


Abstract
Background/Aim: The aim of the present study was to assess clinical outcomes of postoperative radiotherapy for biliary tract cancer patients. Patients and Methods: Clinical results of 187 patients treated with external irradiation in 31 Japanese Institutions between 2000 and 2011 were retrospectively analyzed. The median radiation dose was 50.4 Gy in fractions of 1.8-2 Gy. Results: Two-year actuarial overall survival and locoregional control (LCs) rates were 56% and 68%, respectively. In multivariate analysis, macroscopic residual tumor (R2) and irradiated doses <54 Gy were significant indicators of poor LC prognosis. For patients with complete resection (R0) or microscopic residual tumor (R1), 2-year LCs were 71% for <54 Gy and 83% for ≥54 Gy; doses ≥54 Gy were associated with high long-term LCs. There was no significant difference in acute adverse event rates between <54 Gy and ≥54 Gy. Conclusion: Postoperative irradiation doses of approximately 54 Gy are safe and effective for R0 or R1 resection patients.
Primary biliary tract cancer includes gallbladder and cholangiocarcinoma. In the United States, primary biliary tract cancer accounted for 9,810 new cases in 2012 (1). Certain studies have reported that biliary tract cancer incidence was higher in East Asia, and 21,639 patients in Japan suffered from the disease in 2008 (2). The prognosis for this cancer type is poor; the 5-year overall survival rate (OS) is approximately 14% (3) because biliary cancer is difficult to detect in early stages due to poor symptoms and easy invasion of the liver, pancreas and surrounding organs (4). Therefore, biliary tract cancer patients often undergo multidisciplinary therapy, including surgery, chemotherapy, and/or radiotherapy. The only cure choice is complete resection (5). However, even after complete resection, the 5-year OS is approximately 45% (recurrence rate, >50%) (6). Several studies have reported that major relapses occur in the local primary site (7, 8). Therefore, adjuvant or neoadjuvant therapy, including radiotherapy, is important for improving treatment outcomes. A few studies in a great amount of patients assessed according to Surveillance, Epidemiology, and End Results (SEER) criteria revealed that post-surgery radiotherapy was effective for OS prolongation compared with surgery alone (9, 10). However, results based on SEER data excluded the irradiated dose information, radiation technique and important clinical information. Only few studies including a small number of patients have reported clinical results and prognosticators based on detailed patient information, including radiation dose, radiation technique, patient background and chemotherapy regimen (11-13). Although postoperative radiotherapy is an attractive approach for locoregional control (LC), the most suitable dose and its prognosticators in many patients are unknown. The Japanese Radiation Oncology Study Group (JROSG) conducted a nation-wide questionnaire-based survey on primary biliary tract cancer in 31 Institutions. Herein, we analyzed treatment outcomes and determined prognosticators using data of postoperatively-irradiated biliary tract cancer patients.
Patients and Methods
Japanese Radiation Oncology Study Group (JROSG). JROSG conducted a nationwide questionnaire-based survey on primary biliary tract cancer in 31 Institutions in Japan. All surveyed patients had the following characteristics: (i) Irradiation at the primary site between 2000 and 2011, (ii) absence of distant metastasis, (iii) absence of other malignancies and (iv) no previous irradiation. Clinical diagnostic and treatment data and patient characteristics were sent to the radiation oncology centre of JROSG. This study was conducted according to the guidelines approved by the Institutional Review Board of each Institution.
Patients. The survey included 555 patients meeting our criteria. A description of the pattern of practice for these 555 patients, but without outcome data, has been published (14). Radical or palliative biliary tract surgery was performed on 212 patients. Out of these, 25 were excluded because they underwent intraoperative or intracavitary irradiation or their treatment records were unknown. Consequently, we retrospectively analyzed the clinical results of 187 primary-tract cancer patients who underwent postoperative external irradiation. All had been diagnosed by imaging (computed tomography, magnetic resonance imaging, ultrasonography or endoscopic ultrasonography) and/or biopsies.
Our study included 133 male and 54 female patients (average age at radiotherapy=67 years; range=41-86 years) (Table I). Disease sites included 152 extrahepatic bile ducts, 20 gallbladders, 14 intrahepatic bile ducts and 1 ampulla of Vater. Histological analysis revealed adenocarcinomas in 173 patients (93%) and adenosquamous carcinomas in 4 (2%). We clinically classified primary biliary tract cancer according to the Unio Internationalis Contra Cancrum TNM Classification 6. Clinical stage II disease per the TNM classification was most common among the patients.
Treatment. Out of 187 patients, 75 (40%) underwent sequential or concurrent chemotherapy. Definitive and palliative surgeries were performed on 159 (85%) and 28 (15%) patients, respectively (Table I). Resection included complete resection (R0) in 40 patients, microscopic residual tumor (R1) in 90, macroscopic residual tumor (R2) in 36 and unknown in 21. The most common irradiation dose was 50 Gy in 25 fractions (50 patients, 32%), followed by 50.4 Gy in 28 fractions (31 patients, 17%) and 60 Gy in 30 fractions (21 patients, 11%). Irradiation was performed in multiple fields or using a conformal dynamic arc technique and Liniac with 6, 10, 18 or 20-MV photons. Three-dimensional conformal radiotherapy was used to treat 151 patients, and the others underwent two-dimensional radiotherapy. The chemotherapy regimens varied according to Institution. However, the most common regimen in 75 patients underwent chemotherapy was gemcitabine (31 patients, 41%), followed by 5-fluorouracil (20 patients, 27%).
Patients' characteristics.
The National Cancer Institute's Common Terminology Criteria for Adverse Events version 4.0 is the preferred method for capturing adverse events after all cancer treatments.
Statistical analysis. OS, progression-free survival (PFS) and LC rates were actuarially calculated using the Kaplan–Meier method. We defined OS as the time from irradiation to death or the last follow-up. PFS was defined as the time from irradiation to disease progression, death or the last follow-up. Locoregional control was defined as the time from irradiation to the date of local or regional relapse. We performed univariate and multivariate analyses using the log-rank test and Cox proportional hazards model, respectively, to determine OS, PFS, or LC prognosticators (JMP statistical software; version 9.0). Statistical significance was set at <0.05.
Results
Survival and prognostic factors. On the last observation day, 90 patients had survived and 97 had died. Median follow-up time was 14.8 months (range=1-99.6). The 2- and 5-year OS rates were 56% and 22%, respectively (Figure 1a), and the 2- and 5-year PFS were 36% and 19%, respectively (Figure 1b). Median OS and PFS were 15 and 9.5 months, respectively. We performed univariate analysis to explore potential prognosticators for OS, PFS and LC rates (Table II). The results showed that resection type (OS: p<0.001; PFS: p=0.005), PS (OS: p=0.034; PFS: p=0.009), clinical T stage (OS: p=0.014; PFS: p=0.041), clinical N stage (OS: p<0.001; PFS: p<0.001) and TNM classification (OS p=0.044; PFS: p=0.027) were common significant prognosticators for both OS and PFS and that sex (p=0.045) and age (p=0.015) were significant prognosticators for OS alone. In univariate analysis, concurrent chemotherapy was not a significant prognosticator for OS or PFS. Jaundice and subsites of biliary tract cancer were not significant prognosticators. In multivariate analysis, R2 (OS: p=0.0003; PFS: p=0.0068), PS ≥2 (OS: p=0.0165; PFS: p=0.0077) and TNM stage (OS: p=0.0131; PFS: p=0.0017) were common significant prognosticators for OS and PFS (Table III). Age ≥75 years (p=0.0052) was the only significant prognosticator for OS.
Locoregional control and prognostic factors. After irradiation, recurrence was observed in 97 patients (52%) (Table IV). Relapse data were unavailable for 28 patients. Forty-six patients (25%) experienced recurrence at the primary site or distant metastasis, respectively. Five patients (3%) experienced recurrence at both the primary site and distant metastasis. The 2- and 5-year LC rates were 68% and 44%, respectively (Figure 1c). Median LC was 12 months. Univariate analysis showed that clinical N stage (p=0.007) was the only significant prognosticator for LC (Table II). In multivariate analysis, R2 (p=0.0421) and irradiated doses <54 Gy (p=0.0396) were poor significant prognosticators for LC (Table III).
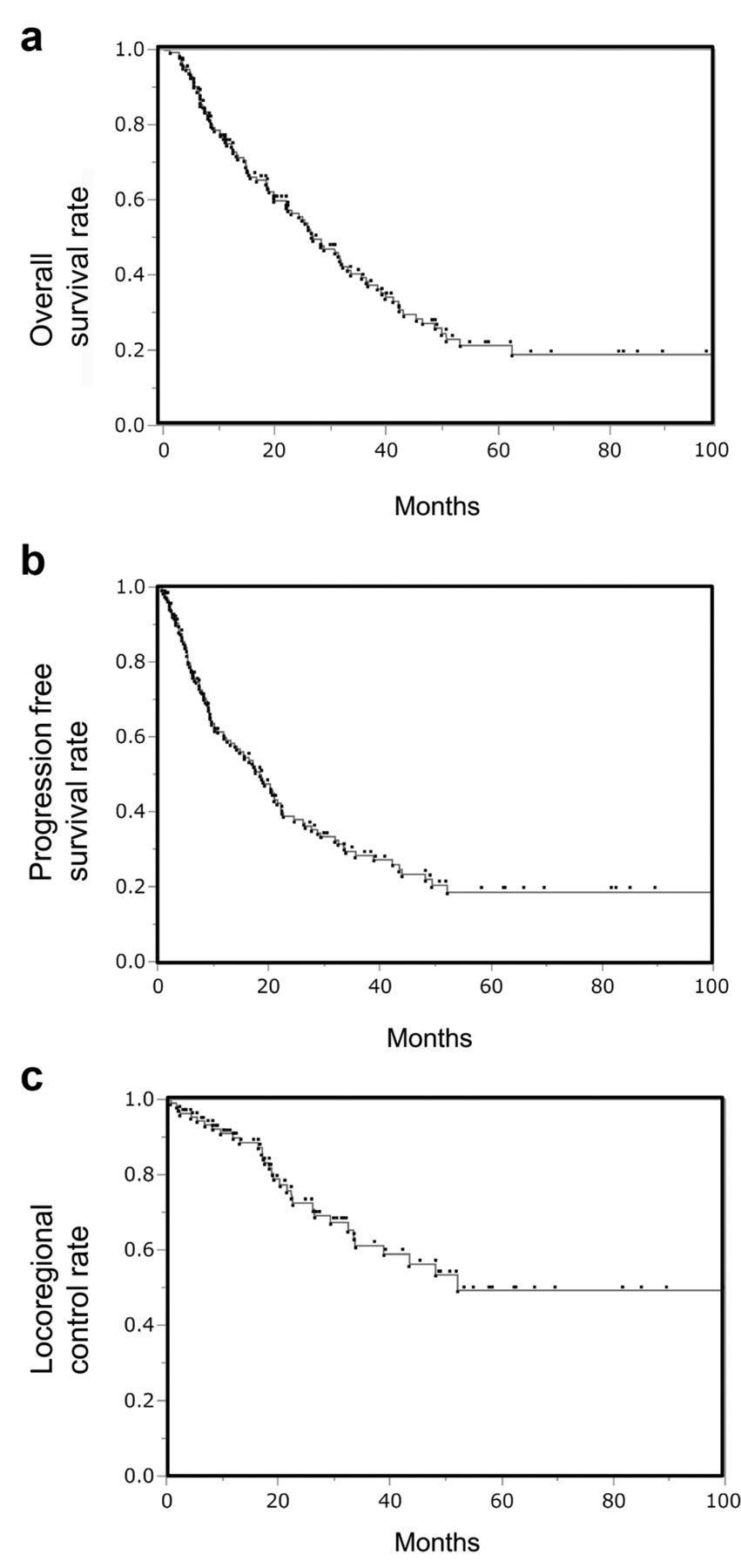
Overall survival rate (a), progression-free survival rate (b) and locoregional control rate (c).
Next, we focused on the irradiated dose impact (<54 Gy/≥54 Gy) on the resection type (R0/R1 or R2). For patients with R0/R1, the 2- and 5-year LC rates were 71% and 42%, respectively, for <54 Gy, and 83% and 83%, respectively, for ≥54 Gy (p=0.1224) (Figure 2a). Although the LC rate of the <54-Gy group decreased during the follow-up period, it remained high in the long term in the ≥54-Gy group. For R2 patients, the 2-year LC rate was 50% for <54 Gy and 60% for ≥54 Gy (p=0.3515) (Figure 2b). For R2 patients, the 5-year LC rate could not be calculated because the follow-up period was less than 5 year.
Univariate analysis of overall survival, progression-free survival and locoregional control rates.
Adverse events. Table V shows all adverse events equal to or greater than grade 3. There were no grade 5 complications. Out of acute hepatobiliary disorders, cholangitis, which seemed to have been caused by stenosis of the postoperative bile duct, occurred in 8 events. Although radiotherapy was suspended in 1 patient, other patients could complete radiotherapy including a temporary interruption. Out of 9 patients with haematological disorders, 8 developed leukopenia and 1 developed pancytopenia; 8 of these 9 patients underwent chemotherapy. Although radiotherapy was suspended in 1 patient, the other patients could complete radiotherapy including a temporary interruption. Gastrointestinal adverse events included one case each of gastritis and pancreatitis. Radiotherapy in both patients was suspended. There was no significant difference in the acute adverse event rates between the <54-Gy and ≥54-Gy groups. Two patients developed late gastroduodenal ulcers; both were irradiated with 60 Gy and were not administered chemotherapy. Ten percent of the patients irradiated with 60 Gy suffered late gastroduodenal ulcers. However, none occurred in patients irradiated with doses <60 Gy.
Discussion
JROSG conducted a nationwide multi-centre survey on primary biliary tract cancer, and the clinical results of 187 patients underwent postoperative external irradiation in 31 Institutions in Japan were retrospectively analysed. In previous studies, OS and PFS rates were 11%-42% and 27%, respectively, at 5 years (9, 10, 12, 13, 15-19). Our 5-year OS and PFS rates of 22% and 19% were approximately comparable to those of previous studies. Certain studies revealed that significantly independent poor prognosticators for OS were age ≥75 years, R2, PS ≥2 and TNM stage classification ≥II. Similarly, some studies showed that R2, PS ≥2 and TNM stage classification ≥II were significantly independent poor prognosticators for PFS. Therefore, in this study, age and PS for OS and resection type, performance status and TNM stage for PFS were identified as new prognosticators.
Our results showed that 46 patients (25%) experienced recurrence at the locoregional site. This was approximately consistent with previous reports wherein LC rates were 30%-65% (7, 8, 20). Multivariate analysis of patients undergoing postoperative radiotherapy revealed that the significant poor prognosticators for LC were R2 and irradiated doses <54 Gy. No studies have reported prognosticators for LC in patients undergoing postoperative radiotherapy; however, Tae et al. found that the use of N stage, perineural invasion and postoperative chemoradiation were significantly associated with LC in biliary tract cancer patients undergoing resection alone or postoperative chemoradiation (21). Therefore, the present study identified new prognosticators for LC.

Comparison of locoregional control rate curves between irradiated doses <54 Gy and ≥54 Gy. Complete resection and microscopic residual tumor group (a), macroscopic residual tumor group (b).
Multivariate analysis of overall survival, progression-free survival and locoregional control rates.
Recurrence patterns.
We also found that, for R0/R1 patients, the LC rate was higher for the ≥54-Gy group than for the <54-Gy group, using the Kaplan–Meier method, although the difference was not statistically significant. The lack of a statistically significant difference in LC rates between the 2 groups may have been due to selection bias. Additionally, our results showed that, for R0/R1patients, the LC rate of the ≥54-Gy group remained high in the long term. Conversely, for R2 patients, the LC rate of the ≥54-Gy group was similar to that of the <54 Gy group. These results indicated that an irradiated dose ≥54 Gy was effective for microscopic residual tumors but insufficient for macroscopic residual tumors. Several studies in primary biliary tract cancer patients who underwent postoperative external irradiation have reported that the irradiated doses ranged from 45–50.4 Gy, and a few studies based on SEER data excluded the irradiated dose information (9-13, 15-17, 19, 21). Therefore, it was unclear how irradiated doses >50.4 Gy affected LC. In this study, the finding that irradiated doses ≥54 Gy enabled long-term LC is new and can be used to benefit R0 or R1 resection patients.
Treatment-related adverse events (≥grade 3),
In the present study, approximately 13% of patients experienced acute toxicities (≥grade 3) and 1% experienced late toxicities (≥grade 3). There were no grade 5 complications. These results were almost tolerable and consistent with those of a previous study (22), although our study included patients irradiated with doses >50 Gy. There was no difference in the acute adverse event rates between the <54-Gy and ≥54-Gy groups. Ten percent of patients irradiated with 60 Gy suffered late gastroduodenal ulcers, but none occurred in patients irradiated with doses <60 Gy. These results suggest that postoperative irradiation doses of approximately 54 Gy are safe and effective for R0/R1 resection patients.
Our JROSG study had 2 limitations as a consequence of performing a nationwide retrospective survey on postoperatively irradiated patients with primary biliary tract cancer in 31 Institutions between 2000 and 2011. First, operability included a selection bias. Second, the patient characteristics, chemotherapy regimen and radiation technique varied among the Institutions and time periods.
In conclusion, the present study identified R2 and irradiated doses <54 Gy as significant predictors of poor LC in biliary tract cancer patients, and the results suggested that postoperative irradiated doses of approximately 54 Gy are safe and effective for R0/R1 resection patients. Our study was a retrospective analysis, and further prospective studies on the topic are warranted.
Footnotes
Conflicts of Interest
The Authors declare that they have no competing interests.
- Received July 18, 2015.
- Revision received September 21, 2015.
- Accepted September 23, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}