


Abstract
Aim: The objectives of our explorative study were to (i) evaluate the immunohistochemical expression of sex steroid hormone receptors (estrogen receptor a [ERα], estrogen receptor β [ERβ], progesterone receptor [PR] and androgen receptor [AR]), angiogenesis factors (vascular endothelial growth factor [VEGF] and inhibitor of differentiation/DNA synthesis 1 [Id-1]) and cell-cycle regulators (cyclin D1, p16 and p27) in intraductal papillary mucinous neoplasms (IPMNs) in comparison to normal adjacent pancreatic tissues and (ii) assess their correlation with the grade and histological sub-type of those lesions. Materials and Methods: Paraffin-embedded specimens from 12 consecutive patients with IPMNs were immunostained for the studied markers and staining quantification was assessed by an image analysis system. Results: AR H-score and cyclin D1 H-score were significantly higher in the IPMN lesions (0.86±0.33 vs. 0.57±0.12 in the normal tissue, p=0.010 and 0.47±0.23 vs. 0.21±0.20 in the normal tissue, p=0.019, respectively). No significant differences were noted regarding the expression of ERα, ERβ, PR, p16, p27, VEGF, Id-1 or MVD. Moreover, no significant associations were found between the expression of studied markers and grade or histological subtype. Conclusion: Our study showed higher expression of AR and cyclin D1 in IPMNs compared to normal pancreatic ducts without any association between AR and cyclin D1 expression and IPMNs' grade or subtype.
Intraductal papillary mucinous neoplasms (IPMNs) are exocrine tumors of the pancreas that develop into the main or branch ducts and are predominately composed of papillary structures lined by mucin-producing atypical epithelium (1). IPMNs are considered to exhibit a pattern of progression similar to the adenoma-carcinoma sequence seen in colorectal adenocarcinoma. The 2010 WHO classification, sub-categorizes IPMNs according to the degree of cytologic atypia into IPMNs with low, intermediate and high-grade dysplasia. If an invasive carcinoma is also present the term IPMN with an associated invasive carcinoma is applied (2, 3). Further sub-division of IPMNs has been achieved on the basis of differences in mucin expression profiles, cytologic appearance and architecture. These histologic subtypes have differing probabilities of progression to malignancy and have been designated as gastric foveolar, intestinal, pancreatobiliary and oncocytic (4). Gastric-type IPMNs typically exhibit low-grade dysplasia, whereas intestinal-type show more often intermediate or high-grade dysplasia. Pancreatobiliary, as well as oncocytic are less common IPMN-types and characterized by high-grade dysplasia, considered to have high malignant potential (4).
The sex steroid hormones (estrogens, progesterone and androgens) exert their effects through binding to their cognate receptors, estrogen receptors (ER), progesterone receptors (PR) and androgen receptors (AR), respectively. Only four studies have studied ER and PR expression on IPMNs without using, however, isoform-specific antibodies for ERα and ERβ (5-8). Three of them studied those receptors' expression on tumor cells (6-8), whereas the other examined their expression on stromal cells in IPMNs cyst wall. AR expression on IPMNs has never been studied.
Vascular endothelial growth factor (VEGF) has been identified as key mediator of the regulation of pathologic blood vessel growth and maintenance, inducing also endothelial cell proliferation and enhancing vascular permeability (9). However, the significance of VEGF in IPMNs neoangiogenesis and progression has still been scarcely studied (10, 11). The inhibitor of differentiation/DNA synthesis 1 (Id-1) has been shown to play a pivotal role in cell proliferation, differentiation and senescence (12). Over-expression of Id-1 has been correlated with high tumor aggressiveness (13), tumor metastasis and angiogenesis (13). Given the absence of any research on Id-1 expression in IPMNs, it seems of great interest to elucidate whether over-expression of Id-1 promotes IPMNs' angiogenesis and evolution. Microvessel density (MVD) is an established method for quantitatively examining angiogenesis in tumors (14). A number of endothelial surface markers, such as CD34, CD31 and factor VIII, have been used to examine MVD in various tumors.
Cell cycle is regulated by changes in the levels and activities of several cyclins, cyclin-dependent kinases (CDKs) and their inhibitors. Cyclin D1 (CCND1) is a well-established human oncogene; over-expression of cyclin D1 in IPMNs has been reported by a number of authors (15-18). However, none of these correlated cyclin D1 over-expression with IPMNs' histological subtype or degree of dysplasia. P27Kip1 (p27), a member of the Cip/Kip family, is a universal CDK inhibitor (19). Loss of expression or down-regulation of the p27 protein in IPMNs has been examined in two studies (18, 20). Both failed to trace any association with dysplasia's degree and IPMNs' architectural pattern. On the other hand, the tumor suppressor gene P16INK4A, encoding the CDK inhibitor p16, is reportedly inactivated in more than 90% of pancreatic ductal adenocarcinoma (PDAC) and is thought to represent an intermediate genetic alteration in the progression of those neoplasms (21). Its loss of expression on IPMNs has been investigated by a few researchers (7, 15, 18, 22-24); nevertheless, only two studies demonstrated correlation of p16 loss of expression and degree of dysplasia (18, 24).
Taking the available literature as a whole, the immunohistochemical expression of sex steroid hormone receptors, angiogenesis factors (VEGF and Id-1) and cell-cycle regulators (cyclin D1, p16 and p27) in IPMNs are poorly investigated. The objectives of our explorative study were to: (i) evaluate the expression of those markers in IPMNs in comparison to normal adjacent pancreatic tissue and (ii) assess their correlation with the grade and histological subtype of those lesions.
Materials and Methods
Patients and tissue samples. After approval from the Ethics Board, 12 consecutive cases of surgically removed IPMNs between December 1999 and July 2004 were obtained from the Division of Pathology at “Eugenidio” General Hospital (Athens, Greece). Whipple pylorus preserving procedure (n=6), distal (n=4) and total pancreatectomy (n=2) for IPMNs of the pancreas were performed by a single surgeon. Haematoxylin and eosin sections were examined and the IPMNs were graded according to current WHO criteria by two experienced pathologists (AL and SS). Tissue blocks that contained IPMNs and adjacent normal tissue were selected for the study.
Immunohistochemical staining. One formalin-fixed, paraffin-embedded block was selected for analysis for each patient's case. Tissue blocks were sectioned into 3.5 μm and placed in 56°C overnight. The next day, they were placed in PT Link (device for deparaffinization, rehydration and epitope retrieval; Dako, Denmark) with Tris/EDTA buffer, pH 9. After having been washed in water, slides were incubated in 3% hydrogen peroxide for 10 min in a dark room to block endogenous peroxidase activity and then rinsed with water and Tris-buffered saline and Tween 20 (TBST). The sections were incubated overnight at 4°C (at least for 10 h) with the primary antibodies listed in Table I. The next day, they were left for 30 min at room temperature and rinsed with TBST followed by incubation with rabbit HRP-labeled polymer (Envision + System-HRP, DakoCytomation, Glostrup, Denmark) for 45 min. Slides were immersed in TBST for 5 minutes three times each and then chromogen DAB-Ni or DAB (Table I) was placed for 5 min and rinsed afterwards with TBST three times. Light green or hematoxylin (Table I) was used as a counterstain, placed for 40 sec and washed with abundant water afterwards. Finally, tissue sections were dehydrated with graded alcohols, cleared with xylene and coversplipped with GLC mounting medium. All cases were stained simultaneously with appropriate specimens, which served as positive controls. For negative controls, primary antibodies were omitted and corresponding preimmune animal serums (rabbit or mouse) were used instead.
Image acquisition. Evaluation of immunohistochemical results was performed using an image analysis system known as Image Pro Plus Media Cybernetics, version 6 (Media Cybernetics, Inc., Rockville, MD, USA). After thorough examination of each immunohistochemical slide at a low power magnification (using 4× objective lens) by two experienced pathologists (SS and AL), three representative pictures of the IPMN areas and adjacent normal ducts were acquired (SC30 Olympus Camera, Tokyo, Japan) and stored as jpeg files with consecutive numbers. For the VEGF, Id-1 and MVD evaluation, however, three representative pictures of IPMN areas and adjacent normal ducts, ×200 field each, were acquired and stored as above. The details of the scanning technique and intensity quantification are available on the manufacturer's Web site (http://www.mediacy.com).
Primary antibodies used in the study.
For the purpose of immunohistochemical analysis, we selected the IPMN foci in each picture and each focus was quantified separately by the analysis system for nuclear staining intensity (0-3) and percentage of positively staining nucleus (0%-100%) (Figure 1) for nuclear stainings (ERα, ERβ, PR, AR, cyclin D1, p16, p27). We followed the same process with regard to normal pancreatic ducts. The H-score, which is a method of assessing intensity in combination with percentage of nuclear immunoreactivity, was obtained by the image analysis system automatically by the formula: 3 × percentage of strongly staining nuclei + 2 × percentage of moderately staining nuclei + percentage of weakly staining nuclei, giving a range of 0 to 3. For VEGF and Id-1 evaluation, the analysis system quantified staining intensity (0-3) and percentage of positively staining cells (0%-100%) with regard only to cytoplasmic expression for IPMNs and normal pancreatic ducts foci. The Positive Activity Index (PAI), a numerical representation of staining intensity and distribution in the specimen, was obtained by the image analysis system automatically by the formula: 3 × percentage of high staining activity intensity + 2 × percentage of medium staining activity intensity + percentage of low staining activity intensity, giving a range of 0 to 3.
To quantify angiogenesis, MVD was assessed by immunostaining with the anti-CD34 antibody as described above. Slides were examined carefully at a low power magnification (×40) to identify the areas with the highest density of capillaries and small vessels in IPMN lesions and normal pancreatic duct areas. In each case, the three most vascularized areas (hot spots) were selected and a ×200 field was stored as a JPEG file. Single endothelial cells or clusters of endothelial cells positive for CD34 were considered as individual vessels. In each vessel, the outline was identified and traced. The presence of blood cells or fibrin without any detectable endothelial cells was not sufficient to define a microvessel. Areas with a dense leukocytic or hemorrhagic infiltration were excluded. MVD was measured automatically by the image analysis system and defined as the mean value of counts from the three hot spots converted to 1 mm2.
Every slide was also blindly evaluated by two experienced pathologists (SS and AL). The results did not statistically significantly differ compared to those obtained by the image analysis system.
Statistical analysis. Given the marked deviation from normality of the H-scores and PAIs (as attested by the Shapiro-Wilk test), non-parametric statistical tests were performed. After the description of the study sample, statistical analysis encompassed two steps. First, the expression of the studied markers in IPMNs was compared to their respective expression in the adjacent normal pancreatic ducts; to this end, p-values were derived from the Wilcoxon matched-pairs signed-ranks test. Subsequently, the associations between the expression of those markers, grade and histological subtype of IPMNs, were evaluated. Regarding grade, the Spearman's rank correlation coefficients and their corresponding p-values were calculated. On the other hand, concerning the associations implicating the histological subtype of IPMN lesions, the Kruskal-Wallis (KW) test was undertaken; the values of the KW chi-squared criterion (with three degrees of freedom, as the sample consisted of four groups) and their corresponding p-values are provided. Statistical analysis was performed with the STATA 11.1 software (StataCorp, College Station, TX, USA).
Results
The study sample consisted of 12 IPMNs lesions; of them five (41.7%) were of gastric-type, four (33.3%) were pancreatobiliary-type, two (16.7%) were intestinal-type and one (8.3%) was of oncocytic-type. Eight patients (66.7%) were males; age ranged between 47 and 77 years (mean±standard deviation (SD): 67.3±8.6; median, 69 years). The majority of lesions (41.7%) were associated with invasive carcinoma, followed by low-grade (25.0%) and intermediate-grade dysplasia (25.0%), whereas only one high-grade dysplasia lesion (8.3%) was noted. Table II presents the description of the study sample.
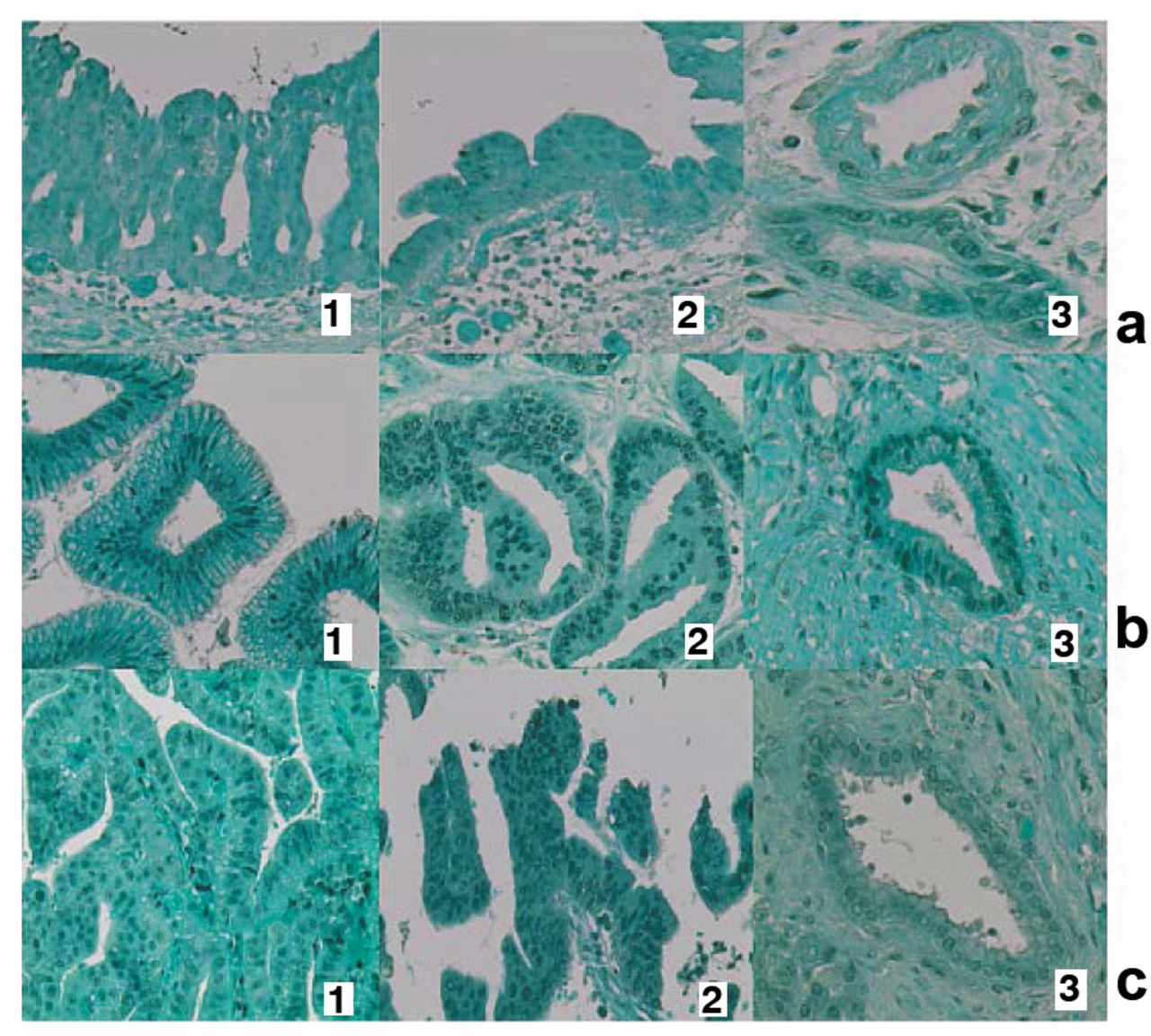
Concerning immunohistochemistry, ERα, ERβ, PR and AR expression was nuclear, as expected. ERα (Figure 3a), ERβ (Figure 3b) and PR presented low to moderate staining intensity in both IPMN lesions and normal pancreatic ducts. ERβ and PR showed additionally strong nuclear positivity in many (ERβ) and a few (PR) cells, respectively. In most of the IPMNs of the study more than 50% of the cells were AR-positive with predominantly low to moderate but also strong intensity in some cells. On the contrary, faint AR expression was observed in normal ducts (Figure 2a).

Spot of intraductal papillary mucinous neoplasm (IPMN) immunostained with cyclin D1 and elaborated with appropriate image analysis software (original magnification ×400).

a. Two different intraductal papillary mucinous neoplasms (IPMN) cases showing low to moderate androgen receptor (AR) expression in most nuclei but also strong intensity in a few of them (1, 2). Normal duct exhibiting weak positivity in a few cells (3). b. Two different IPMN cases showing weak to strong nuclear cyclin D1 positivity in most of the cells (1, 2). Normal duct exhibiting weak positivity in scarce cells (3).
Cyclin D1 positivity was often observed in the nucleus of IPMN cells, as opposed to very few normal duct cells that showed cyclin D1 expression; intensity ranged from weak to strong (Figure 2b). The staining pattern for p16 was nuclear (moderate to strong), as well as cytoplasmic in both IPMNs and normal pancreatic ducts (Figures 4a-b). Nevertheless, only nuclear staining was evaluated. P27 showed weak to moderate nuclear positivity in IPMNs but only weak positivity in normal ducts (Figure 3c). VEGF exhibited a granular, weak to moderate cytoplasmic expression in some IPMNs and normal duct cells (Figures 4c-d). Id-1 expression was cytoplasmic in all cases. Nuclear positivity was additionally depicted in a few of them; however, only cytoplasmic expression was evaluated. Staining intensity ranged between weak to strong in IPMNs and normal ducts (Figures 4e-f).

a. Estrogen receptor a (ERα): low to moderate (1, 2) nuclear positivity in intraductal papillary mucinous neoplasms (IPMNs) but only weak in normal duct (3). b. Estrogen receptor β (ERβ): low to strong staining intensity in both IPMN lesions (1, 2) and normal pancreatic ducts (3). c. P27: low to moderate (1, 2) nuclear positivity in IPMNs but only weak in normal duct (3).
Table III portrays the differences in the expression of the studied markers between IPMNs and the adjacent normal pancreatic ducts. AR H-score was significantly higher in the IPMN lesions (0.86±0.33 vs. 0.57±0.12 in the normal tissue, p=0.010, Wilcoxon matched-pairs signed-ranks test); moreover, cyclin D1 H-score was significantly higher in the IPMN lesions (0.47±0.23 vs. 0.21±0.20 in the normal tissue, p=0.019, same test). No significant differences were noted regarding the expression of ERα (p=0.239), ERβ (p=0.433), PR (p=0.136), p16 (p=0.308), p27 (p=0.182), VEGF (p=0.346), Id-1 (p=0.583) or MVD (p=0.906).
Table IV presents the results of the statistical tests examining the association between the expression of the studied markers, grade and histological sub-type of IPMNs. No significant associations were revealed either with IPMNs grade or with IPMNs histological subtype. Nevertheless, these analyses should be deemed explorative given the small study sample, especially among subgroups.

P16: Nuclear, as well as cytoplasmic staining, in intraductal papillary mucinous neoplasms (IPMNs) (a). Normal pancreatic duct showing only nuclear positivity (b). Vascular endothelial growth factor (VEGF): granular moderate cytoplasmic expression in IPMN(c) and normal duct cells (d). Inhibitor of differentiation/DNA synthesis 1 (Id-1): weak to strong cytoplasmic expression in IPMN (e) and normal duct (f). Nuclear positivity is also noted in IPMN case.
Discussion
In the present explorative study, AR and cyclin D1 expression, as depicted by H-score, were significantly more intense in IPMN lesions compared to the normal pancreatic ducts. No significant differences were noted regarding the expression of ERα, ERβ, PR, p16, p27, VEGF, Id-1 and MVD in the same structures. Moreover, no significant associations were revealed between the expression of the studied markers either with IPMNs' grade or with IPMNs' histological subtype. The existing literature is extremely poor regarding the expression profile of the aforementioned studied markers in IPMNs. Additionally, no previous study has compared expression of these markers to normal adjacent pancreatic ducts. Our study is the first to examine AR expression in IPMNs and to find it significantly higher compared to the adjacent normal pancreatic ducts. However, no association of AR expression with IPMNs' subtype and grade was found.
Moreover, this is the first study to examine ER expression in IPMNs using isoform-specific antibodies for ERα and ERβ. In our study all IPMN lesions exhibited low or low to moderate expression of ERα and ERβ respectively, in contrast to the results of previous studies (6-8) that reported no expression of ERα in IPMNs. The latter studies, however, used different ERα specific clones and evaluation was performed depending only on pathologist's estimation. Furthermore, our study is the first that found low PR positivity compared to the previous studies (6-8); all, except for one (6), used different primary antibodies against PR. Nevertheless, the latter survey used higher antibody dilution (1:50) and a somewhat different immunohistochemical technique. A possible explanation for the diversification of the aforementioned findings in our study would be that the image analysis technique employed can depict more details in immunohistochemical expression than a pathologist using light microscopy alone. Despite the fact that our study failed to find any association between ERα, ERβ and PR expression with IPMNs' grade and subtype, it is of great interest to further examine those associations in surveys using greater number of cases, taking into account studies indicating a putative therapeutic role of steroid receptor antagonist or blocking agents in pancreatic cancer (25-27).
In our study, VEGF expression in IPMNs was low to moderate in all cases. However, we failed to show a statistically significant difference of VEGF expression between IPMNs and normal pancreatic ducts as we failed to elucidate any correlation of that marker with IPMNs' grade and subtype. Two previous studies (10, 11) found increased VEGF expression as grade increased. This correlation, however, was not significant in one study (10), whereas the other work did not use statistical analysis (11).
Moreover, were the first to investigate Id-1 and MVD expression (using anti-CD34 immunostaining) in IPMN lesions. However, we have not ascertained any difference in the expression of the aforementioned markers between IPMNs and normal pancreatic ducts or any inter-correlation between those markers and IPMNs' grade and subtype. As Id-1-induced transcriptional activation of VEGF in various cancer types has been reported (28, 29) and given that anti-VEGF therapy (30) has been proven only temporary or not at all effective (31), therapeutic strategies based on targeting Id-1 expression may seem rather promising. At any case, according to a recent study, neovascularisation measured by angiogenesis-associated molecules like CD105 and CD31 seems to play an important role in the tumorigenesis of invasive pancreatic IPMNs (32).
Cyclin D1 over-expression is associated with worse patient outcome and often withmore aggressive phenotype in many cancers (33). Our study demonstrated significantly higher cyclin D1 expression in IPMNs compared to normal pancreatic ducts. Nevertheless, this over-expression was not associated either with the degree of dysplasia, in accordance to previously published studies, or with the histological subtype. In addition, p27 and p16 expression did not differ between IPMNs and normal pancreatic ducts, whereas no correlation was found between their expression with grade or histological subtype (15-18). Our results confirm the previous literature regarding p27 (18, 20) and the majority of literature regarding p16 (7, 15, 22, 23). This pattern seems distinct from that noted in PDAC, where p16 and p27 down-regulation or loss of expression has been associated not only with poor survival but also with various clinicopathological parameters, such as tumor size, grade, stage and lymph node metastases (34-37).
Description of the study sample.
Differences in the expression of the studied markers between intraductal papillary mucinous neoplasms (IPMNs) and the adjacent normal pancreatic tissue. Bold prints denote statistically significant differences between IPMNs and the adjacent normal pancreatic tissue.
Associations between the expression of the studied markers, grade and histological subtype of intraductal papillary mucinous neoplasms (IPMNs).
Concerning the limitations of this study, the small sample size should be mentioned, underlining the explorative nature of our approach. Indeed, the limited statistical power may have hampered the emergence of statistically significant associations that could have been noted in larger samples. However, the differences in expression patterns that were marked enough to emerge in this context of limited power may also be reproducible in larger series and may, thus, merit further validation. Additionally, this effort has adopted a cross-sectional design and no follow-up data regarding the survival of patients were assessed; nevertheless, any survival analysis approach would seem of limited reliability as only five cases were associated with invasive carcinoma.
In conclusion, our study showed higher expression of AR and cyclin D1 in IPMNs compared to normal pancreatic ducts. However, no association was found between AR and cyclin D1 expression and IPMNs' grade or sub-type. Accepting the limitations of our study, we consider it to be explorative and admit that possible inter-correlations of the studied markers, as well as their correlation with clinicopathological parameters, might not be explicitly clarified. The previous ascertainment, combined with the potential of selective targeting therapy of IPMNs, should prompt further validation of the present findings in studies encompassing larger samples and more elaborate techniques, such as western blotting and real-time quantitative polymerase chain reaction (qPCR).
Footnotes
-
↵* These Authors contributed equally to this study.
-
Funding
This study was supported by grants from the Alexandros Onassis Foundation, as part of Dr. D.Georgiadou doctoral thesis.
-
Ethical Approval
The study was approved by the Ethics Committee of Hippokratio Hospital.
-
Conflicts of Interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
- Received September 17, 2014.
- Revision received October 15, 2014.
- Accepted October 21, 2014.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.