


Abstract
Aim: We investigated the prognostic value of clinicopathological factors in patients with a distal bile duct adenocarcinoma after curative resection. Patients and Methods: This retrospective study included 25 patients who underwent 18F-fluorodeoxyglucose positron-emission tomography/computed tomography (FDG-PET/CT) before surgery. The maximum standardized uptake value (SUVmax), metabolic tumor volume (MTV), and total lesion glycolysis (TLG) were measured using FDG-PET/CT. FDG-PET/CT parameters and other clinicopathological factors were assessed to evaluate survival. Results: Univariate survival analysis showed that high TLG, high MTV, and high SUVmax were significant prognostic predictors for poor overall survival. For progression-free survival, high TLG and large tumor size were significant predictors for a poor prognosis. After multivariate survival analysis, only high TLG was an independent prognostic predictor for poor overall survival (p=0.025). Conclusion: Preoperative assessment of TLG by FDG-PET/CT might be a useful prognostic predictor in patients with a distal bile duct adenocarcinoma after curative resection.
Cholangiocarcinomas are rare malignant tumors, but with devastating characteristics (1). Because of differences in anatomy, clinical presentation, and management, they can be classified into three groups, namely, intrahepatic, perihilar, and distal bile duct cancer. Among them, the proportion of distal cholangiocarcinoma has been reported to be 20-30% (2). Because the bile duct has a thin tubal structure, distal cholangiocarcinoma typically present with the signs and symptoms of biliary obstruction. However, most patients are diagnosed at an advanced stage at initial presentation, resulting in poor survival (3, 4). Furthermore, not only patients with advanced-stage disease, but also those who undergo surgical resection for localized tumors have unsatisfactory prognoses (5).
Finding an appropriate treatment strategy with regard to prognosis is most important if we are to improve survival in patients with such cancers. Several prognostic factors, such as the resection margin status, tumor invasion, and lymph node metastasis, have been suggested for predicting the outcome for patients with resectable distal cholangiocarcinoma (6). However, the role of such factors has not yet been clearly determined. Parameters measured by 18F-fluorodeoxy-glucose positron-emission tomography/computed tomography (FDG-PET/CT), such as the maximum standardized uptake value (SUVmax), have been recommended as prognostic factors for several cancer types (7-9). The metabolic tumor volume (MTV) and total lesion glycolysis (TLG) are also measurable by FDG-PET/CT using automated contouring programs. These parameters can be used to assess the tumor burden and overall metabolic activity. Because the tumor burden is associated with prognosis, the prognostic values of MTV and TLG have been investigated, with promising results (10, 11). Despite the prognostic potential of FDG-PET/CT parameters, only SUVmax has been evaluated as a possible prognostic factor for distal cholangiocarcinoma, mostly in combination with other types of hepatobiliary cancer (12, 13). Therefore, this study aimed to investigate the prognostic value of clinicopathological factors including the FDG-PET/CT parameters SUVmax, MTV, and TLG in patients with distal cholangiocarcinoma who underwent potentially curative resection.
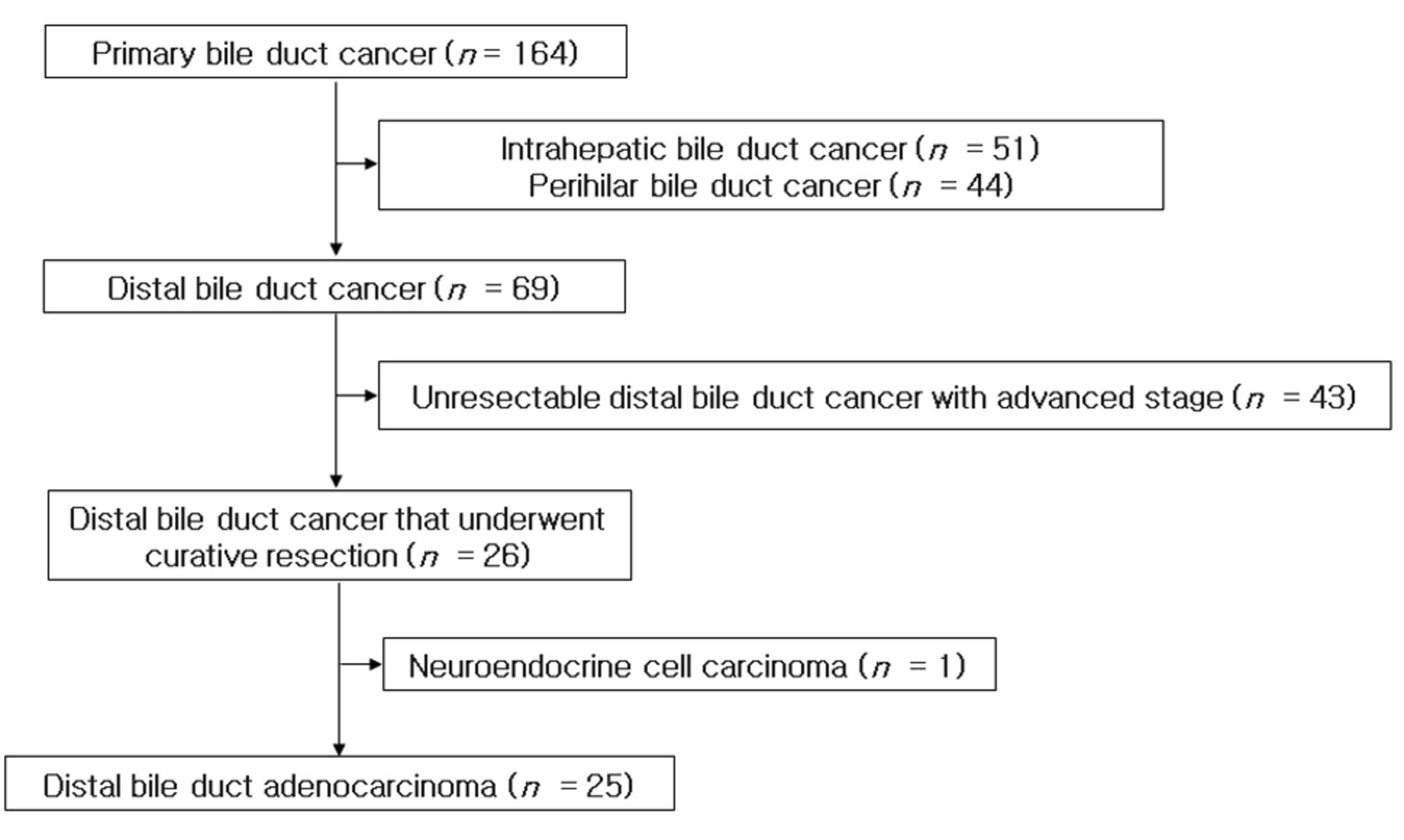
Flowchart of patient enrollment.
Patients and Methods
Patients. This retrospective study was approved by our Institutional Review Board, with a waiver from the need to obtain informed consent. The medical records of 164 consecutive patients with newly diagnosed cholangiocarcinoma who underwent FDG-PET/CT as part of the tumor staging procedures at our medical center from August 2008 to March 2014 were reviewed. Inclusion criteria for this study were as follows. Firstly, the tumor was located in the distal bile duct; patients with intrahepatic and perihilar bile duct cancer were excluded, along with those with ampullary, gall bladder, and pancreatic tumors. Secondly, patients underwent potentially curative resection and had subsequent clinical follow-up at our medical Center. Patients who did not undergo curative surgery for advanced-stage cancer were excluded. Thirdly, patients with carcinoid tumors or sarcomas were excluded. The flowchart of patient selection is shown in Figure 1. Tissue diagnosis was obtained before surgery by endoscopic retrograde cholangiopancreatography, percutaneous transhepatic cholangioscopy or direct peroral cholangioscopy with biopsy or cytology. Contrast-enhanced computed tomographic (CT) or magnetic resonance imaging (MRI) of the abdomen were performed within 2 weeks of FDG-PET/CT, before surgery. Preoperative levels of the serum tumor marker cancer antigen (CA) 19-9 were measured. The TNM stage was determined using surgical specimens. All patients were staged according to the 2010 American Joint Committee on Cancer staging manual, seventh edition (14).
Treatment and clinical follow-up. All patients underwent surgical resection with curative intent after the pathology diagnosis and initial tumor staging. Postoperative adjuvant chemotherapy was administered to patients according to the stage of the tumor or their individual medical condition. Adjuvant chemotherapy regimens used in this study included 5-fluorouracil and cisplatin (nine patients), 5-fluorouracil and leucovorin (one patients), and gemcitabine and cisplantin (two patients). Each chemotherapy regimen was selected according to the physician's discretion and was not related to the degree of disease. Chemotherapeutic responses were evaluated by contrast-enhanced CT after the third or fourth cycle of chemotherapy according to the Response Evaluation Criteria in Solid Tumors (15). Patients without tumor progression underwent further therapy with the same regimen. Patients with progressive disease underwent second-line chemotherapy or supportive care. Follow-up monitoring for recurrence or metastasis was performed every 3-4 months. Follow-up evaluation included a complete physical examination, biochemical screening, and contrast-enhanced abdomen CT. Contrast-enhanced chest CT, MRI, and FDG-PET/CT were performed whenever indicated clinically.

Measurement of metabolic tumor volume from images by an automated contouring program (arrow).
FDG PET/CT imaging and analysis. All patients fasted for at least 6 h prior to imaging. Blood glucose concentrations were checked before the PET studies (<120 mg/dl indicating patients without diabetes and <200 mg/dl indicating diabetes). Individuals in the resting state were given intravenous injections of FDG (4.8 MBq/kg of body weight). PET/CT images were acquired 60 min later using a GEMINI PET/CT scanner (Philips Medical Systems, Cleveland OH, USA). The axes of both PET and CT systems were aligned mechanically. CT was performed from the skull base to the mid-thigh (without intravenous contrast) for correcting attenuation and anatomical localization using a standardized protocol of 120 kV, 50 mA, tube-rotation time 0.75 s per rotation, pitch 1.5, and section thickness 5 mm. Immediately after CT, PET images were acquired for 2.5 min per frame using a conventional three-dimensional protocol.
Two experienced Nuclear Medicine physicians assessed the FDG-PET/CT images. Any discrepancies were resolved by consensus. All images were reviewed on a workstation (Extended Brilliance Workspace; Philips Healthcare). Volumetric regions of interest were placed over areas of the malignant lesion. The SUV was defined as the concentration of FDG divided by the injected dose and normalized to the body weight of the patient. The SUVmax, MTV, and TLG values of the primary tumor were recorded. The MTV (in ml) was measured from attenuation-corrected torso FDG PET/CT images by an SUV-based automated contouring program (Figure 2). Initially, voxels with a threshold of 40% of the SUVmax in the volume of interest within the contouring margin were incorporated to define the tumor margin accurately. If the tumor margin was not defined correctly, the SUVmax threshold was adjusted accordingly. The TLG was calculated by multiplying the MTV by the corresponding average SUV determined in a selected contouring volume of interest.
Statistical analysis. The primary endpoint was overall survival (OS), and the secondary endpoint was progression-free survival (PFS). OS was defined as the time between the date of PET imaging and the date of death from cancer. Patients who had not died at the date of the last clinical follow-up and who died from any other cause were censored. PFS was measured from the date of PET imaging to the first recurrence of the disease. Patients who did not have disease progression at the date of their last clinical follow-up were also censored. The OS rates for 1, 3, and 5 years were analyzed using the Kaplan–Meier method. For survival analysis, the cut-off values for categorization of low and high primary tumor SUVmax, primary tumor MTV, primary tumor TLG, primary tumor size, and preoperative levels of CA19-9 were determined using receiver operation characteristic (ROC) curve analysis. Univariate analysis of prognostic factors was performed using the Kaplan–Meier method, and the significance of differences between survival curves was tested with the log-rank test. Multivariate survival analysis for independent prognostic factors was performed using a Cox proportional hazards model that included significant univariate variables. PASW statistics version 17.0 for Windows (SPSS, Chicago IL, USA) was used for the analyses. p-Values of less than 0.05 were considered statistically significant.
Results
Patients' characteristics. Twenty-five patients (three women, 22 men; mean age=67±6 years) with distal cholangiocarcinomas were eligible for study inclusion. The clinical characteristics of patients are summarized in Table I. Pathology results of all patients indicated distal bile duct adenocarcinoma. No patient died in hospital from postoperative complications. For curative surgery, five bile duct resections, 11 pylorus-preserving pancreaticoduodenectomies, and nine Whipple procedures were performed. One patient undergoing bile duct resection also underwent resection of the portal vein. No hepatectomy was combined with a pylorus-preserving pancreaticoduodenectomy or Whipple procedure.
Survival analysis. The OS rates were 92%, 67%, and 54% for 1, 3, and 5 years, respectively. At the time of last follow-up, 16 out of 25 patients had survived with a minimum of 14.6 months of clinical follow-up (median=38.9 months). For survival analysis, the cut-off values for categorization of low and high primary tumor SUVmax, primary tumor MTV, primary tumor TLG, primary tumor size, and preoperative level of serum CA19-9 were set at 4.0, 2.8 ml, 13.0, 2.0 cm, and 125.0 U/ml, respectively. Each cut-off value was selected based on an ROC curve analysis of our data.
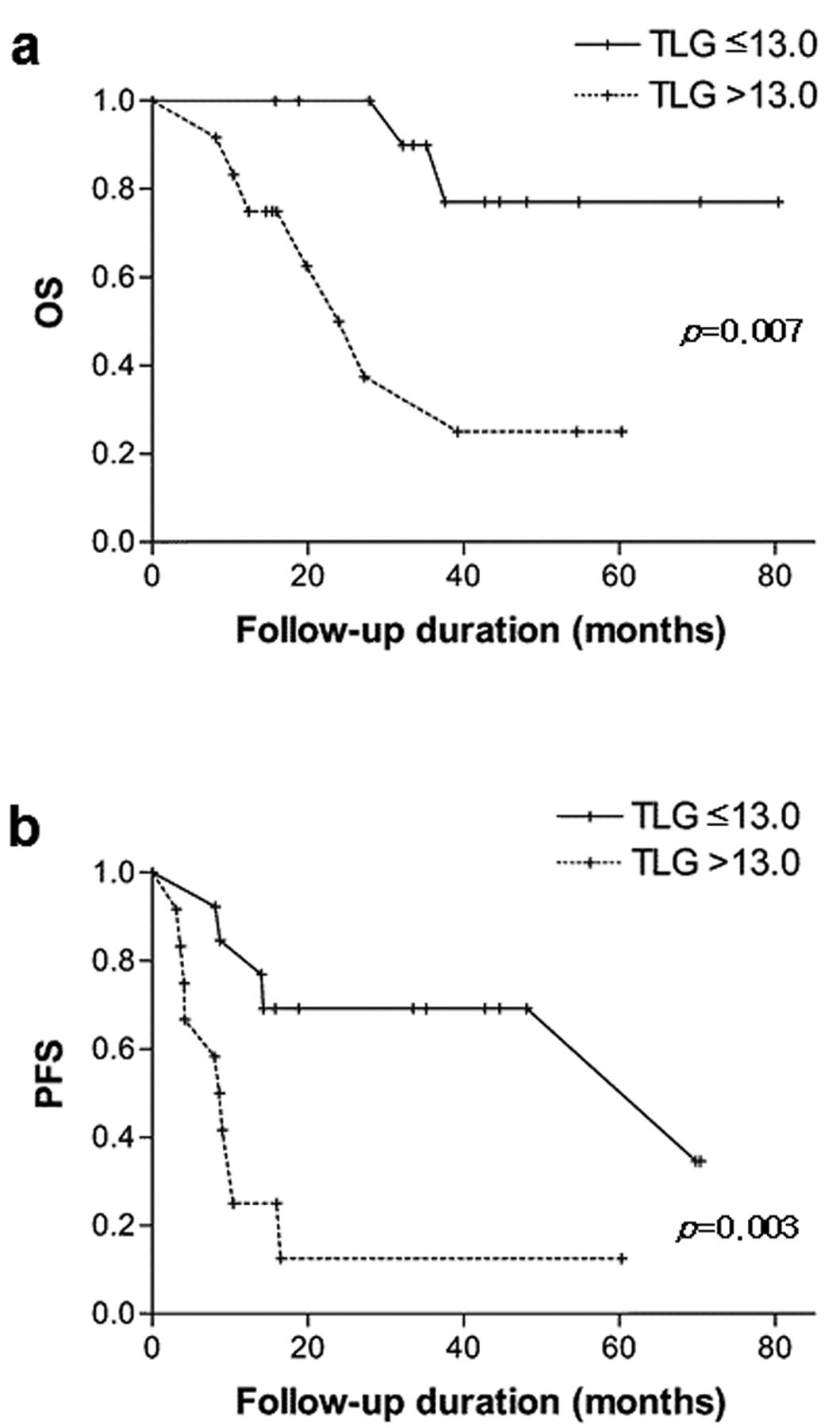
Univariate survival analysis identified that a high primary tumor TLG value (>13.0), a high primary tumor MTV value (>2.8 ml), and a high primary tumor SUVmax value (>4.0) were significantly prognostic predictive of poor OS. For PFS, a high primary tumor TLG value (>13.0) and a large primary tumor size (>2.0 cm) were significant predictors of poor prognosis (Table II). The Kaplan–Meier survival curves for OS and PFS according to the primary tumor TLG value are shown in Figure 3.
Clinical characteristics of patients.
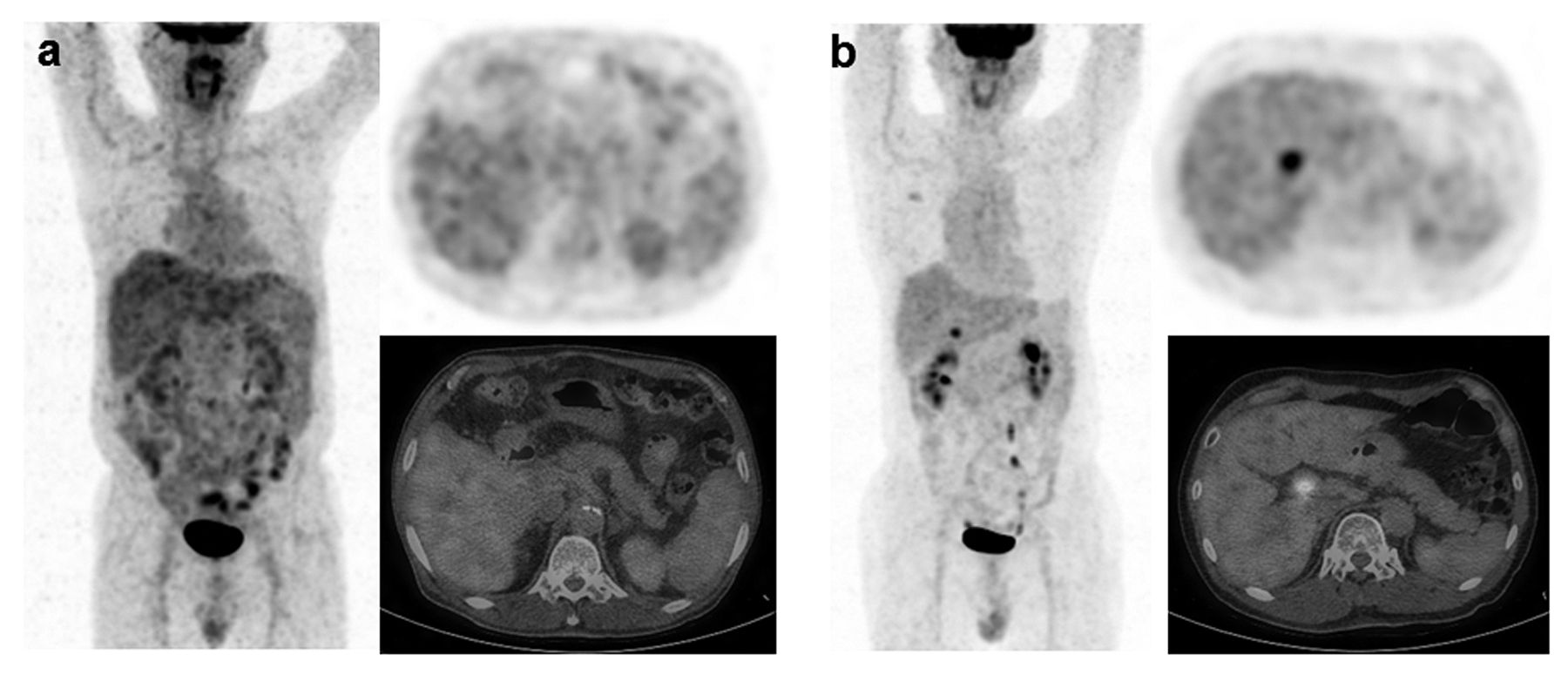
After multivariate analysis of patient survival, only a high primary tumor TLG level was an independent prognostic predictor for poor OS (Table III). No independently prognostic predictor was found for PFS. Representative examples from patients with distal bile duct adenocarcinoma with a low and high primary tumor TLG values are shown in Figure 4.
Discussion
To our knowledge, this is the first report to evaluate the prognostic value of the primary tumor TLG level in patients with distal bile duct adenocarcinomas after potentially curative resection. The primary tumor TLG value was the only independent prognostic factor for OS.
Several prognostic factors based on tumor characteristics such as TNM stage, histological type, perineural and lymphovascular invasion, positivity of the surgical margin, and preoperative levels of serum tumor markers have been suggested for patients with distal cholangiocarcinomas (14). DeOliveira et al. reported that histological margins after resection, lymph node metastasis, tumor size, and tumor differentiation were significantly associated with the prognosis of patients with for cholangiocarcinoma after resection (4). Similarly, Kwon et al. reported that the TNM stage and lymphovascular invasion of primary tumor were independent prognostic factors for patients with distal cholangiocarcinomas (16). However, those factors did not have any significant predictability for the prognosis in the present study. This result might be explained by the small number of patients included. On the other hand, this might emphasize the value of the primary tumor TLG value as a prognostic predictor.
Univariate analysis of progression-free survival and overall survival.
We also found that the SUVmax value was not an independent predictor for prognosis. Previous reports suggested that this parameter is associated with tumor aggressiveness and survival in patients with various cancer types (17-19). However, it has limited value for demonstrating the precise metabolic burden of the whole tumor. SUVmax only measures a single maximum uptake count in a region of interest, not an entire tumor's metabolic activity. Accordingly, several recent reports suggested that volumetric parameters of tumors measured by FDG-PET/CT, such as TLG and MTV, are more accurate prognostic factors than SUVmax in patients with various malignancies (20, 21). Consistent with those reports, our results suggest that TLG might be a more reliable prognostic factor than SUVmax in patients with distal bile duct adenocarcinomas after curative resection.
To date, the only curative treatment in patients with distal cholangiocarcinomas that enables long-term survival is complete surgical resection with a negative margin (22). No standard protocol for adjuvant therapy is widely accepted for such patients. In previous randomized clinical trials, no significant improvement in survival was found among patients with adjuvant chemotherapy compared to simple postoperative observations (23, 24). Recently, the association of improved OS with adjuvant radiotherapy after curative resection for extrahepatic biliary tract cancer was found by a meta-analysis of 10 observational studies in the absence of randomized controlled studies (25). Some institutional studies suggest a possible benefit from adjuvant chemoradiation or chemotherapy in patients with resected extrahepatic cholangiocarcinomas (26). Valle et al. reported some improvements in survival in patients with locally advanced unresectable or metastatic cholangiocarcinomas using a cisplatin plus gemcitabine regimen (27). In pre-clinical studies, the therapeutic potential of molecular targeting has emerged and the epidermal growth factor receptor pathway is one such promising target (28, 29). However, there are too few studies and inconsistent results to support the general use of adjuvant therapy after curative resection. Furthermore, most studies included patients with intrahepatic and extrahepatic cholangiocarcinomas, or cancer of the ampulla of Vater, gallbladder, and pancreas.
Multivariate analysis of progression-free and overall survival.
In our univariate survival analysis, patients with higher stages of cancer and a positive histological margin after resection had a hazard ratio of <1.0 for both OS and PFS. Although this difference in survival was not significant, this might be because most of these patients underwent adjuvant chemotherapy after resection. Therefore, we hypothesize that a patient with distal bile duct adenocarcinoma who has a high primary tumor TLG at preoperative FDG-PET/CT imaging might benefit from further adjuvant therapy after curative resection. Because of the medical insurance coverage in Korea, 5-fluorouracil and cisplatin were the first-line treatments in most patients who underwent adjuvant chemotherapy in this study. Further prospective large-scale studies should be conducted to establish the standard adjuvant treatment for patients with distal bile duct adenocarcinomas.
There were several limitations to this study. Firstly, and most importantly, the results were obtained by a retrospective review of a small study population at a single institution. This weakened the statistical power of our analysis. In addition, patient-selection bias might have influenced the prognostic value of each parameter. Therefore, this should be considered a preliminary report. Secondly, we included only patients with distal bile duct adenocarcinomas. As a result, our results are not applicable to those with entire distal cholangiocarcinomas. However, the homogeneity of our study population might strengthen the statistical power in considering such a small patient group. Thirdly, the follow-up duration was limited for some patients. However, because most surviving patients had a follow-up time of more than 2 years (12/16, 75%), it is unlikely that our conclusions will change significantly with further follow-up.

Kaplan–Meier analysis of overall survival (OS) (a) and progression-free survival (PFS) (b) according to primary tumor TLG value.

Evaluation in patients with distal bile duct adenocarcinoma. a: A 74-year-old man with a low primary tumor TLG value (4.0). He had no tumor-progression and survived until the last follow-up (42.7 months of progression-free and overall survival). b: A 69-year-old man with a high primary tumor TLG value (14.3). His progression-free survival was 3.1 months and overall survival was 8.2 months.
In conclusion, preoperative assessment of primary tumor TLG values by FDG-PET/CT was an independent prognostic predictor for OS in patients with distal bile duct adenocarcinomas after curative resection. Furthermore, the prognosis was more predictable using the primary tumor TLG value rather than previously recommended prognostic factors such as tumor stage, surgical margin, perineural and lymphovascular invasion, or the preoperative levels of serum CA19-9. Therefore, primary tumor TLG measured by FDG-PET/CT preoperatively might be a useful predictor for prognosis in patients with distal bile duct adenocarcinomas after curative resection.
Acknowledgements
This work was supported by the Konkuk University Medical Center Research Grant 2015.
Footnotes
Ethical Statement
This study was reviewed by the appropriate Ethics Committee and was therefore performed in accordance with the ethical standards laid down in the Declaration of Helsinki revised in Brazil 2013. This retrospective study was waived from the need to obtain informed consent by our Institutional Review Board.
Conflicts of Interest
The Authors declare that we have no conflicts of interest.
- Received September 10, 2015.
- Revision received October 7, 2015.
- Accepted October 8, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of Metabolic Parameters of 18F-Fluorodeoxyglucose Positron-emission Tomography After Hepatic Resection in Patients With Intrahepatic Cholangiocarcinoma
- Prospective Evaluation of the Clinical Implications of the Tumor Metabolism and Chemotherapy-Related Changes in Advanced Biliary Tract Cancer
- Karnofsky Performance Score Is Predictive of Survival After Palliative Irradiation of Metastatic Bile Duct Cancer
- Outcomes After Radio(chemo)therapy for Non-Metastatic Bile Duct Cancer