


Abstract
Aim: To present a series of seven cases of gastric small cell carcinoma (GSCC) treated surgically and to illustrate the clinicopathological features and clinical course. Patients and Methods: Among 1,832 patients with gastric cancer who underwent gastric resection between 1997 and 2012, we reviewed the clinical records of 7 patients with histopathological diagnoses of GSCC. Results: No patients had preoperative confirmation of GSCC from endoscopic biopsy. Curative resection (R0) was achieved in 5 patients (71.4%). Two out of the 5 patients with curative resection survived more than four years. Two out of 3 patients who received weekly paclitaxel had progression-free survival of more than 10 months. The median survival time for the whole patient group was 14 months and the 3-year survival rate was 25.0%. Conclusion: Curative surgery with adjuvant chemotherapy may be essential to improve the prognosis of GSCC, and weekly paclitaxel chemotherapy may represent a promising chemotherapy for GSCC.
Small cell carcinoma occurs most commonly in the lung, but arises in the gastrointestinal tract on rare occasions (1). In small cell carcinoma of the gastrointestinal tract, the esophagus (53.3%) is the most common site, followed by the colorectum (20.3%) and stomach (11.0%) (2). Primary gastric small cell carcinoma (GSCC) accounts for fewer than 0.1% of all gastric cancer cases, and has aggressive biological behavior and frequent metastasis to lymph nodes and the liver, even in the early stage (3). The prognosis of GSCC is poorer than that of common-type gastric cancer, particularly in the advanced stage, and the median survival time (MST) has been reported as nine months (4). Because GSCC is an extremely rare tumor, no standard treatment strategy has yet been established. The aim of the present study was to present a series of seven cases of GSCC surgically-treated at our Institution and to discuss the clinicopathological features of and treatment strategy for this rare tumor.
Patients and Methods
Among the 1,832 patients with gastric cancer who underwent gastric resection at Osaka City University Hospital (Osaka, Japan) between January 1997 and December 2012, all 7 patients diagnosed histopathologically with GSCC were included in this study. The medical records of these patients were reviewed retrospectively, and the following data were collected for each patient: age; sex; preoperative pathological diagnosis; tumor location; gross type; tumor size; surgical procedure; stage; presence of residual tumor; postoperative adjuvant chemotherapy; metastatic/recurrent site; chemotherapy; and clinical outcome. This retrospective study was conducted in accordance with the principles of the Declaration of Helsinki and informed consent was obtained from all patients prior to treatment.
Distal or total gastrectomy was performed according to tumor size, location, and the status of the resection margin. Clinicopathological characteristics and tumor staging were evaluated based on the third English edition of the Japanese Classification of Gastric Carcinoma (5). Immunohistochemical staining using antibodies such as chromogranin A, synaptophysin, neuron-specific enolase and cluster of differentiation 56 was performed for differential diagnosis. Histopathological diagnosis was confirmed by two experienced pathologists. Chemotherapeutic response was evaluated based on the Response Evaluation Criteria in Solid Tumors (RECIST) guideline version 1.1 (6). Overall survival (OS) was calculated from the date of surgery to the date of last follow-up or death, determined using the Kaplan–Meier method with SPSS software (SPSS, Chicago, IL, USA).
Results
Clinicopathological characteristics of the seven patients with GSCC are shown in Table I. The median age was 74 years (range=59-82 years), and all seven patients were men. It was not possible to confirm GSCC preoperatively by endoscopic biopsy in any patient. Preoperative pathological diagnosis revealed malignant lymphoma in one patient, undifferentiated carcinoma in two, poorly differentiated adenocarcinoma in three and well-differentiated adenocarcinoma in one. The median tumor size was 70 mm (range=35-120 mm). No early gastric cancer was seen, with stage II in three patients, stage III in two and stage IV in two. Although curative resection (R0) was achieved in five patients (71.4%), the other two patients with stage IV disease underwent R2 resection because of peritoneal dissemination and liver metastasis. Tumors in four patients (57.1%) showed adenocarcinomatous components. All five patients who underwent curative resection received adjuvant chemotherapy (two received S-1, two received uracil-tegafur (UFT) and one patient started with S-1, but was changed to UFT after 2 two weeks due to adverse effects of general fatigue). Among these five patients, four developed recurrences. The site of initial recurrence was most commonly the liver (n=3, 75%), followed by lymph nodes, the peritoneum and the site of anastomosis (n=1 each, respectively). The other patient who received S-1 for 1.5 years, who also revealed stage II disease with absence of lymphovascular invasion, remains alive without recurrence as of 48 months after initial surgery (Case 3). As first-line chemotherapy for metastatic/recurrent GSCC, two patients received weekly paclitaxel, one received S-1 plus cisplatin, one received S-1 alone and one received UFT plus irinotecan. In the two patients who received weekly paclitaxel, progression occurred after 10 months (Cases 4 and 7). Case 4 showed first recurrence at the site of anastomosis 20 months after initial surgery, and total gastrectomy was performed. Liver metastases were then found four months after second surgery. Because S-1 could not be continued due to rash that developed one week after administration, weekly paclitaxel (80 mg/m2 on days 1, 8, and 15 of a 28-day cycle) was administered. After one month, liver metastases were significantly reduced, but progression of tumors was identified 11 months after starting weekly paclitaxel (Figure 1). In Case 7, liver metastasis, hepatoportal lymph node metastasis and peritoneal dissemination were found under adjuvant chemotherapy six months after initial surgery. Weekly paclitaxel was administered, and partial response was confirmed 10 months after chemotherapy (Figure 2). However, the patient was found dead at home 12 months after starting chemotherapy, and the cause of death remained unclear.
Characteristics and outcomes for 7 cases of gastric small cell carcinoima.
Five patients died of their primary disease. The median survival time for the whole patient group was 14 months, and the 3-year survival rate was 25.0% (Figure 3).
Discussion
GSCC is an extremely rare and highly malignant tumor, and was first reported by Matsusaka et al. (7) in 1976. A 2011 review of the English literature identified 69 cases of GSCC, the majority of which were from East Asia, particularly from Japan (8).

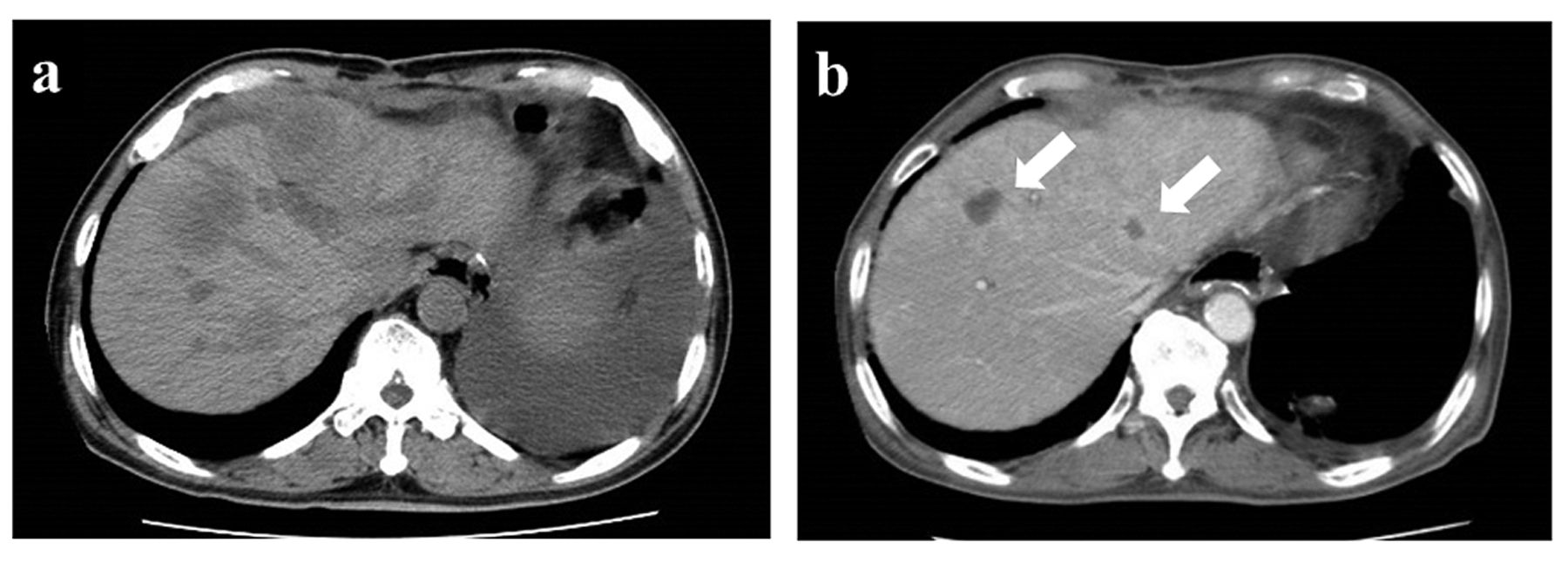
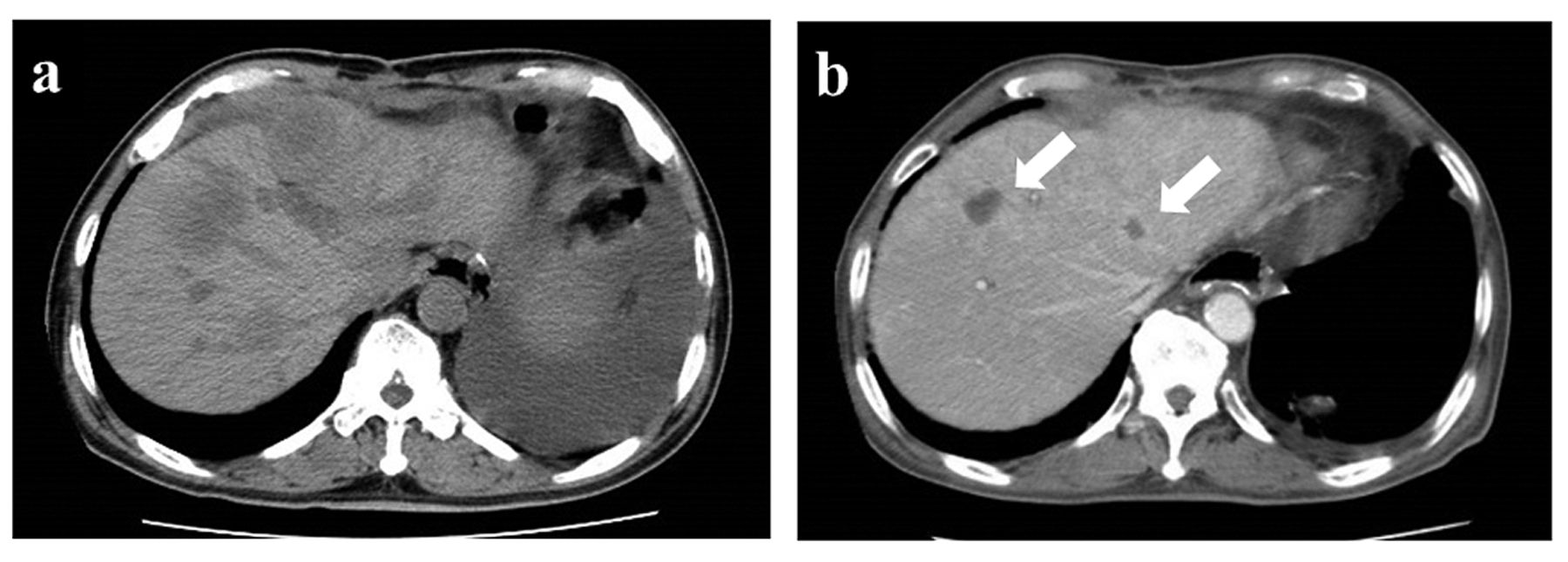
Abdominal computed tomography for Case 4. a: Liver metastasis from gastric small cell carcinoma in S7 (arrow) before starting weekly paclitaxel chemotherapy. b: Eight months after initiating chemotherapy, the tumor shows partial response (arrow).
Abdominal computed tomography for Case 7. a: Multiple liver metastases from gastric small cell carcinoma and ascites before starting weekly paclitaxel chemotherapy. b: Ten months after initiating chemotherapy, liver metastases show partial response (arrow) and ascites have disappeared.
Confirmation of the histopathological diagnosis on preoperative endoscopic biopsy is generally difficult. Tanemura et al. reported that only 18% of patients with GSCC were diagnosed accurately before surgery, whereas 18% of cases were misdiagnosed as malignant lymphoma, 18% as undifferentiated carcinoma and 35% as common-type gastric cancer (9). Similarly, in our series, no patients were preoperatively diagnosed with GSCC from endoscopic biopsy.
GSCC can be classified as pure type or composite type, which comprises mixed histological types including adenocarcinomatous and/or squamous cell components (3). Multi-directional differentiation is observed in 63-71% of GSCCs (10,11), compared to <10% of small cell lung cancers (SCLCs) (12). Similarly, among our cases, four patients (57.1%) showed mixed histological types that included adenocarcinomatous components. The influence of pathological type on prognosis and optimal chemotherapy remains unclear.
GSCC is well-known as being associated with a more frequent incidence of lymphovascular invasion and lymph node metastasis compared to common-type gastric cancer (13). Furthermore, Kubota et al. reported lymphovascular invasion and lymph node metastasis as important factors for survival (14). Consistent with previous reports, out of the five patients in our series who underwent curative resection, all four patients with one of these factors experienced relapse, whereas the only patient who had none of these factors has remained alive without recurrence for 48 months. These findings suggest that intensive postoperative chemotherapy may be needed for patients with GSCC with lymphovascular invasion or lymph node metastasis.
Although no standard treatment strategy has yet been established for GSCC, surgery is generally performed for patients with GSCC without distant metastasis (4). Ishida et al. reported curative surgery as an independent prognostic factor in their retrospective study (15). In the present study, two out of five patients with curative resection survived more than four years. Furthermore, one of these patients underwent curative resection for local recurrence (Case 4). On the other hand, adjuvant chemotherapy has been performed despite a lack of evidence of any survival benefit, due to the high probability of micrometastases and high recurrence rate. Peng et al. reported postoperative chemotherapy as an independent prognostic factor for gastrointestinal small cell carcinoma (16). Huang et al. reported the median survival time for patients with curative surgery using adjuvant chemotherapy as 48.5 months (17). In our case series, the aforementioned two long-term survivors received adjuvant chemotherapy with fluoropyrimidines, and one remains alive without recurrence. Although we cannot draw any definitive conclusions due to the small sample size in this retrospective study, aggressive surgery with adjuvant chemotherapy may be essential in the treatment of cases without distant metastasis. Further study is needed to establish the optimal regimen for adjuvant chemotherapy.

Kaplan–Meier curve of overall survival for the seven patients with gastric small cell carcinoma.
The optimal regimen for metastatic/recurrent GSCC remains unclear due to the paucity of cases. Because the biological and clinicopathological features of GSCC are similar to those of SCLC (7), chemotherapy is often performed using a regimen for SCLC. In the largest retrospective study on chemotherapy for GSCC, Okita et al. reported that irinotecan-plus-cisplatin chemotherapy revealed its efficacy, with a response rate of 75%, a median progression-free survival time of 212 days and a median survival time of 679 days (18). On the other hand, chemotherapy based on that for common-type gastric cancer has also been performed for GSCC in Japan. Some reports have described the efficacy of S-1-based chemotherapy for GSCC (19), whereas no reports describe paclitaxel for GSCC despite this being a common therapy for common-type gastric cancer. For patients with SCLC, weekly paclitaxel chemotherapy has been reported to show efficacy in phase II trials (20, 21). Furthermore, some reports have revealed that weekly paclitaxel is well tolerated for gastric cancer (22, 23). In our case series, chemotherapy was performed according to protocols for common-type gastric cancer, and three patients received weekly paclitaxel as second-line chemotherapy (in Cases 4 and 7, S-1 alone was not tolerated). Two out of the three patients who received weekly paclitaxel chemotherapy achieved partial response for long-term without severe adverse events, although one patient died because of other disease during partial response. Weekly paclitaxel chemotherapy may be a promising chemotherapy for GSCC.
In conclusion, curative surgery with adjuvant chemotherapy may be essential to improve the prognosis of GSCC. Our case series seems to show the efficacy of weekly paclitaxel chemotherapy for GSCC. Examination of a large series is required to determine an optimal treatment strategy for GSCC.
Acknowledgements
The Authors declare no conflicts of interest.
- Received September 23, 2014.
- Revision received October 16, 2014.
- Accepted October 22, 2014.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.