


Abstract
Neurofibroma constitutes a heterogeneous group of solid tumours occurring sporadically or in association with syndromes. The aspect of these peripheral nerve sheath tumours may vary considerably, with disseminated tumours covering various parts of the body or nodular/diffuse plexiform neurofibroma that can grow to an impressive size. Although neurofibromas have vascular density comparable to that of normal tissue, they have tendency to bleed upon surgery which is poorly understood. Herein we investigated whether this finding may result from alterations of peripheral vasculature innervation. Different types of neurofibroma and controls were evaluated with special reference to nerve fibre topography and vessel density. Materials and Methods: Seventy-six formalin-fixed and paraffin-embedded tissue samples (63 neurofibromas and 13 skin biopsies) were retrieved from the archives of the Institute of Neuropathology, University Medical Center Hamburg-Eppendorf. Nerve fibres and blood vessels were differentiated immunohistochemically on 10-μm-thick tumour slices using antibodies against smooth muscle actin (arteries), protein gene product 9.5 (PGP9.5) and neurofilament (nerve fibres). Skin samples served as controls. Nerve fibre and vessel densities were quantified morphometrically. Results: Nerve fibre density varied considerably. However, vascular innervation did not statistically significantly differ between the different tumour sub-groups and controls. Vessel density was not significantly increased in tumours compared to skin biopsies. Within the tumour sub-groups, diffuse plexiform neurofibroma presented a significantly higher vascular density than atypical neurofibroma (p=0.006). Conclusion: Blood vessel density and vascular innervation in the whole cohort of neurofibromas did not significantly differ from that of controls. Thus, the source of prolonged and intense bleeding of neurofibroma during surgical procedures cannot be explained by increased vessel density or loss of innervation, but may be attributed to other factors such as alterations in the structure of the vascular wall.
- Nerve fibre density
- vessel density
- blood vessels
- lymphatic vessels
- NF1
- neurofibroma
- neurofibromatosis
- vessel innervation
Neurofibromatosis type 1 (NF1) is one of the most important inherited human diseases (1). Penetrance in affected individuals is almost 100% but the phenotype is highly variable (1). In 1987, the NF1 gene was discovered on the pericentromeric region of chromosome 17 (2, 3). The complete sequence of the gene locus 17q11.2 was published three years later (4). The NF1 gene comprises of 350 kb genomic DNA (1) organized into 60 exons which code for neurofibromin, a protein of 2,485 amino acids (4). The protein has a molecular weight of about 220-280 kDa (5) and acts as a tumour suppressor. It is a negative regulator of rat sarcoma (RAS)-GTPase in the RAS pathway (6). Furthermore, neurofibromin stimulates intracellular adenylate cyclase resulting in a decrease of intracellular cAMP (4, 5, 7). It was shown that translocation mutation (‘loss of function‘) results in aberrant activation of RAS (1) and functional loss of cell proliferation control (4). While neurofibromin is present in many human cell types, its expression is predominantly detected in neurons and glial cells, in particular Schwann cells (8).
A predominant feature of NF1 is the development of multiple neurofibromas that may present as distinct tumours of the skin resembling button-like knots (cutaneous or dermal neurofibroma) or as tumours arising at various segments of a peripheral nerve arranged like a string of pearls (plexiform neurofibroma). Plexiform neurofibroma in NF1 de-differentiates into malignant peripheral nerve sheath tumours (MPNST) with a lifetime risk of 8-13% (9). MPNST are highly vascularized (10, 11).
The therapy of choice in NF1 is surgical resection of tumours. During ablative surgery for neurofibroma, an increased blood loss from the surgical site is well known (12). It was shown that neurofibroma Schwann cells have angiogenic properties and that NF1 haploinsufficiency augments angiogenesis (13, 14).
Spontaneous bleeding in elephantiasis neurofibromatosa is well-known (15-17). Heavy bleeding during surgical procedures may result from higher vessel density in tumours compared to unaffected skin regions, or alternatively, increased blood flow could lead to the same phenomenon. Previous studies have shown no increased vascular density of cutaneous and plexiform neurofibroma compared to normal human skin (18), but increased vascularization of malignant peripheral nerve sheath tumours is well-documented (10, 11). A hypothesized increased blood flow in benign tumours without apparently increased vessel density could result from a larger vessel diameter, in particular in resistant vessels. Neural and endocrine factors have a huge impact on the actual diameter of vessels via interaction with vascular smooth muscles.
In neurofibroma, tumorous growth of Schwann cells can lead to degeneration of nerve fibres (18). Discontinuation of functional sympathetic nerve fibres in neurofibroma might result in denervation of associated blood vessels and consequently in permanent vessel dilatation. This would predominantly affect resistance vessels. To assess this hypothesis, we investigated the vascularization and nerve supply of arterioles in NF1-associated neurofibroma and control tissue.
Materials and Methods
Patients. All patients fulfilled updated clinical diagnostic criteria for NF1 of the US National Institutes of Health given in Table I (19). Skin samples from patients who did not show NF1 served as controls. All data were anonymized prior to the study. The mean age of patients was 35.05±18.09 years (minimum 2 years, maximum 80 years) at the time of tissue excision.
Tissue samples. Seventy-six formalin-fixed and paraffin-embedded tissue specimens from NF1-associated neurofibromas (n=63) and skin biopsies (n=13) were drawn from the archive of the Institute of Neuropathology, University Medical Center Hamburg-Eppendorf. The samples originated from surgical patients treated in the Department of Oral and Craniomaxillofacial Surgery (Table II). Prior to the study, the specimens were investigated using haematoxylin and eosin, periodic acid Schiff reaction and elastica van Gieson stain. In addition, all samples were immunohistochemically stained with antibodies against epithelial membrane antigen (EMA), Ki-67, S100 and neurofilament (NF). For this study, the material was independently re-evaluated by two neuropathologists applying current WHO criteria (20) to diagnose peripheral nerve sheath tumours (MG, CH). Following these procedures, 10-μm-thick section were cut from the blocks for immunohistochemical detection of neurofilament, PGP9.5 and smooth muscle actin (SMA) (Table III).
Pre-treatment of slides. SuperFrost Plus® slides (Menzel Gläser, Braunschweig, Germany) were coated with poly-L-lysine-solution for 5 minutes, dried for 60 min at 60°C and stored dust-free until usage.
Preparation of slices. Slices 10-μm-thick were cut from the tissue blocks omitting ice-cooling of the block prior to cutting. Cuts were stretched in a water bath at 60°C and drawn onto poly-L-lysine pre-treated slides. A rubber roller was used to slightly press the slices onto the slides. After adhering to the slides, the specimen were stored at 60°C for 120 min.
Immunhistochemical double staining of NF and SMA. All reagents were freshly prepared and rapidly used. Two specimens of normal nerves (biopsy) were added as controls in every staining passage. Briefly, 10-μm tissue sections were de-waxed for 120 min at 65°C in a dry cabinet followed by 8 h in xylol. Then blocking of endogenous peroxidase in 3% H2O2 for 90 min in 100% ethanol was perfomed followed by a descending series of ethanolic solutions and antigen de-masking for 90 min in citrate buffer (pH 6.0) at 85°C in closed cuvette in a water-bath. Tissues were cooled to room temperature in citrate buffer for about 45 min, then rinsed in Tris-buffered saline (TBS). Nonspecific antibody binding was blocked with 10% goat serum in TBS buffer for 30 min at room temperature in a humid chamber. For incubation with 200 μl diluted NF antibody solution (1:400) was added for 18 h at room temperature. Secondary antibody (Histofine® Simple Stain MAX PO-Multi, Nichirei, Tokyo, Japan) was applied for 3 h at room temperature and bound antibodies were visualized with 3’3-diaminobenzidine-tetrahydrochloride (DAB) for 15 min. After thorough rinsing in TBS, SMA antibodies were applied (1:2,000) for 18 h at room temperature. Histofine® Simple Stain MAX PO-Multi AP was applied for 3 h as secondary antibody and bound SMA antibodies were visualized with Fast-Red Chromogen for 15 min.
Immunhistochemical double staining of SMA and PGP9.5. Double staining of tissue sections with PGP9.5 and SMA was performed with fully automated staining equipment (BenchMark XT; Ventana Medical Systems, Tucson, AZ, USA). The automat performed all necessary staining steps on up to 30 slides in one run. In order to achieve representative results in 10-μm-thick slices, tissues were de-waxed with xylene for 8 h and incubated in 3% H2O2 for 2 h prior to starting the staining procedure.
Measurement of tissue nerve fibre density (NFD) and vessel density (VD). Double-stained (SMA, NF) specimens were fixed on the electromechanical specimen stage of a StereoInvestigator® light microscope (MBF Bioscience, Williston, VT, USA). Basic settings (light quality, colour filter) were identical for all measurements. The whole tumour area was circled and marked using the measurement algorithm of StereoInvestigator® software under a ×5 objective (EC Plan NeoFluar; Carl Zeiss, Jena, Germany). The measurement frame was set at 500×250 pixel. Thereafter, the complete digitally marked tumour area was automatically screened. The screened area was visualized on a monitor. Markings were restricted to crosswise cut vessels and nerves. Nerve fascicles consisting of several axons were marked only once. NFD and VD were calculated as the total number of marked objects per mm2.
Number of patients, age (range) and tumour sub-type.
Antibodies used for immunohistochemistry.
Relative innervation of vessels with smooth muscles. Slices were evaluated at ×400 magnification with a Carl Zeiss Axiovert S-100 (Zeiss) light microscope. Measurement started on the left upper margin of the sample. The whole specimen was examined from visual field to visual field. For every visual field, the total number of SMA-marked vessels and the number of vessels with adjacent PGP9.5-stained nerve fibres were counted. Crosswise cut vessels were counted only. A vessel was judged to be innervated when the maximum distance of the nerve fibre to smooth muscle cells of vessel did not exceed 5 μm. The number of innervated vessels was divided by the total number of vessels present then multiplied by 100 to give the percentage vessel innervation.

Example of double labelling with antibodies against smooth muscle actin and neurofilament in a cutaneous neurofibroma. Red: Smooth muscle actin in an arterial walls (chromogen fast red); brown: neurofilament labelling of nerve fibres (arrows, chromogen diaminobenzidine (DAB); scale bar=100 μm.
Statistical evaluation. Statistical analysis was performed with IBM® SPSS® Statistics 21 software (International Business Machines, Armonk, NY, USA). Nerve fibre density, VD and perivascular innervation were calculated from primary data. Student's t-test for independent variables and unifactorial analysis of variance were used for calculating group-specific differences. Post-hoc Tukey test was used to compare vessel density with respect to tumour type.
Results
Nerve fibre density. The mean size of the evaluated area was 5.18 mm2 (median 4.56/mm2, standard deviation 3.39, standard error of mean: 3.89, range=0.92-27.21/mm2). Staining result is illustrated in Figure 1.
The mean NFD of all 76 cases was 13.59 nerve fibres/mm2. Nerve fibre density was highest in plexiform-nodular neurofibroma (mean=19.99 nerve fibres/mm2) and lowest in the 13 skin samples (5.14 nerve fibres/mm2) (Figure 2). Plexiform-diffuse neurofibroma had a lower NFD (11.95 nerve fibres/mm2). The mean NFD of plexiform neurofibroma overall was 15.83 nerve fibres/mm2 (Figure 2).
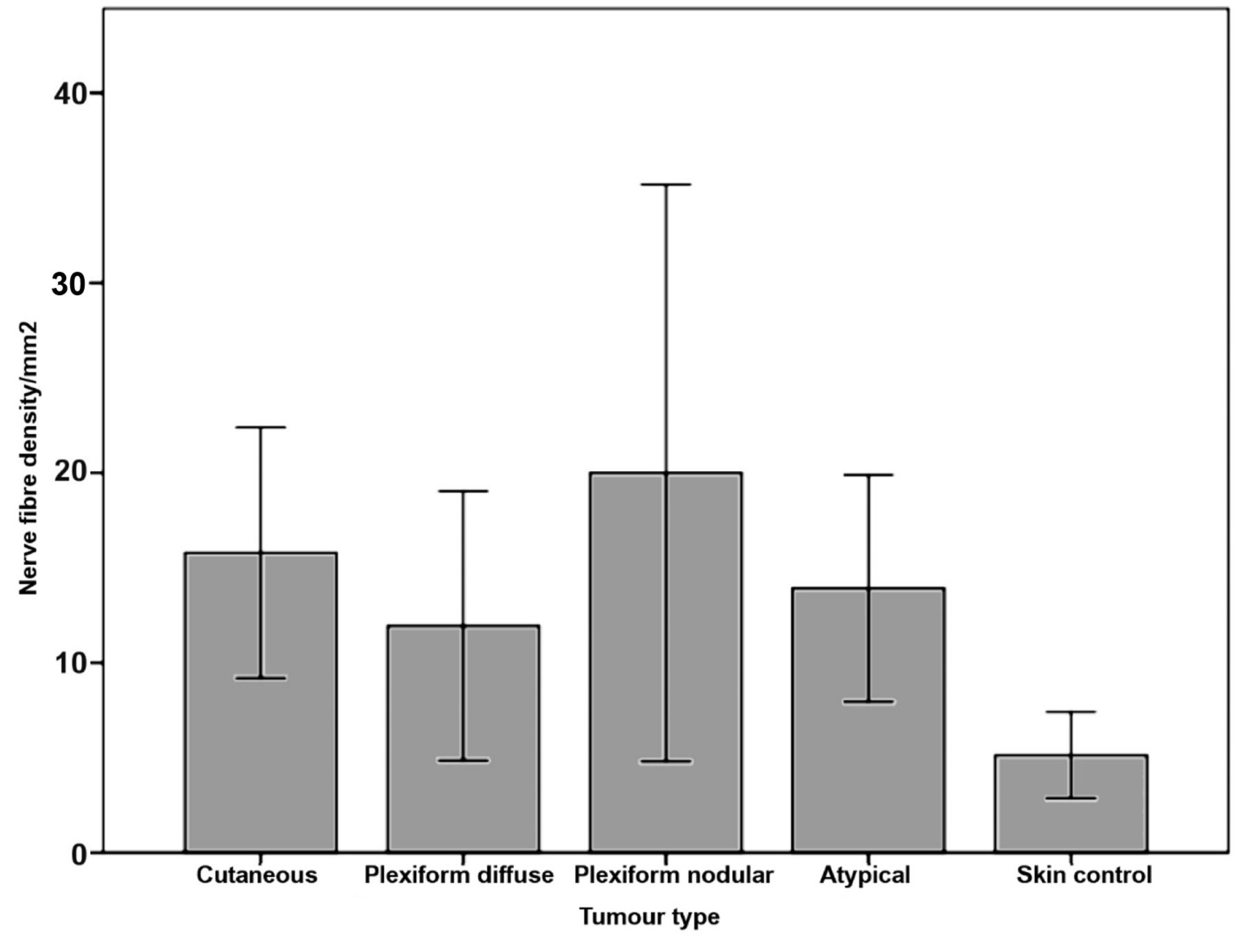
Nerve fibre density in neurofibromatosis type 1 (NF1)-associated neurofibroma and skin biopsies. Data are the mean±95% confidence interval.
Comparing mean NFD values, the t-test demonstrated a significantly higher NFD in cutaneous neurofibromas compared to skin biopsies (p=0.001). All other comparisons of the means revealed no significant differences of measurements.
Vessel density. Vessel density was highest in plexiform-diffuse neurofibroma followed by cutaneous neurofibroma and plexiform-nodular neurofibroma (Figure 3).
Univariate analysis of variance (ANOVA) revealed significant differences with respect to histological diagnosis (p=0.003). Post-hoc analysis with Tukey HSD test demonstrated a significantly higher VD in plexiform diffuse neurofibroma compared to atypical neurofibroma (p=0.006) and in plexiform-diffuse neurofibroma compared to skin samples, respectively (p=0.01).
Relative vessel innervation. A mean of 129 vessels were evaluated per case. Out of 9,813 vessels assessed, 628 showed an innervation. The mean relative vessel innervation of all 76 cases was 8.8%. This result implies the detection of a nerve fibre in the region of every 12th vessel. Relative vessel innervation was highest in skin samples (13.24%) and lowest in plexiform-diffuse neurofibroma (4.71%). However, univariate ANOVA and t-test revealed no significant differences of this parameter between histological subtypes and controls (Figures 4 and 5) because of large variations between the cases.
Discussion
The present study revealed a remarkable heterogeneity of NFD and VD in NF1-associated neurofibroma as well as in control samples of skin biopsies. The morphometric analysis demonstrated only minor differences in NFD and VD between control tissues and peripheral nerve sheath tumours.
Only few authors calculated NFD as a measurement related to tissue area. For example, one study reported an NFD of 21.1 nerve fibres/mm2 in 17 skin biopsies of healthy controls (21). In contrast to these findings, in the present study, the NFD values were remarkably lower in the controls. Possible causes of this are physiological variations of NFD, age and also an impact of technical procedures, such as the thickness of tissue sections. Furthermore, we only had access to skin specimens that were biopsied for diagnostic reasons (dermatitis, vasculitis, polyneuropathy, dermatomyositis etc.) and therefore, even if the skin did not harbour obvious pathological alterations, an underlying disease may have led to a reduced NFD.

Vessel density in NF1-associated neurofibroma and skin biopsies. Data are the mean±95% confidence interval.
Concerning the tumour sub-groups, plexiform-nodular neurofibromas had the highest nerve fibre counts. Since these tumours grow primarily within a peripheral nerve where numerous nerve fibres of the fascicle may be preserved, this finding was to be expected. The extensive variation in the number of nerve fibres in plexiform-nodular neurofibromas likely resulted from different stages of degeneration of pre-existing nerve fibres and differences in the number of nerve fibres contained in the fascicle before tumorous transformation. Plexiform diffuse neurofibromas, which are characterized by nodular and diffuse tumour growth, demonstrated lower nerve fibre counts. This is plausible because adjacent connective tissue invaded by the tumour does not have a high nerve fibre density. Atypical neurofibromas are defined by increased nuclear pleomorphism and other histological features not referring to the intraneural or diffuse growth and thus may present as diffuse or nodular tumours. The mean fibre density was in the range of diffuse and nodular tumours. Fibre densities in cutaneous neurofibromas were also in the range of those for diffuse tumours. Comparing the findings in neurofibroma with those in normal skin reported in the above mentioned study (21), the mean NFD of all tumours except for intraneural neoplasms were below 21.1 nerve fibres/mm2, although the maximum values in some cases reached levels of normal skin. This is in accordance with clinical findings showing that patients with NF1 only rarely suffer from a clinically apparent polyneuropathy (22, 23), but show abnormal-evoked sensitive potentials of the peripheral nervous system in about 36% of cases, indicating a sub-clinical neuropathy (24).

Example of double labelling with antibodies against smooth muscle actin and protein gene product 9.5 (PGP9.5). Red: Smooth muscle actin in an arterial wall (chromogen fast red); brown: PGP9.5 labelling of innervating nerve fibres (black arrows) and distant nerve fibres (grey arrow) (chromogen diaminobenzidine (DAB); scale bar=20 μm.
Overview of published studies of vessel density (VD) providing normal and pathological (*) values.
Vessel density. Vessel density has a practical relevance in the assessment of malignancy in tumours, e.g. breast cancer. Data in the literature differ remarkably, both for malignant and benign entities. Rossi et al. studied VD by means of immunohistochemical detection of von-Willebrand-Factor in healthy skin of the lower arm. In this location, VD in papillary dermis was 139.5 vessels/mm2 and thus almost four-fold higher than in reticular dermis (36.4 vessels/mm2) (25). Indeed, the VD can differ to a large extent even in the same individual and by different skin layers (18, 21, 26-33) (Table IV).
Other authors used antibodies against the endothelial marker CD31 or stained tissues with haematoxylin and eosin. VD in the skin ranged between 18.3 vessels/mm2 (31) and 21 vessels/mm2 (31), whereas that in peripheral nerves was assessed as 14/mm2 (7) to 18/mm2 (27). In the present study, the mean VD was assessed as 36.9 /mm2 which was comparable to that reported for the reticular dermis (36.4 vessels/mm2) (25). Neurofibroma sub-groups presented higher mean VD than skin biopsies, however, due to a large variation in VD, a statistically significant difference was verified only between plexiform diffuse neurofibroma and skin biopsies. The VD of the different neurofibroma sub-groups in the present study was somewhat higher than in another study where we determined VD by CD34 labelling (18). Although CD34 not only labels endothelia of arterial vessels but also capillaries and venules and thus was expected to give higher values for VD, only CD34-positive structures with a patent lumen were counted, which may explain the lower VD in our previous study (18). However, the lowest VD in both our studies was measured in skin biopsies and atypical neurofibroma. Plexiform diffuse neurofibroma had the highest VD values, followed by plexiform nodular neurofibroma.
Vessel innervation. Interestingly, most authors referred to panaxonal protein PGP9.5 for determining nerve fibre density. The antibody also non-specifically marks tumours of different origin. Unfortunately, the more specific antibody to neurofilament (NF-L, 70 kDa), which is widely applied in routine diagnostics, failed to stain the nerve fibres surrounding the smallest of the vessels and thus the PGP9.5 antibodies remained the only way to investigate vascular innervation.

Vessel innervation in neurofibromatosis type 1 (NF1)-associated neurofibroma and skin biopsies. Data are the mean±95% confidence interval.
Relative vascular innervation was highest in skin biopsies of healthy individuals (13.24%) and lowest in plexiform diffuse neurofibroma (4.71%). In spite of non-specific background staining of the tumour mass, perivascular nerve fibres were clearly distinguishable in all cases. This study did not reveal any statistically significant alteration of perivascular innervation with respect to tumour type or tumour at all.
It is known that patients with NF1 may suffer from vasculopathy which manifests as arterial or venous aneurysm, arteriovenous fistula, arterial stenosis (most often of the renal arteries) or as rupture of vessels (15-17). In addition, tumour infiltration of large arteries which led to fatal haemorrhage in a patient with NF1 has been previously described (16). Although intense intraoperative bleeding is usually not due to vascular malformations, it is tempting to speculate that both vascular malformations and intraoperative bleeding have a common cause. Since we were unable to demonstrate increased VD or a decreased vascular innervation in NF1-associated neurofibroma as a cause of extensive intraoperative bleeding, this surgical problem may result from a hitherto unknown angiopathy in NF1.
Conclusion
Benign NF1-associated neurofibromas exhibit a highly variable VD which, however, does not differ from that of skin biopsies. Nerve fibre density in tumours is generally below that of controls, however, no significant differences in vascular innervation were observed between neurofibroma and controls. Hence, the well-known bleeding tendency of neurofibroma during surgical procedures may be related to alterations of the vessel not addressed in the present study.
Footnotes
↵* These Authors contributed equally to this study.
Conflicts of Interest
The Authors declare they have no conflict of interest concerning this publication.
- Received August 26, 2015.
- Revision received October 15, 2015.
- Accepted October 23, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}