


Abstract
Dermatofibrosarcoma protuberans (DFSP) is an uncommon cutaneous sarcoma with high recurrence rate. Radical surgery is the treatment of choice, although in cosmetically-sensitive areas such as the head and neck, this option is often not pursued. Electrochemotherapy (ECT) is a minimal invasive anti-tumor modality which is increasingly being used to treat skin metastases from different malignancies. A 31-year-old woman presented with subcutaneous local multirecurring DFSP located at the proximal end of the left eyebrow. ECT was offered as a palliative treatment to avoid radical disfiguring surgery. Two days following ECT, the patient was discharged in good general health. Partial tumor regression was appreciable at two months' follow-up by ultrasound and magnetic resonance imaging. At six months, residual fibrotic tissue was observed; at three years, no evidence of the tumour was detected. In our case, ECT achieved good local tumor control with excellent cosmetic results, preserving the patient's quality of life.
Dermatofibrosarcoma protuberans (DFSP) is a rare, dermal low- to intermediate-grade soft-tissue sarcoma. It has a high rate of recurrence and aggressive local growth within the subcutaneous tissue fascia and underlying muscles but distant metastasis is uncommon (1). The incidence of DFSP is approximately 0.1% of all tissue cancer and 1% of all soft-tissue sarcomas. DFSP usually involves the trunk of the body and proximal extremities but it is also rather frequent in the head and neck area, accounting for up to 6% of sarcomas in this location (2). Wide local surgical resection with recommended surgical margins of 3-4 cm, when feasible, represents the standard treatment for DSFP (3). Larger margins, including skin, subcutaneous tissue and underlying fascia, produce better clearance rates. Unfortunately, such margins are not possible when DSFP involves the face.
Electrochemotherapy (ECT) is a safe, simple non-thermal anti-tumor modality that combines the local application of electric pulses (electropermeabilization) and low dosage chemotherapy in order to facilitate the delivery into the tumour cell of otherwise non-permeant anticancer drug and increase local antitumor activity (4). ECT has proven highly effective for the treatment of cutaneous and subcutaneous tumours, regardless of their histological origin (5, 6). We report here our experience using ECT to treat biopsy-proven DFSP in a patient unsuitable for surgery.
Case Report
A 31-year-old woman presented at the San Gallicano Institute in December 2011 with subcutaneous local recurrence of DFSP on the left orbital margin. The patient's clinical history started in 1999 when she was first admitted to a different institution for multiple neoplasms in the forehead region. Histopathological examination showed well-differentiated benign fibroblastic proliferation, which in some areas involved adipose tissue in accordance with a fibrous histiocytoma medical description. The patient underwent surgical resection of the tumor subcutaneously. Two years later she was diagnosed with multiple lesions from DFSP in the region of the previous surgery and underwent large excision of the neoplasms below the frontal plane and reconstruction with local flap and skin graft. The immunohistochemical examination of the deep resection margins confirmed the diagnosis of DFSP, showing positive reaction for CD34 and negative for S100, and revealed inadequate deep surgical margins and incomplete tumoural resection. Computed tomographic (CT) scans of the head showed a thin filling and thickening of the soft parts at the front-right paramedian-median location, which at depth did not seem to match any alteration of the cranial plate. No other localization of the neoplasia was detected. Therefore, further wide excision along with radial forearm free-flap reconstruction was undertaken to ensure adequate clearance; however, immunohistochemical analysis of the resected specimen showed that the deep surgical margins were still positive for tumour markers.
In late 2011, 10 years following the third surgery, the patient was admitted to our institute. CT scans revealed the presence of recurring subcutaneous neoplasms at the proximal end of the left eyebrow, covering an area of about 2 cm in diameter and ending on the underlying plane. Chest X-ray was negative for evidence of metastatic disease. CT scan demonstrated the presence of recurrent neoplasm, while no tumoural infiltration of the deep planes was shown (Figure 1). The overlying skin was apparently clear of the disease and painless.
Standard radical surgery would have required extensive resection of the whole ocular area, with wide safety margins of the tumoral mass, including most of the orbital floor and this was refused by the patient. On the other hand, previous more conservative surgical interventions had not provided complete removal of the tumour. Thus, ECT was offered as a palliative treatment to avoid major disabling surgery and to preserve the patient's quality of life. The patient gave their informed consent to the procedure. The treatment was performed under general anaesthesia in accordance with the European Standard Operating Procedures on Electrochemotherapy (7). Bleomycin (Sanofi-Aventis S.p.A., Milano, Italy, vials of 15 mg) was administered intravenously at a dose of 15,000 UI/m2. Electrical pulses were applied to the tumoral area 8-28 min following intravenous injection of bleomycin. Type II linear configuration electrodes were used. Electrical pulses (eight pulses of 100 ms duration) were delivered using a square wave pulse generator (Cliniporator, IGEA S.p.A., Carpi, Italy). The applied voltage amplitude was 1000 V/cm (voltage to electrode distance ratio). The pulses were applied at a frequency of 5 kHz. The area including the subcutaneous tumorous lesion, the flap and 4.5 cm tumour-free margin was treated by multiple adjacent insertions of the electrode to safely cover the whole tumorous lesion. A biopsy (9 mm × 4 mm) of the lesion was taken before ECT treatment. Histopathological analysis showed uniform, small spindle cells with plump nuclei intersected in irregular whorled fascicles to form the typical storiform pattern. Tumour cells insinuated between the fat cells in the subcutaneous tissue and surrounded dermal appendages, without invasion compatible with DFSP. Immunohistochemistry showed positive reaction for CD34 (Figure 2).

Cranial computed tomographic examination of the patient performed without contrast medium before electrochemotherapy treatment. Axial plane (A), reconstruction in sagittal plane (B) and 3D reconstruction for soft tissue (C) images showing thickening of the subcutaneous fat plane in the frontal region above the orbital plane without evidence of lytic tumorous area in the bone structure.

Histological analysis of the lesion. Proliferation of monomorphic spindle cells invading the dermis and subcutaneous tissue (H&E staining; ×40) (A); interwoven fascicles of small spindle cells arranged in a swirling or storiform pattern (H&E staining; ×100) (B); highly packed tumor cells insinuated between the fat cells in the subcutaneous tissue (H&E staining; ×200) (C); immunohistochemistry staining showing that CD34 is diffusely expressed in the dermatofibrosarcoma protuberans components (×200) (D).
According to the Common Terminology Criteria for Adverse Events (version 4.3) (8) no serious ECT-related adverse events were observed. After the treatment, the patient developed grade 1 cutaneous toxicity that included modest oedema, mild skin necrosis and a transient palpebral bruise. The patient reported mild pain which resolved in 3-4 days without pain medication. Postoperative therapy included amoxicillin and clavulanic acid. Skin care consisted of application of betamethasone dressing. The patient was discharged two days following ECT treatment in good general condition.
At 6 months after ECT, examination by ultrasound and magnetic resonance imaging (MRI) revealed the presence of little residual tissue, suspicious of fibrosis, of about 25% in volume of the initial tumoral formation. At later follow-up visits, performed every six months for three years, imaging evaluations showed further reduction of the residual neoplastic tissue until final disappearance of the lesion at the last visit at 42 months following ECT (Figure 3).
Discussion
DFSP is a locally invasive dermal mesenchymal neoplasm. It is most common among young adults between the third and fourth decades of life, with a slight predominance in males (1). DFSP has slow-growing behaviour, with a marked tendency for local recurrence due to its strong capacity to infiltrate subcutaneous tissue and muscle (2). The treatment option for DFSP is primarily surgical. The accuracy of the initial surgical procedure is the main prognostic factor for locoregional recurrence, with a risk of 60% after conventional surgery, decreasing to 10% when margins are larger than 4 cm (3). In addition, the frequency of recurrence has been shown to be correlated with the number of previous surgical attempts and not the size of the original tumor (9). Notably, the head and neck area is a more common site for recurrence, likely reflecting the difficulties in excising DFSP located across this area for cosmetic and organ-saving reasons (10).
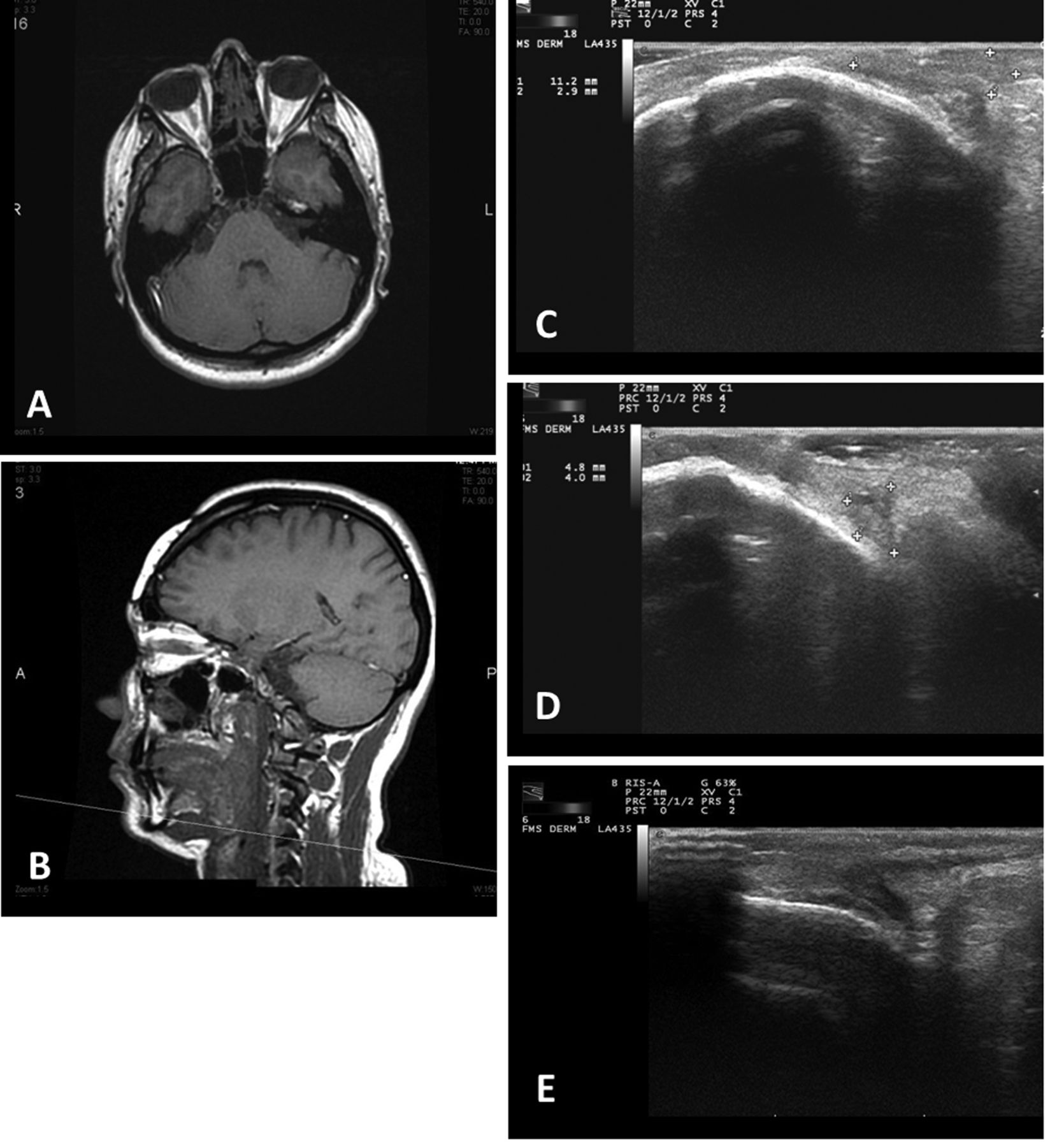
Imaging examination of tumor response to electrochemotherapy (ECT). Axial plane (A) and sagittal plane (B) of magnetic resonance imaging scan showing only minimal alteration of the soft tissue at the lesion site immediately post treatment. Ultrasound imaging revealed residual fibrous tissue at 2 months (C) that decreased at 24 months (D) and had disappeared at 42 months (E) following ECT.
In experienced hands, Mohs micrographic surgery, which allows examination of all surgical margins to minimize the amount of resected tissue, has been reported to reduce the recurrence risk rate to 2-5% (3, 9, 11). Surgical treatment of DFSP in the head and neck region performed with wide margins of resection often involves problematic reconstruction due to the presence of different structures and tissues over multiple aesthetic units of the face. When choosing for the appropriate method, the reconstructive use of local flaps is often rejected because of the low capacity to fill a large loss of substance, while skin grafts, although having the ability to bridge large gaps, have limited coverage of the underlying structures and, no less importantly, they fail to achieve a quickly acceptable aesthetic result. The use of expanded flaps is a valid reconstructive option but it involves long set-up times and the ontologically disputed carrying out of migration in the presence of the tumour. In certain cases, the alternative option may be the direct use of skin grafts (along with the removal of the tumor) for the time necessary to the preparation of the expanded flaps. Free flaps most frequently represent the ideal reconstructive choice, as was the case of our patient, but they require a microsurgical team, good physical condition of the patient, and that the patient accepts the long operating times and the possibility of failure (12). Indeed, our patient refused to undergo further invasive disfiguring surgery and additional time-consuming free flap reconstruction. Therefore, ECT was offered as the last treatment option with palliative intent.

Recurrent dermatofibrosarcoma protuberans located on the orbital margin treated by electrochemotherapy (ECT). Baseline presentation: surgical margins drawn before starting ECT (A); after ECT at 2 months (B), 24 months (C), and 42 months (D).
ECT is an easy to perform, safe, tumour ablation that is effective on any type of solid tumour, including primary skin cancer (e.g. squamous cell and basal cell carcinomas, and Kaposi sarcoma) and cutaneous metastases from different histotypes (e.g. melanoma and breast cancer) (5).
Currently, ECT is recognized as a valid option for the management of superficially disseminated metastases when surgery is not possible because of the number of lesions or their localization (13, 14), as an organ-sparing treatment of non-operable skin primary tumours or relapses (14-16), for tumours refractory to conventional treatments such as radiotherapy (5), and as a cytoreductive procedure before surgical resection (17). ECT is largely used as palliative therapeutic approach in patients with primary and recurrent head and neck tumours who are not candidates for standard treatments because of advanced age, performance status, comorbidities or when cosmetic, visible areas are involved (18, 19).
In our case, the ECT procedure was feasible and well-tolerated. It was decisive in controlling the disease using a single course of treatment, with minimal operating time, and minimal side-effects. Three years following ECT, no recurrences have been noted (Figure 4). In the standard management of head and neck cancer, in view of good control of the disease, in order to achieve a cosmetically acceptable result, a reconstruction must be usually performed. In our case, ECT obtained good local tumour control with an excellent cosmetic result, without reconstruction, greatly preserving the patient's quality of life.
In conclusion, ECT was demonstrated to be a valuable locoregional treatment and a beneficial non-invasive alternative in skin-directed therapies for cutaneous and subcutaneous neoplasia located in the head and neck region.
- Received July 27, 2015.
- Revision received September 8, 2015.
- Accepted September 16, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.