


Abstract
Background/Aim: The cell surface receptor programmed death-1 (PD1) and its ligand (PDL1) have been detected in various cancer types. It has been reported that expression of PDL1 and PD1 in a tumor is associated with poor prognosis of the patient. In the present study, we retrospectively examined tumor expression of PDL1 and intratumoral PD1+ cell infiltration, and assessed their relationship with patient prognosis according to the pathological stage of gastric cancer. Materials and Methods: PDL1 and PD1 expression in primary tumors from 431 patients was evaluated using immunohistochemistry. The association between the expression of PDL1/PD1 and clinicopathological features was assessed. Results: High expression of PDL1 was observed in 128 (29.6%) patients. PDL1 expression was correlated with tumor infiltration of PD1+ cells. In multivariate analysis, PDL1 expression was associated with worse overall survival. In subset analysis, PDL1 expression was significantly associated with survival in patients with stage II/III gastric cancer. In conclusion, PDL1 was an independent prognostic factor for patients with stage II/III gastric cancer. Our results suggested that patients with stage II/III gastric cancer might be appropriate for PD1/PDL1-targeted therapy.
Surgical resection with lymphadenectomy is the standard treatment for patients with stage II/III gastric cancer. In Japan, postoperative adjuvant chemotherapy is considered effective for stage II/III gastric cancer. However, recurrent disease after surgery is observed in 30% of patients with stage III disease (1). Thus, more aggressive therapy after surgery, including a combination of chemotherapeutic agents or molecular-targeted therapy, is required (2).
Cell-surface molecule programmed death 1 (PD1) inhibits T-cell co-stimulation and is a key molecule in the regulation of peripheral immunotolerance (3, 4). PDL1, which is one of a number of PD1 ligands, has a much broader tissue distribution than PD1 and can deliver inhibitory signals to PD1+ T-cells to suppress immune responses (4, 5). PDL1 is widely expressed in cancer, where it contributes to immune evasion and facilitates tumor growth (6). Recently, targeting the inhibitory PDL1/PD1 interaction using a monoclonal antibody was shown to result in striking antitumor activity in patients with melanoma in a phase I study (7, 8).
We previously showed that gastric cancer cells have the potential to react with cytotoxic T-lymphocytes (9). Furthermore, we showed that immunochemotherapy after surgery might be effective for patients with gastric cancer lymph node metastasis (10). Thus, gastric cancer cells may be immunogenic and the clinical effect of an antibody to PD1 antibody on the survival of patients with gastric cancer may possibly be shown in the near future. The aim of the present study was to investigate the impact of the expression of PDL1 and PD1 in tumors on the survival of patients with gastric cancer in order to determine which patients might be appropriate for immune checkpoint-targeted therapy.
Materials and Methods
Clinical samples. Tumor samples were obtained from 431 patients (mean age=66 years) who underwent surgical resection for gastric cancer without preoperative chemotherapy at the Department of Surgical Oncology, Osaka City University Hospital, between 1997 and 2010. Tumors were diagnosed histologically based on the Third Edition of the Japanese Classification of Gastric Carcinoma (11). Informed consent was obtained from all patients.
Immunohistochemistry. Tumor specimens in paraffin-embedded blocks were cut into 4-μm-thick sections. For antigen retrieval, the samples were autoclaved in 0.01 M citrate (pH 6.0) at 121°C for 15 min. The samples were then deparaffinized in xylene and rehydrated using a graded series of ethanol. The slides were then washed twice for 5 min per wash in phosphate-buffered saline (PBS). Endogenous peroxidase activity was blocked with absolute methanol containing 3% hydrogen peroxide for 15 min. After washing in PBS, the samples were microwaved for 10 min for the purpose of antigen retrieval. Nonspecific binding was blocked using a non-specific staining blocking reagent (Dako, Kyoto, Japan). The samples were then reacted with rabbit polyclonal anti-PDL1 (#58810, 1:50 dilution; Abcam, Tokyo, Japan) or with mouse monoclonal anti-PD1 (#52587, 1:50 dilution; Abcam) at 4°C overnight, and were subsequently washed with PBS for 10 min. The samples were then incubated with secondary antibodies for 10 min at room temperature. The secondary antibody was a biotin-labeled goat anti-rabbit IgG (1:500; Nichirei, Tokyo, Japan) for anti-PDL1 and a biotin-labeled rabbit anti-mouse IgG+IgM+IgA (1:500, Nichirei, Tokyo, Japan) for anti-PD1. After washing in PBS, signals were visualized by incubation with 3-3’-diaminobenzidine for 5 min, and the slides were counterstained with hematoxylin before mounting. All reactions were performed using appropriate positive and negative controls. The expression of PDL1 was evaluated according to the percentage of the stained cell. We defined samples with less than 10% of positive cells, 10-50% of positive cells, more than 51% of positive cells as weak, moderate, strong expression respectively. For analysis of the expression of PD1, the total number of PD1+ cells was counted in three high-power fields (HPFs) within tumor samples. Samples with a mean of more than five PD1+ cells were classified into a high-infiltration (PD1 high) group. Two experienced investigators, who were blinded to the clinical follow-up data, independently analyzed the expression of these molecules.
Statistical analysis. The Mann–Whitney test was used to assess the associations between the expression of PDL1 and PD1 and clinicopathological features. Correlation of tumor PDL1 expression with infiltration of PD1+ cells was investigated by using the Wilcoxon rank sum test.
The Kaplan–Meier method was used to construct the overall survival curves and a log-rank test was used to assess the significance of differences in survival. A Cox proportional regression model was used for univariate and multivariate analyses of prognostic factors. A p-value of less than 0.05 was considered statistically significant. Each statistical analysis was performed using JMP software (SAS Institute, Cary, NC, USA).
Results
Expression of PDL1 and PD1 in gastric cancer. In total, 431 patients with gastric cancer who underwent surgical resection were included in the study. The characteristics of the patients are summarized in Table I. The median follow-up time was 34 months. Out of these patients, 165 were diagnosed with stage II/III disease and 27% of these had received postoperative adjuvant chemotherapy.
Immunohistochemical staining detected PDL1 in the cytoplasm of tumor cells (Figure 1A-C). Strong staining of PDL1 was present in 128 (29.6%) and weak staining was observed in 113 (27.3%) of the tumor samples. The remaining samples showed moderate PDL1 staining. Strong staining of PDL1 was significantly associated with depth of invasion (pT), lymphatic invasion, venous invasion, lymph node metastasis, and pathological stage (Table II). No significant association was detected between PDL1 staining level and histology or macroscopic type. PD1 was detected in stromal lymphocytes (Figure 1D and E). With regard to PD1 expression, a cut-off of 5, the median number of PD1-positive cells, was used to define ‘low’ versus ‘high’ expression. PD1 expression was significantly higher in tissues with lymph node metastasis, serosal invasion and late pathological stage than in tissues without lymph node metastasis or early stage cancer (Table II). No significant difference was observed in PD1 expression level by histological type. Strong staining of PDL1 was associated with high infiltration of PD1+ cells. Out of 128 tumors with strong staining of PDL1, 96 (75%) had a high density of PD1+ cells. In contrast, in tumors that were weak for PDL1 staining, the percentage of tumors with a high density of PD1+ cells was only 26.5%. A significant positive correlation was observed between PDL1 expression and PD1+ cell infiltration (Figure 2).
Summary of patient characteristics (N=431).
Impact of PDL1 and PD1 expression on the survival of patients with gastric cancer. We evaluated the effect of PDL1 and PD1 expression in the primary tumor on patient prognosis. In this analysis, we also defined strong staining of PDL1 as positive and defined moderate and weak staining of PDL1 as negative for PDL1 expression. With regard to PD1, we defined high infiltration as positive and defined low infiltration as negative. Univariate Cox regression analysis showed that poor tumor differentiation, lymph node metastasis (pN), depth of invasion, PDL1 expression and PD1 infiltration were negative prognostic factors for patients overall (Table III). In multivariate analysis, pT, pN, lymphatic invasion and PDL1 expression were independent prognostic factors (Table III).
Correlation of PD1 and PDL1 expression with clinicopathological features of patients with gastric cancer.
Overall survival according to PD1 and PDL1 expression is shown by Kaplan–Meier curves in Figure 3. Patients with strong staining of PDL1 in tumor had significantly poorer prognosis compared to patients with weak staining (Figure 3A). With regard to PD1, patients with a high level of PD1+ cell infiltration had a worse prognosis compared to those with a low level of infiltration (Figure 3B). As shown in Figure 3C, the overall survival of patients whose tumors were positive for both PDL1 and PD1 was significantly worse than that for patients whose tumors were negative for both molecules, indicating that a positive relationship between PDL1 and PD1 could reflect on prognosis. In sub-group analysis based on pathological stage, PDL1 expression was not associated with prognosis in stage I and IV; however, it was significantly associated with overall survival in stage II/III cancer (Figure 4). The survival rate at 1, 2, and 5 years following gastrectomy was 91.9%, 67.0% and 33.2%, respectively, for patients with strong tumor PDL1 staining compared with 90.9%, 85.4% and 69.2%, respectively, for patients with weak staining. In multivariate analysis, PDL1 expression was an independent prognostic factor for gastric cancer patients with stage II/III cancer (Table IV).
Discussion
In the present study, we obtained the following findings. First, weak tumor staining of PDL1 was associated with significantly better overall survival than strong tumor staining of PDL1 in patients with gastric cancer. Secondly, expression of PDL1 in the primary tumor was correlated with tumor-infiltrating PD1+ cells. Thirdly, we showed that PDL1 expression was an independent prognostic factor for patients with stage II/III cancer who underwent curative resection surgery. Our results suggest that PDL1 expression might be a good prognostic factor for consideration of immunotherapy using an immune checkpoint antibody for patients with stage II/III gastric cancer.

Immunohistochemical staining for programmed death-1 ligand-1 (PDL1) and programmed death-1 (PD1) in gastric cancer tissue. A-C: Representative immunohistochemical staining for PDL1 expression in gastric cancer. Samples were divided into three groups according to the intensity of PDL1 expression: weak (A), moderate (B), and strong (C) staining of PDL1 (at ×400 magnification). D and E: Representative immunohistochemical staining for PD1+ cells infiltrating gastric cancer tissue: low infiltration (D) and high infiltration (E) (original magnification ×200).
It has been demonstrated that tumor cells are capable of up-regulating their expression of PDL1, thereby providing inhibitory signals to suppress the cytotoxic activity of CD8+ T-cells (12). Although the precise mechanism by which intra-tumoral PDL1 worsens a patient's prognosis remains to be determined, PDL1 has been reported to be expressed in different cancer types including in breast, ovarian, pancreastic, esophageal, colorectal and gastric cancer (6, 13, 14-16). Furthermore, PDL1 expression by tumor cells has been reported to strongly correlate with poor prognosis (14).
We previously reported that immunosuppressive status within a tumor was associated with progression of gastric cancer (17, 18). In addition, we showed that immunotherapy might be effective for gastric cancer (10). We, therefore, hypothesized that gastric cancer may be relatively immunogenic. Our study showed that the expression level of PDL1 was significantly correlated with the density of PD1+ cell infiltration. Saito et al. demonstrated very high up-regulation of PD1 expression on T-cells in gastric cancer tissue and they suggested that the cancer cells themselves could affect PD1 and PDL1 expression in the local environment (19). Our results suggest that PD1 on the surface of intra-tumoral infiltrated T-cells might be induced in response to an inflammatory environment that is created by cancer cells.
Univariate and multivariate Cox regression analysis of clinicopathological and molecular features for overall survival in patients with gastric cancer.
Univariate and multivariate Cox regression analysis of clinicopathological and molecular features for overall survival of patients with stage II/III gastric cancer.
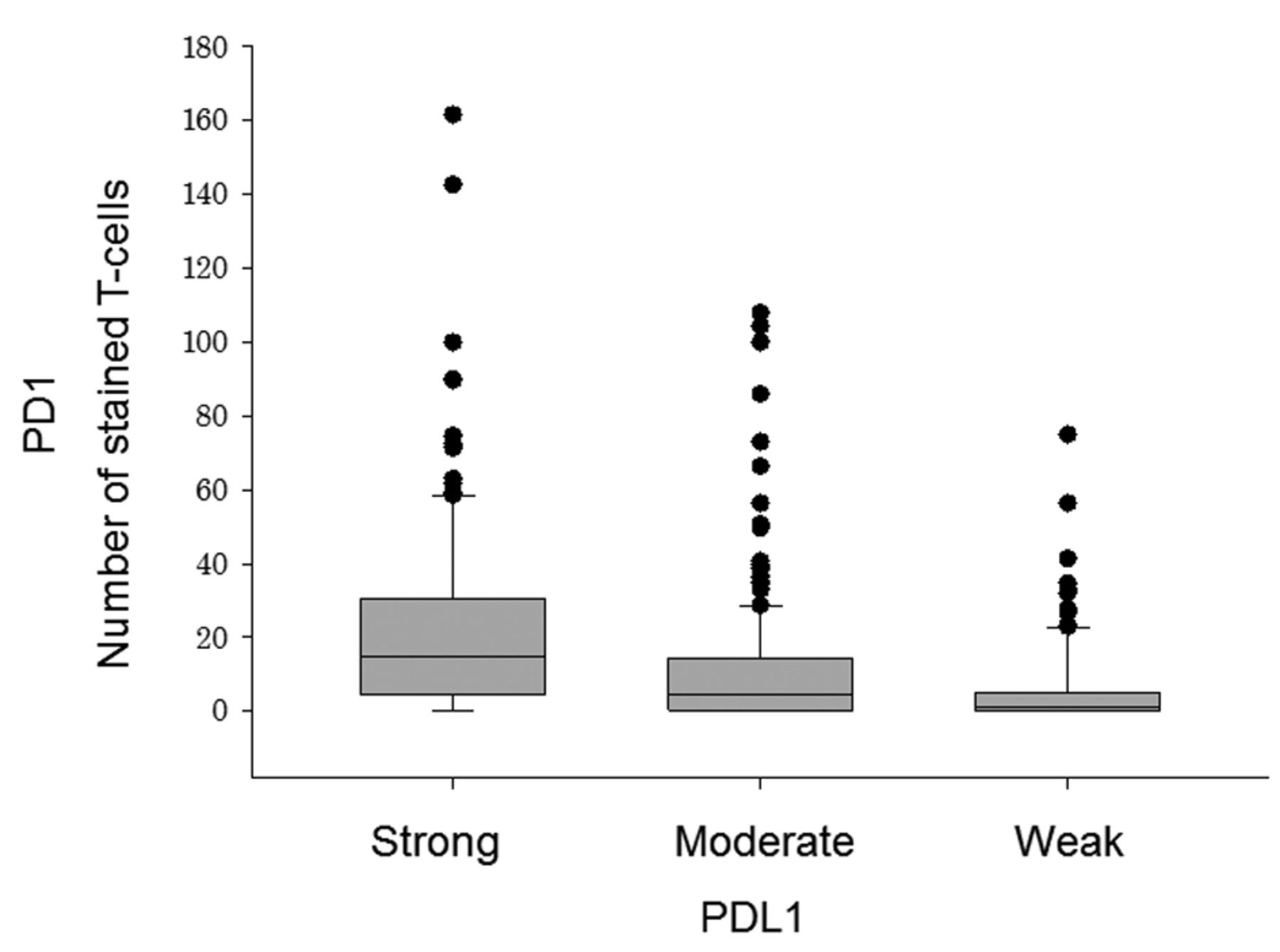
Correlation of tumor Programmed Death-1 Ligand-1 (PDL1) expression with infiltration of programmed death-1 (PD1)-positive cells. The number of stained PD1+ T-cells within tumors with high, moderate, and weak staining of PDL1 was plotted. Each box indicates the first and upper quartiles, and the bar in each box indicates the median value. The number of PD1+ cells significantly increased according to the intensity of PDL1 staining. ***p<0.0001.
Immune checkpoint blockade with monoclonal antibodies directed at PD1 and PDL1 has emerged as a treatment for patients with advanced melanoma (7). As the population of patients who attain clinical benefit is relatively small, identification of a biomarker for response to this immunotherapy is critical. PDL1 expression has been considered as a predictive marker for tumor response to PD1 antibody treatment. Indeed, PDL1 expression is one of the eligibility criteria in the clinical study of PD1 antibody immunotherapy for several types of cancer. Although the safety and the efficacy of anti-PD1 treatment has been demonstrated in patients with advanced non-small cell lung cancer in a phase I study, the efficacy of such immunotherapy for gastric cancer has not been elucidated (20). We found a strong prognostic impact of PDL1 expression in pathological stage II/III cancer. Over 30% of patients with pathological stage II/III cancer often have recurrent disease after gastrectomy due to remnant cancer cells (1). Our results suggest that remnant tumor cells with low PDL1 expression might be attacked by tumor-specific cytotoxic T-cells after surgery, resulting in longer patient survival.
Our study has several limitations. One is the definition of PDL1 positivity. Distinction between PDL1 staining patterns (for example, membranous or cytosolic) and determination of cut-off values for the percentage of stained cells were difficult. Nevertheless, we showed that there were significant differences in overall survival among patients whose tumors were positive for both PD1 and PDL1 expression, were positive for either molecule, or were negative for both molecules, by examination of PD1 and PDL1 expression in the same section. Another limitation is that there may be a bias in the selection of patients since this was a retrospective study. In order to minimize such a potential bias, we did examine 431 consecutive samples.

Survival curves for patients with gastric cancer with different expression levels of programmed death-1 ligand-1 (PDL1) and Programmed Death-1 (PD1). The overall survival of patients with the indicated expression of PDL1 (A), PD1 (B), or combinations of PD1 and PDL1 expression (C), is indicated using Kaplan–Meier curves. The p-value was determined using the log-rank test. Patients with strong PDL1 staining had a poorer prognosis than those with weak or moderate PDL1 staining (A). Patients with high PD1+ cell infiltration had a poorer prognosis than those with low PD1+ cell infiltration (B). Patients that were negative for both PD1 and PDL1 had a better prognosis than patients that were positive for both molecules (C).

Survival curves according to programmed death-1 ligand-1 (PDL1) expression in different pathological stages of gastric cancer. The overall survival of patients with weak or strong PDL1 staining in pathological stage I (A), II (B), III (C), IV (D) or II/III (E) gastric cancer is indicated using Kaplan–Meier curves. The p-value was determined using the log-rank test. Patients with strong PDL1 staining had a worse prognosis compared to those with weak PDL1 staining in pathological stage II/III cancer.
In conclusion, PDL1 was found to be an independent prognostic factor for patients with gastric cancer especially for those with pathological stage II/III cancer. Our study suggests that therapeutic targeting of PDL1 in gastric cancer might provide an antitumor effect and reduce the metastatic risk for patients with stage II/III gastric cancer.
- Received May 28, 2015.
- Revision received July 6, 2015.
- Accepted July 9, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Gene of the month: T-cell immunoreceptor with immunoglobulin and ITIM domains (TIGIT)
- PD-1 Expression and its Correlation With Prognosis in Clear Cell Renal Cell Carcinoma
- Frequent amplification of HDAC genes and efficacy of HDAC inhibitor chidamide and PD-1 blockade combination in soft tissue sarcoma
- Clinical Significance of Tumor and Immune Cell PD-L1 Expression in Gastric Adenocarcinoma
- The Clinical Significance of PD-L1/PD-1 Expression in Gastroenteropancreatic Neuroendocrine Neoplasia
- Multimodal Anti-tumor Approaches Combined with Immunotherapy to Overcome Tumor Resistance in Esophageal and Gastric Cancer
- The Prognostic Significance of the Tumor-infiltrating Programmed Cell Death-1+ to CD8+ Lymphocyte Ratio in Patients with Colorectal Cancer
- Evaluation of Prognostic Immune Signatures in Patients with Breast, Colorectal and Pancreatic Cancer Receiving Chemotherapy
- Practical Immuno-PET Radiotracer Design Considerations for Human Immune Checkpoint Imaging