. Results: The mean OS from the first treatment was significantly higher in the TT than in the DC group (48 versus 21 months, range=3-85 months versus 1-57 months, respectively; p=0.0002). Patients with one (p=0.036) or two metastases (p=0.037) and especially patients with bone metastases (52 versus 12 months; p<0.0001) benefited significantly from TT. However, there was no significant difference between therapy types in patients with lung (p=0.147) or liver (p=0.745) metastases, or in patients with more than two metastatic sites (p=0.074). Conclusion: Targeted therapy is an effective treatment against mRCC, but is limited due to common adverse events and a higher toxicity when combinations of different-targeted agents are used. Immunotherapy with DC vaccines seems to be a potent and well-tolerated therapy against mRCC, possibly showing higher benefit for patients with specific sites of metastasis, and should be investigated as a co-treatment with TT in further studies.
Renal cell carcinoma (RCC) represents 2-3% of all malignant tumors in adults and nearly 90% of all kidney cancers (1). Recent epidemiological analyses of kidney cancer in Germany revealed about 9,000 new cases for men and 5,500 for women in 2010, with an average age at-diagnosis of 68 years for men and 71 years for women. Three quarters of new cases of kidney cancer are diagnosed in early stages (T1 and T2) and the relative five-year survival rate is approximately 75% (2).
Localized tumors are primarily treated with surgical resection (partial or radical nephrectomy) aimed at curing the patient (3). Nevertheless approximately one third of those patients suffer a relapse. An additional 20-30% of RCC cases already exhibit metastatic sites (mRCC) at first diagnosis (4).
In cases of mRCC, overall survival (OS) decreases considerably to a five-year survival rate of less than 10% and indicates the need for a systemic therapy (5). Due to multi-drug resistance, conventional chemotherapies are ineffective against mRCC, which led to a rise in demand for other therapy forms. After an era of immunotherapy characterized by interleukin-2 and interferon-α therapy, targeted-therapy (TT) revolutionized mRCC-treatment in the past eight years. Today, there are seven approved targeted-agents regarded as standard therapy for mRCC: the monoclonal antibody to vascular endothelial growth factor (VEGF) bevacizumab; the VEGF receptor tyrosine kinase inhibitors (VEGFr-TKIs) sunitinib, pazopanib, sorafenib and axitinib; as well as the mammalian target of rapamycin (mTOR) inhibitors everolimus and temsirolimus (6, 7). All of them have been shown to improve treatment outcome and enhance life-quality in first- or second-line therapy; however, complete responses are rare and adaptive resistance, as well as various side-effects, limit their benefit (8). In cases of disease progression or toxicity, a switch to a different targeted-drug (sequential treatment with multiple lines of targeted agents) can be indicated to sustain clinical benefit (9).
Patient characteristics by study group.
Although TT can extend progression-free survival (PFS) and OS, it has reached its plateau and is still only palliative. Other therapy forms against mRCC are being researched, including vaccine immunotherapy with dendritic cells (DC) or tumor peptides as promising new treatments, which try to fight cancer by boosting the patient's own immune system. DCs are potent antigen-presenting cells which activate a primary immune response against tumor cells, mainly via T-cell response. Using these physiological mechanisms, toxicity is only seen in sporadic cases (10, 11).
This analysis matches sequential treatment with targeted-agents, today's clinical standard therapy, against DC vaccine therapy, by comparison of long-term OS from the day of first treatment and day of first diagnosis. DC therapy is represented by three clinical phase I/II trials with autologous or allogeneic DCs fused in vitro with tumor-specific material (12).
Number of therapy lines and the drugs applied in the targeted therapy group.
Long-term survival from the day of first diagnosis and treatment in patients treated with targeted and dendritic cell therapy.
Patients and Methods
In total, this analysis contains data of 60 patients with mRCC separated into two different therapy groups. On the one hand, 30 patients who received vaccine therapy treatment with DCs and on the other hand 30 patients who were treated with sequential targeted therapy, today's standard therapy (Table I).
The DC group is based on three clinical phase I/II trials which took place between 1999 and 2003 (12). The first trial investigated therapy with tumor lysate-pulsed autologous DC vaccines (13), the second trial made use of DCs fused with allogeneic or autologous renal tumor cells (14). The last trial utilized DCs pulsed with human telomerase reverse transcriptase peptide (15). All of them have in common that the DC vaccination was used for patients who had mRCC with a Karnofsky score between 60-100% and an age greater than 18 years. In 14 cases, cytokine treatment was administered at least 28 days before the first vaccination. The pulsed DCs were injected in intradermal, intranodal, subcutaneous or intratumoral form. More details are given in the quoted references (12-15).
The TT group included data of 486 patients with RCC treated at the University Hospital of Bonn, Germany, from January 2010 to July 2013. After selecting for patients characterized by advanced RCC, treatment with TT and age greater than 18 years, and excluding any persons with additional experimental therapy forms or lacking data, 30 patients remained. Furthermore these patients were matched with the DC group, which was limited to 30 patients, regarding age at diagnosis, tumor stage and number of sites of metastasis.
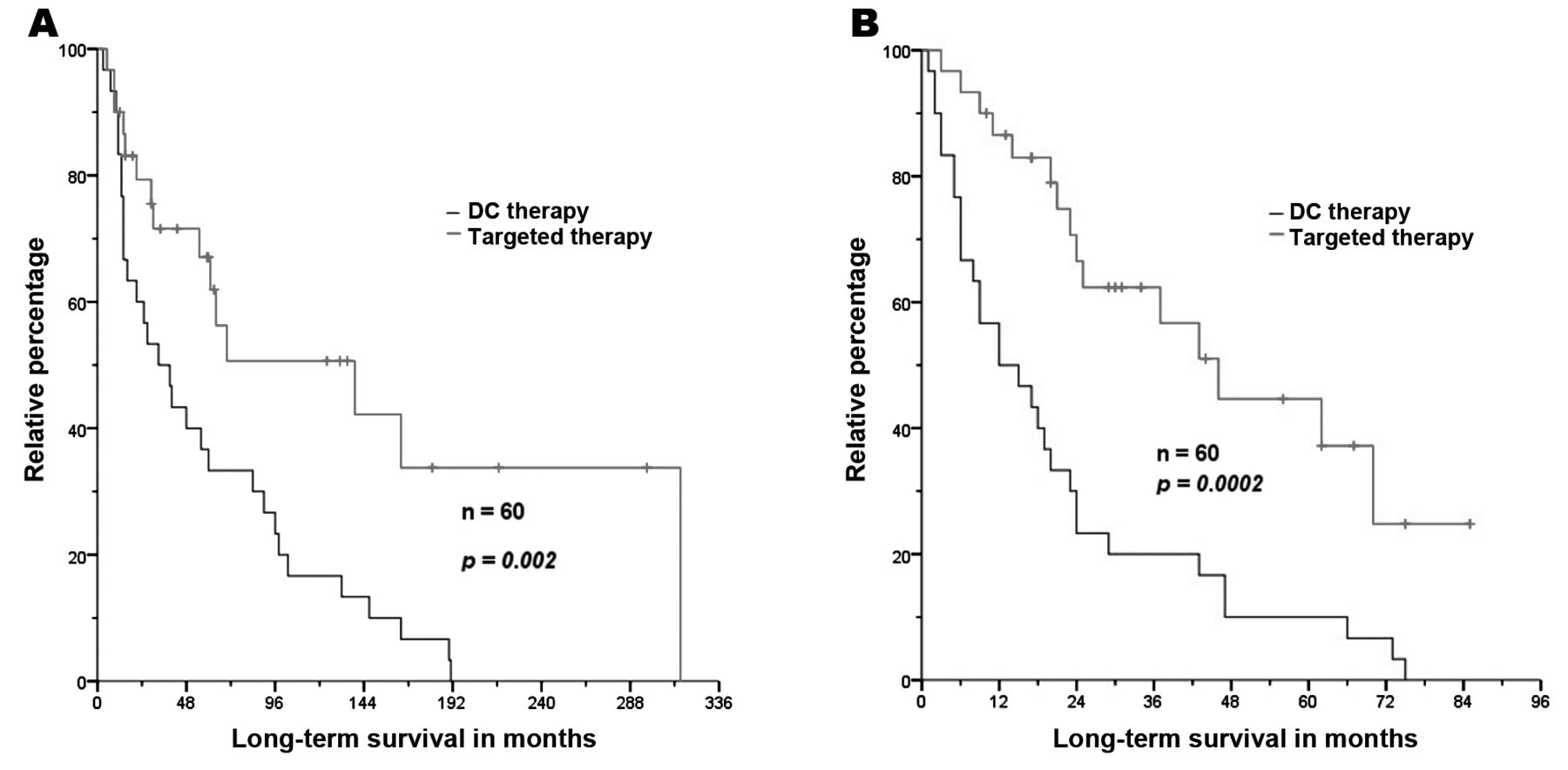
Long-term survival from the day of first diagnosis (A) and treatment (B) in patients treated with targeted agents or dendritic cell (DC) vaccine therapy.

Long-term survival from the day of first treatment in patients treated with single or multiple lines of targeted therapy (TT) or with dendritic cell (DC) vaccine therapy.
Treatment with TT was defined as therapy with at least one of the seven approved targeted agents, predominantly given in different sequences because of rising resistance, tumor progress or side-effects. The most widely used drugs in first-line were sunitinib (50%) and pazopanib (27%), in second-line sorafenib (38%) and everolimus (25%), and in third-line everolimus (30%) and sunitinib (25%). Two in every three patients were treated with more than two therapy lines (Table II).
At first diagnosis of RCC, metastases already existed in 17 cases in the TT group and in 16 cases in the DC group. Lung and bone metastases were found in about every second case in both groups, whereas liver metastases were more frequent in the DC group. As a consequence of differences in treatment dates between the groups, all 30 patients in the DC group died, while 15 patients in the TT group died and the remaining 15 were still under medical treatment at the time of data collection (Table I).
Long-term survival was determined from the day of first diagnosis and the day of first treatment until point of death and is presented using Kaplan-Meier curves calculated by SPSS Version 22.0.0.0 (SPSS Inc., Chicago, IL, USA).
Primary end-points of this analysis were long-term OS from the day of first diagnosis and the day of first treatment based on two different therapy groups: today's clinical standard sequential TT and experimental DC vaccine therapy.
Results
Four patients in the DC group received more than one vaccination because of their participation in several of the aforementioned clinical trials. The initial 33 patients of the TT group were reduced to 30 patients since one patient participated in the ASET study and the other two lacked data their documentation of therapy. Due to the fact that 15 patients in the TT group were still receiving medical treatment at the time of analysis, they are included as censored cases in this analysis.

Long-term survival from the day of first treatment with targeted agents or dendritic cell (DC) vaccine therapy in patients younger (A) and older (B) than 60 years.
The mean OS from initial diagnosis was significantly (p=0.002) higher in the TT group, at around 150 versus 59 months in the DC group (Figure 1A). The range was between 5 to 315 and 3 to 191 months, respectively (Table III). Because five patients of the TT group had an extremely late relapse (an interval of at least eight years between first diagnosis of RCC with consequent nephrectomy and occurrence of the first metastasis), the mean OS since first treatment should be more relevant than the data since first diagnosis. The survival time since first treatment was significantly (p=0.0002) different between the groups, ranging from 3 to 85 months in the TT group and 1 to 57 months in the DC group, with a mean survival of 48 months regarding TT versus 21 months regarding DC therapy (Figure 1B, Table III). In addition, the TT group was separated into subgroups of single and multiple TT and compared to the DC group, resulting in patients significantly benefiting from multiple (48 versus 21 months; p=0.001), as well as from single TT (46 versus 21 months; p=0.048) (Figure 2).
Analyzing both groups with regards to age, namely being younger or older than 60 years, shows that TT had an advantage (p<0.0001 and p=0.028, respectively) over DC vaccine therapy in both cases (Figure 3).
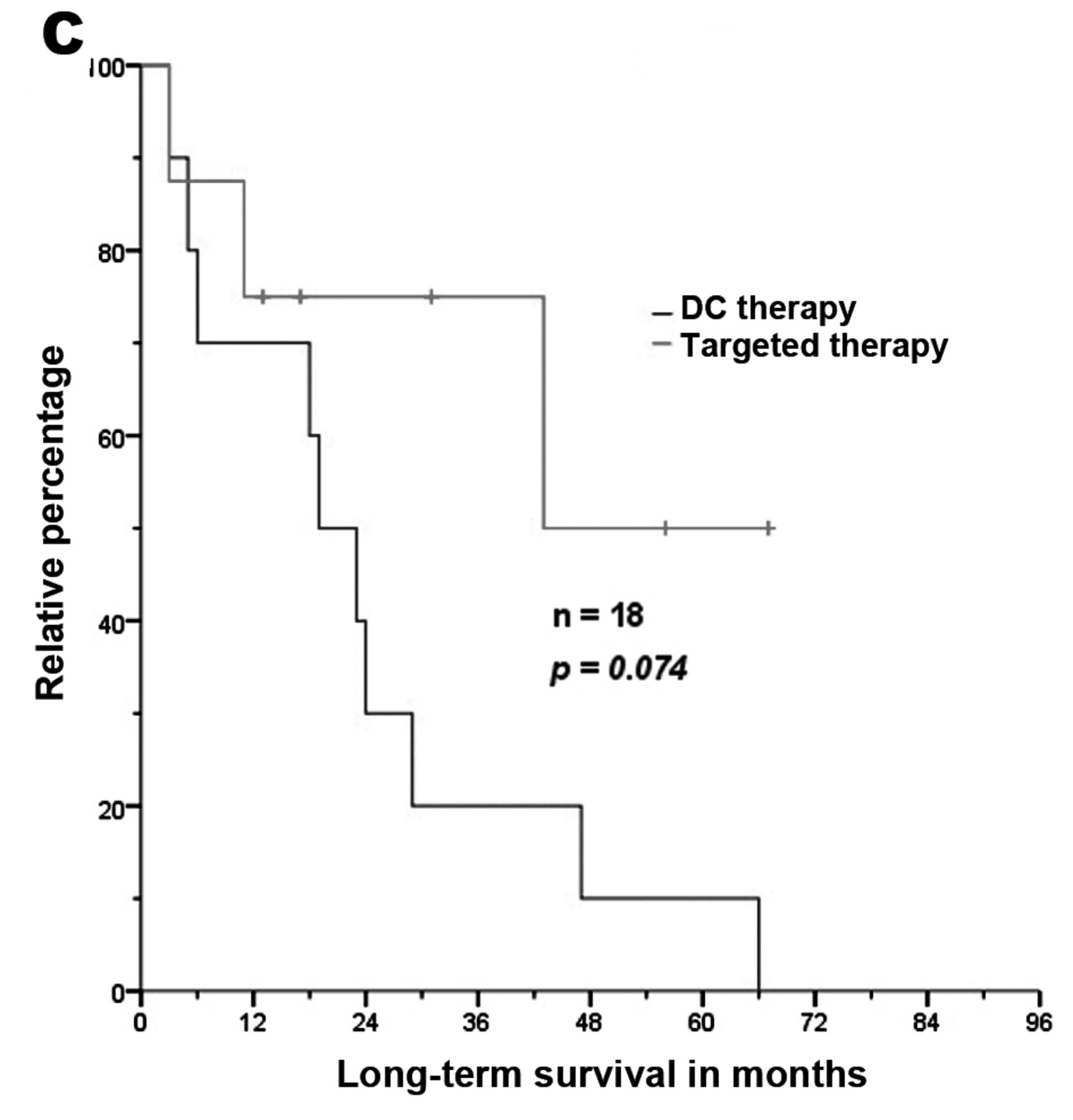
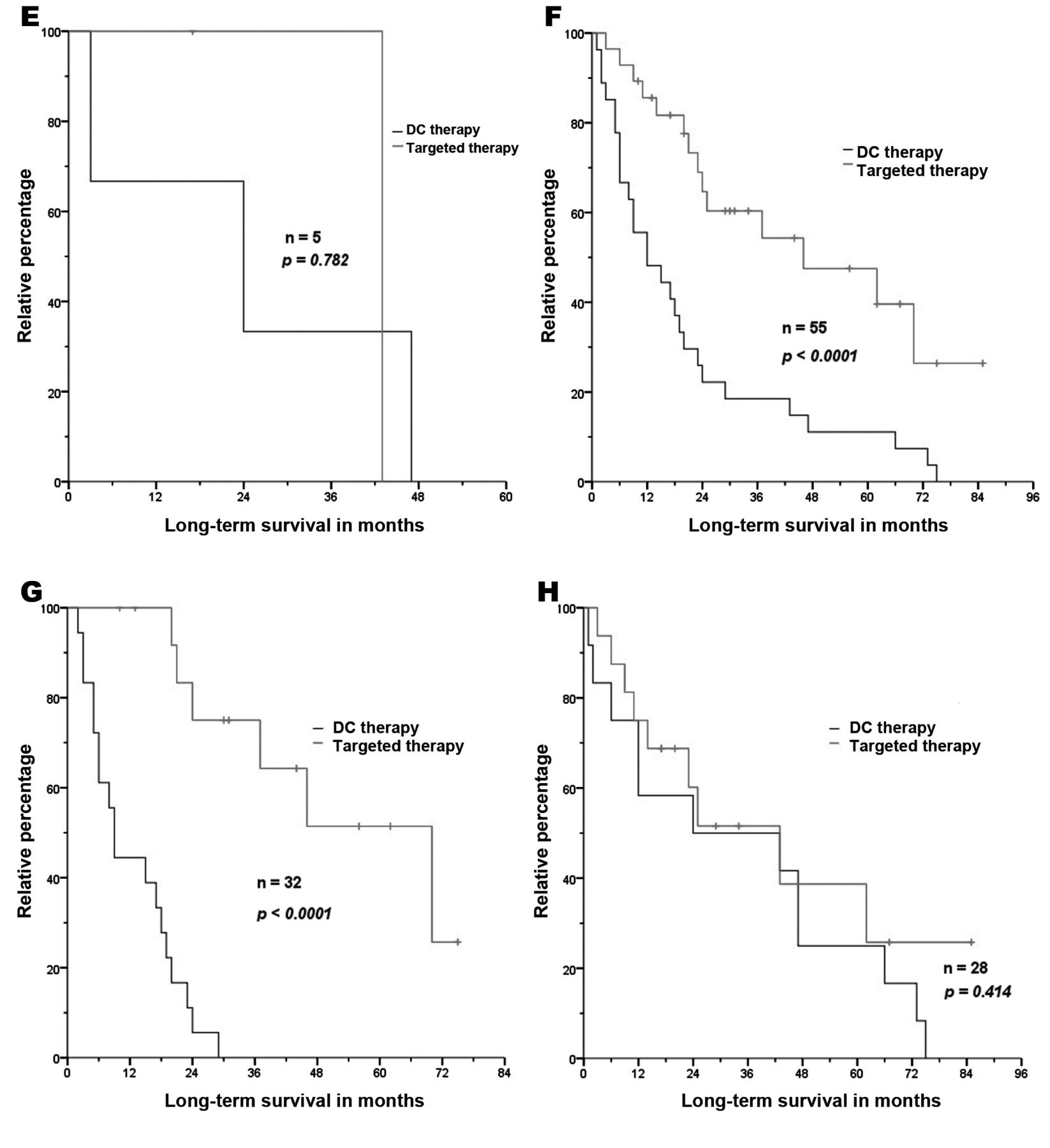
Furthermore, the two therapy forms were analyzed concerning OS dependence on pre-existing number and type of metastases, particularly pulmonary, liver, bone and brain metastases. Referring to the number of sites of metastases there was a significant benefit of TT in patients with one (p=0.036) or two metastases (p=0.037), but no significant (p=0.074) difference between therapy forms in patients with more than two sites (Figure 4). Figure 5A shows that there was no considerable difference (p=0.147) between the groups for patients with lung metastases. Even for patients with liver metastases, the disparity is not significant (p=0.745) (Figure 5C). The same (p=0.782) applies to the admittedly minor group of patients with brain metastases (Figure 5E). Notably, the survival curve twisted resulting in non-significant (p=0.287) advantage for the DC group when patients who had both pulmonary and liver metastases were analyzed (Figure 6). There was, however, a major difference for patients with bone metastases, revealing a remarkable benefit (52 versus 12 months; p<0.0001) for patients after TT (Figure 5G).
Discussion
The ultimate aim of this analysis was the comparison between today's clinical standard TT and the experimental DC vaccine therapy.
Nowadays, sequential TT with multiple use of VEGFr-TKIs or mTOR inhibitors is the established clinical first-line treatment, yet there are currently only a few randomized trials available which investigated the ideal sequence or combination of targeted-drugs to achieve maximum clinical benefit (16). Today, sequential use of targeted-drugs has raised OS of patients with mRCC by 40 months and more (17). Data for the TT group with up to five lines of therapy revealed a mean OS of 48 months (Figure 1B; Table II). This positive outcome is probably the result of continuous treatment by consequent switching to another TKI or mTOR inhibitor in cases of intolerance or drug resistance (18).


Long-term survival from the day of first treatment with targeted agents or dendritic cell (DC) vaccine therapy in patients with one (A), two (B) or more than two (C) sites of metastasis.
Therapy with DC vaccines as an experimental form of immunotherapy seems to be a potent and safe treatment for mRCC. Several phase I and II trials showed that DC vaccines reliably induce an immune response against cancer cells and may reduce tumor mass without any severe adverse events (11). Due to the multitude of different vaccines and the current lack of phase III trials, these results should be noted cautiously. Findings in the DC vaccine trials, which are presented in this analysis, nonetheless confirm those aspects regarding outcome and tolerance (12).
The comparison between groups revealed a significant benefit for the TT group (48 versus 21 months; p=0.0002). Interestingly, the mean OS for patients with particular metastatic sites, namely the lung and liver, showed no significant difference by therapy group. In fact, considering patients who had both pulmonary and hepatic metastases, the curve twisted, leading to a non-significant advantage for DC therapy (29 versus 15 months; p=0.247). In patients with an especially high number of metastatic sites (more than two), DC therapy also seemed to be similar regarding patient benefit (p=0.074). For patients with bone-metastatic sites however, TT was significantly better than DC treatment (53 versus 12 months; p<0.0001).
In terms of side-effects, DC therapy seems to be very well tolerated (10, 13-15), whereas treatment with targeted drugs is frequently accompanied by adverse events such as hypertonia, hand-foot syndrome, fatigue, nausea, diarrhea and others (19). Moreover, when combinations of two targeted-agents were used at the same time, it commonly led to an increase in adverse events without an improvement in treatment outcome in several trials (20-22). Co-treatment with temsirolimus-plus-interferon as immunotherapy showed no significant benefit either (23). Changing the sequence by making use of alternative TKIs or mTOR inhibitors remains the only available strategy to avoid intolerance or resistance and guarantee continuous treatment. The almost complete absence of adverse events in DC therapy obviously suggests combining both therapy forms to achieve a synergistic effect and increase treatment outcome. First studies based on the AGS-003 DC vaccine showed there were no additive side-effects when DC therapy and TT were used as co-treatment (24). However, well-designed, randomized phase III trials are not available at the present time, but are anticipated in the near future, e.g. ADAPT [AGS-003 (24) plus sunitinib]. Even so, treatment of advanced RCC with today's available TT or DC vaccines will still be palliative and linked to a poor prognosis. Therefore different molecular therapeutic approaches apart from VEGFr-TKIs or mTOR pathways are required. Inhibitors of the Wingless-type signaling pathway in combination with a bi-functional peptide revealed significant reduction of cancer cells in vitro and should be investigated in further trials (25).


Long-term survival from the day of first treatment with targeted agents or dendritic cell (DC) vaccine therapy in patients with pulmonary metastases (A), metastases other than pulmonary (B), liver metastases (C), metastases other than of the liver (D), brain metastases (E), metastases other than of the brain (F), bone metastases (G) and metastases other than to bone (H).

Long-term survival from the day of first treatment with targeted-agents or dendritic cell (DC) vaccine therapy in patients with both pulmonary and liver metastases.
- Received November 4, 2014.
- Revision received November 11, 2014.
- Accepted November 17, 2014.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.