


Abstract
We have established a “second-look operation” protocol that consists of whole biopsy of surgical scar tissue following radio-hyperthermo-chemotherapy (RHC) after unplanned excision of soft tissue sarcoma. Out of 30 patients who underwent RHC for soft tissue sarcoma at our Institution, 6 were enrolled into this study to undergo a second-look operation for unplanned excision. Radiotherapy was given to a total dose of 32 Gy. Hyperthermia was conducted once a week, for a total of five sessions. Chemotherapy was performed at weekly intervals. Surgery was performed to excise the scar tissue that was enhanced on preoperative MRI. In all six cases, no residual tumors were identified in resected scar tissue; thus, no additional wide excision was performed. The average follow-up period was 10.9 years. There were no local recurrences, and all patients were alive at their final follow-up. Long-term follow-up confirmed that RHC can replace additional wide excision for unplanned excision of soft tissue sarcoma.
Optimal treatment strategies exist for most conditions. Such treatments should either be administered by primary care physicians, or primary care physicians should consult with specialists for further evaluation and therapy. In practice, minor treatment delays, misdiagnosis, or mistreatment occur on a regular basis in an effort to treat all patients. If a condition such as a minor infection is initially misdiagnosed at first examination, the patient can still potentially be cured even if antibiotic therapy is delayed, resulting in only minimal disadvantage to the patient. Similarly, if a benign tumor is only partially resected, an additional complete excision would be expected to carry the same risk of complications as those associated with initial complete surgery, resulting in no added harm to the patient. In contrast, partial or marginal excision of soft tissue sarcoma by the initial physician could result in several disadvantages to the patient. Sarcoma should be excised with wide margins of 2 cm or more (1). If tumor cells are identified in the initial surgical field, then an even wider excision must be performed. This can result in the sacrifice of neurovascular bundles, creation of large skin defects with additional skin flaps, or even unexpected amputation. General surgeons tend to excise soft tissue masses without considering these factors.
When unplanned excisions are required and patients are referred to hospitals that specialize in tumor resection, the goal is to reduce the surgical margins so as not to sacrifice adjacent structures. Although chemotherapy is widely used to treat soft tissue sarcoma, its efficacy remains controversial (2-4). To enhance the efficacy of adjuvant therapy, additional options are required, particularly for unplanned excision cases. We have developed a radio-hyperthermo-chemotherapy (RHC) regimen that is administered before surgery for high-grade soft tissue sarcomas of the limbs, and have reported excellent clinical results (5, 6). In the present study, we performed RHC prior to unplanned excision in soft tissue sarcoma cases and examined the surgical scar tissue to determine whether any tumor cells remained (second-look operation) following RHC. Second-look surgery is commonly performed in patients with ovarian cancer, and colorectal cancer to determine whether any cancer cells remain following tumor resection (7-12). We modified and introduced this procedure following RHC for the first time in the field of musculoskeletal oncology (5). The short-term outcomes were excellent in that no tumor cells remained after RHC, so no further wide excision was required. However, the validity of this procedure was estimated only by histology, so the possibility of local recurrence was a continuous concern. In the present study, we report the long-term results of second-look operation following RHC for unplanned excision of soft tissue sarcoma and its superiority to conventional additional wide excision.
Patients and Methods
A total of 30 patients underwent RHC for soft tissue sarcoma at our Institution between 1995 and 2004. Out of these, 6 patients (three men, three women) were entered into this study to undergo a second-look operation. All cases were referred to our Department after simple marginal resection performed by a previous physician and histological diagnosis was obtained. Patients with low-grade sarcomas (such as dermatofibrosarcoma protruberans and well-differentiated liposarcoma), or tumors in the pelvic and dorsal regions were excluded from this study. Other exclusion criteria included age <15 or ≥70 years, performance status of >2, white blood cell count <3000/μl, neutrophil count <1500/μl, platelet count <75000/μl, hemoglobin <7g/μl, creatinine clearance <60 ml/min, aspartate aminotransferase/alanine aminotransferase >75 IU/l (male) or 67.5 IU/l (female), total bilirubin >3.0 mg/dl, left ventricular ejection fraction <50%, no documented consent obtained, and allergies to any of the drugs used in the study.
Sarcomas were located in the forearm (n=4), foot (n=1), and thigh (n=1). Diagnoses included malignant fibrous histiocytoma (n=3), myxoid liposarcoma (n=1), sclerosing epithelioid fibrosarcoma (n=1), and synovial sarcoma (n=1). The mean patient age was 54 years (range=39 to 66 years).
Prior to RHC, angiography was performed, after which an arterial catheter was inserted and a reservoir was implanted. If the tumor was in a lower extremity, the catheter was inserted via the femoral artery on the affected side and the contralateral side, and the reservoir was implanted in the inguinal region or in the lower abdomen. If an upper extremity was affected, the catheter was inserted into the brachial artery and the reservoir was implanted in the precordial region. Chemotherapy was given by intra-arterial infusion using the reservoir, and consisted of cisplatin (100 mg/m2) in conjunction with the first, third, and fifth hyperthermia sessions, and pinorubin (an adriamycin derivative; 30 mg/m2) in conjunction with the second and fourth hyperthermia sessions (5). Two weeks after five sessions of RHC had been completed, patients underwent systemic chemotherapy (primarily ifosfamide), followed by surgery. Chemotherapeutic agents were administered continuously via the reservoir from the start of hyperthermia until approximately 1.5 h after hyperthermia was completed.
Radiotherapy involved the delivery of radiation at a dose of 2 Gy, five days per week, over 16 sessions, for a total dose of 32 Gy. Irradiation was performed immediately before hyperthermia and chemotherapy.
Hyperthermia was conducted using an 8-MHz radiofrequency capacitive heating system (Thermotron RF-8; Yamamoto Vinyter, Osaka, Japan). The temperature was measured by insertion of a hyperthermia needle into the scar tissue and insertion of a thermocouple thermometer (0.64-mm) into the space. The objective of treatment was to achieve a temperature of 42.5°C or more for 60 min. The treatment protocol involved five sessions, consisting of four sessions of RHC followed by one session of hyperthermia and chemotherapy.
Surgery was performed to excise scar tissue that was enhanced on preoperative magnetic resonance imaging (MRI). Resected specimens were examined postoperatively under a microscope on the largest cut section. If any residual cancer cells were present in the specimen, wide excision was planned. All of the patients were informed about the nature of the treatment and their consent was obtained. Adverse events were graded according to the Common Terminology Criteria for Adverse Events (CTCAE) v3.0 issued by National Cancer Institute (http://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/ctcaev3.pdf). Functional outcomes were assessed by Enneking et al.'s functional scoring system (13).
This study protocol was approved as 45-07-0022 by the Institutional Review Board (IRB) of the Nagoya City University Hospital, Nagoya, Japan. This study complied with ethical standards outlined in the Declaration of Helsinki. Written informed consent was obtained from all patients before entry of the patients into this study.
The Authors confirm that all ongoing and related trials for this drug/intervention are registered. Cases in this study were not registered when the treatment started because there were no IRB system in our hospital. IRB first approved on February 14, 2008. The patients were registered between July 27 and 1995 to March 11, 2004, and followed-up until March 1, 2014.
Results
In all six cases, no residual cancer cells were identified in the resected scar tissue, hence no additional wide excisions were performed. Patient and tumor characteristics, and therapy are shown in Table I. No major complications were observed during preoperative RHC, except for mild pain and minor burns. Burns were caused by hyperthermia in three patients. Dehiscence of the skin wound and delayed healing occurred in three patients. Details of adverse effects associated with RHC are listed in Table II. Preserved adjacent structures included the median nerve, radial nerve, and femoral artery, vessel, and nerve, and postoperative function was 100% by Enneking et al.'s score for all patients. The average follow-up period was 10.9 years (range=8.1 to 17.6 years). There were no local recurrences and all patients were alive at final follow-up. Figures 1 and 2 are representative cases of RHC after unplanned excision of sarcoma. Adjacent structure such as median nerve in figure 1 is successfully preserved without postoperative recurrence.
Unplanned excision cases generally experience a higher frequency of local recurrence and shorter survival (14-16). Thus, RHC and second-look operation produced excellent clinical results in this patient population.
Discussion
Soft tissue masses in the extremities are quite common, and most of them are benign conditions, such as ganglia, epidermal cysts, lipomas, and hemangioms. These tumors are located in fat, muscle, or subcutaneous tissue and appear to be relatively easy to excise. When patients with these masses consult oncologists, MRI and biopsy are generally performed prior to excision of suspected malignancies. However, most patients consult general physicians, some of whom resect the tumors without pretreatment examination or planning. Optimal treatment strategies exist for all soft tissue tumors, even those that are benign. When the histological diagnosis reveals malignancy, initial therapy directly influences the clinical course of the patient and often worsens it.
Patient and tumor characteristics, and therapy. All patients were continuously disease-free at follow-up.
Ideal surgical margins for cure of extremity sarcomas were defined by Enneking in 1980 (1). The concept of a wide surgical margin has become more sophisticated with several modifications, such as the barrier concept, and narrow margins can be used with an adequate statistical analysis of recurrence (17). Following unplanned excision, additional wide excision is necessary in most cases. In such procedures, neurovascular structures may be resected if the initial surgery contaminated them with cancer cells. Skin and muscle defects also tend to be larger following unplanned excisions compared to when initial wide excision is carried out properly. When patients who must undergo unplanned excision of soft tissue sarcoma consult us, our goal is to minimize the surgical margin to at least the same size as the initial wide margin.
Although chemotherapy is an option for eradication of remaining tumor cells, the efficacy rate for local chemotherapy for soft tissue sarcoma is only 20% to 40% (2-4).
We have established hyperthermia combined with chemotherapy and radiotherapy to augment the therapeutic efficacy of second-look surgery (5, 6). We previously reported improved local tumor control and 5-year survival rates in patients with high-grade soft-tissue sarcomas who received RHC (5). Basic research supports the rationale for the use of hyperthermia. Cancer cells are damaged at 42°C, while surrounding normal cells are not. This suggests that 42.5°C is the optimal temperature for therapeutic killing of cancer cells while minimizing damage to surrounding skin, blood vessels, and nerves (18, 19). Following effective RHC, we performed resection of scar tissue to determine whether any viable tumor cells remained. Informed consent was obtained from all of the patients regarding the performance of wide excision if any viable cells remained. However, no viable cells were detected in the resected tissue of any patients, so no further additional wide excisions needed to be performed. This procedure is called a second-look operation. In this study, long-term follow-up demonstrated that this procedure is effective, because no local recurrences were observed after any second-look operation.
Adverse effects associated with radio-hyperthermo-chemotherapy.
Qureshi et al. reported that among 134 patients who underwent unplanned excision of soft tissue sarcoma, residual tumors were identified in 48% of patients after surgical re-excision (14). Furthermore, local recurrence rates were considerably higher in the unplanned excision group compared to the control group (23.8% vs. 11%), and survival rates were also significantly lower in the unplanned excision group. Additional studies have reported that unplanned excision of soft tissue sarcoma compromises of long-term local control (15, 16). The present results suggest that more comprehensive oncological management consisting of chemotherapy, radiotherapy, and hyperthermia can be used to minimize the disadvantages associated with unplanned excision.

Case 1. A 57-year-old female presented with a soft tissue mass in the palmar forearm and median nerve pain. Several steroid injections were administered, and marginal excision was performed by a previous physician. The histological diagnosis was malignant fibrous histiocytoma. Gadolinium enhancement on Magnetic resonance imaging (MRI) showed tumor cell contamination surrounding the flexor tendons and median nerve, indicating that the tendons and nerve would be sacrificed in an additional wide excision. After radio-hyperthermo-chemotherapy (RHC), only scar tissue was excised in a piecemeal fashion for biopsy. No tumor cells were found on histology, resulting in no further wide excision. No local recurrence has occurred, and the patient is disease-free 17 years postoperatively. The function of the affected limb is excellent. A: T1-weighted MRI after unplanned excision. B: T2-weighted MRI. C: Gadolinium-enhanced MRI. D: Hematoxylin and eosin (H-E) stain of excised tumor margin. E: Preserved tendons and median nerve.
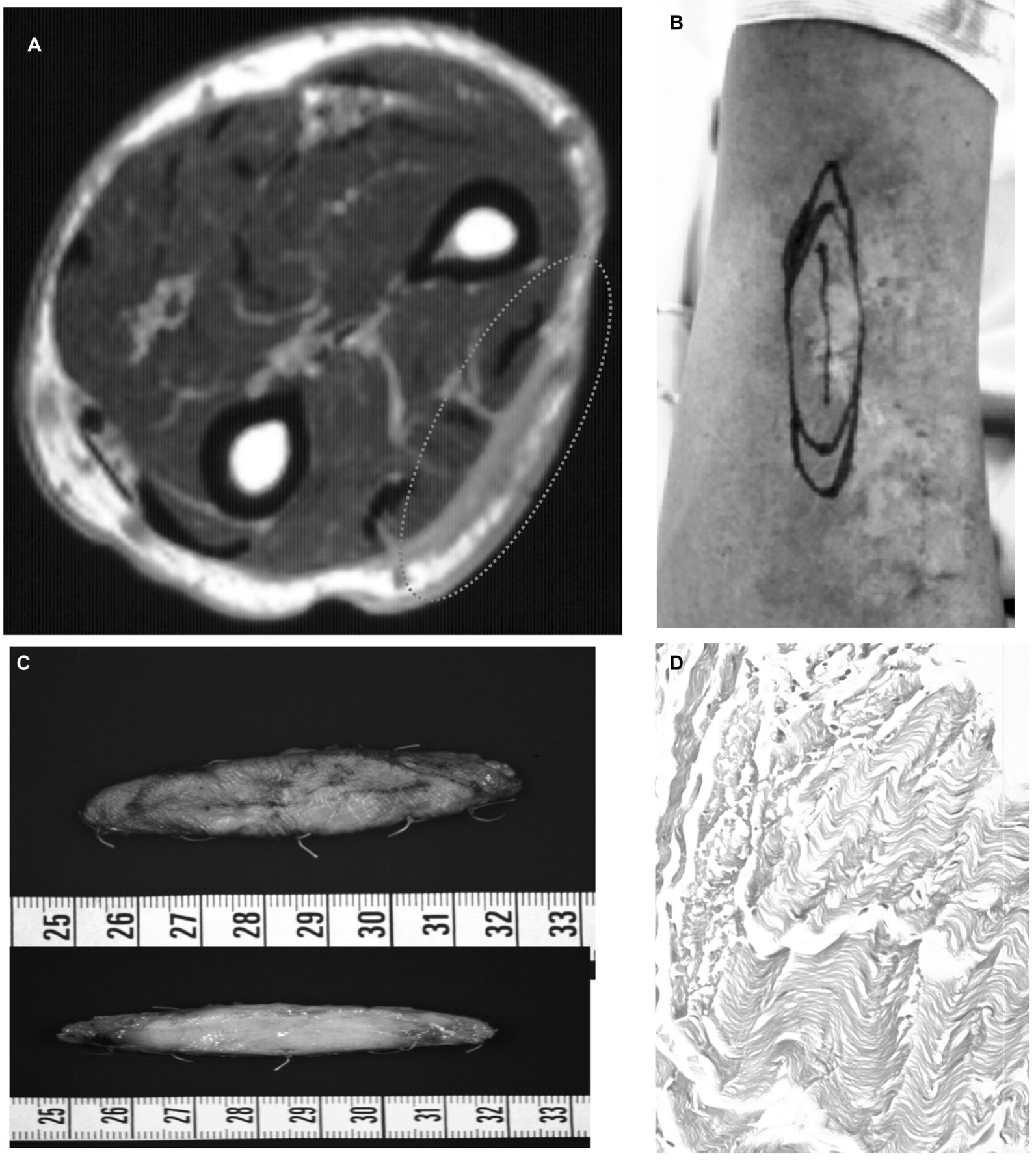
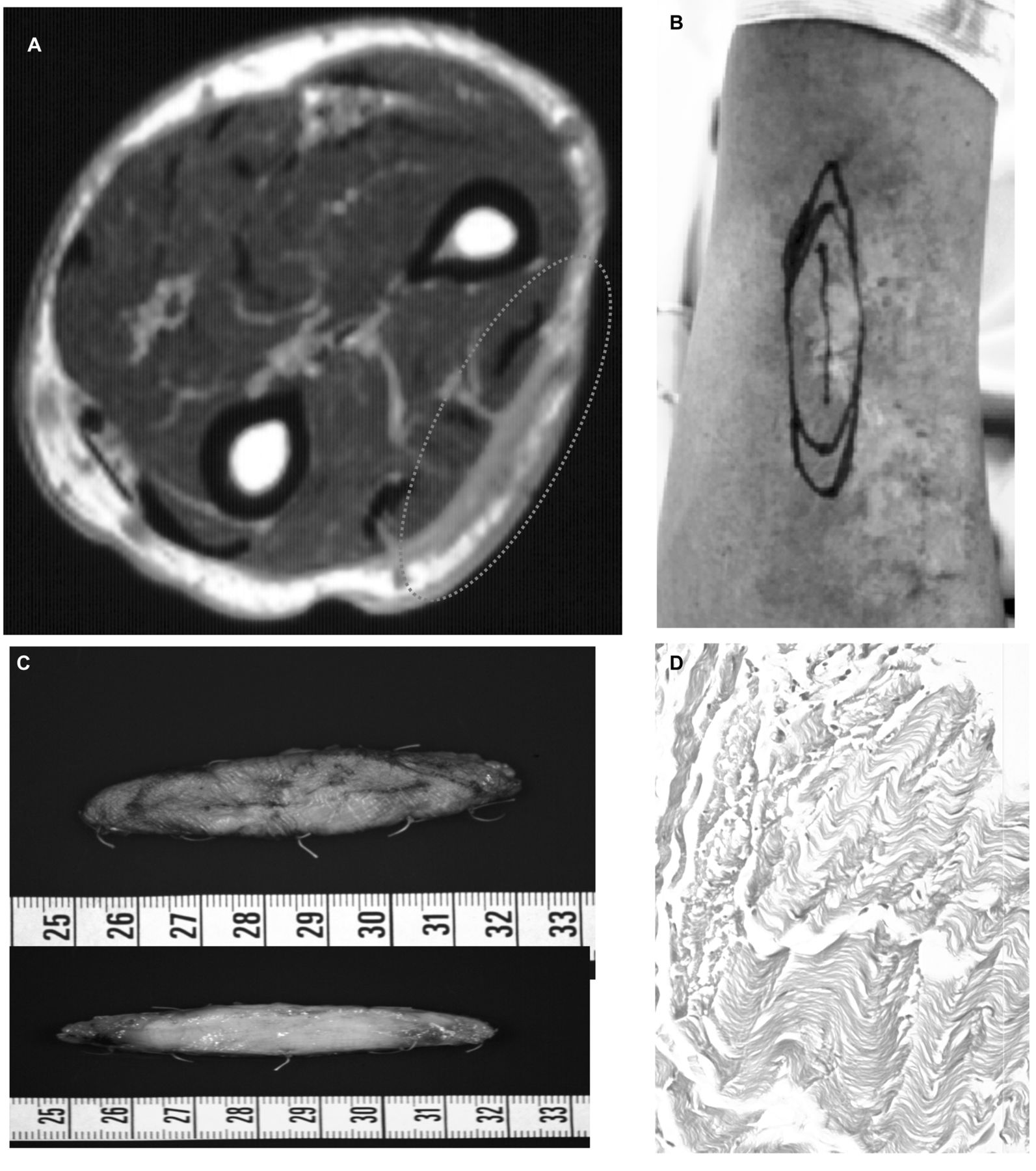
Case 5. A 66-year-old man presented with a soft tissue mass in the forearm. Marginal excision and histological examination revealed malignant fibrous histiocytoma. RHC and a second-look operation were performed. No residual tumor was found in excised scar tissue. The function is excellent and the patient is disease-free 8 years postoperatively. A: Gadolinium-enhanced MRI after unplanned excision. B: Surgical plan after RHC to excise the scar tissue that was enhanced on preoperative MRI. C: Excised scar tissue for second-look operation. D: H-E stain revealed no residual tumor cells.
Second-look surgery is defined as a surgical procedure used to determine whether a patient is free of disease after initial treatment. If disease is found, additional surgery will be performed at the time of or after second-look surgery. Second-look surgery is performed for some patients with ovarian cancer or colorectal cancer (7, 8, 10, 11). Following resection of cancer and administration of chemotherapy, second-look procedures are performed to determine whether any cancer cells remain. However, even when no colorectal cancer cells are observed in second-look surgery specimens, the relapse rate is 12% to 19% (9).
The indications for a second intervention in patients with cancer remain under debate. Some surgeons use postoperative carcinoembryonic antigen levels to determine which patients with colorectal cancer should undergo second-look surgery (9). The second-look operation procedure presented herein slightly differs from the procedures used in ovarian cancer and colorectal cancer, since it is not actively performed in patients with primary tumors. Rather, it is used as a remedial measure for patients who have undergone inadequate resection at another hospital. However, we have defined this treatment as a second-look operation for bone and soft tissue tumors as a comprehensive biopsy procedure to check the previous surgical field. Our current results indicating an absence of viable cancer cells and a lack of recurrences during long-term follow-up, support this concept. Avoiding additional wide excision preserves blood vessels, nerves, and muscles, resulting in preservation of limb function. Due to recent attempts to educate general practitioners about avoiding unplanned excision of soft tissue sarcoma, the incidence of unplanned excisions has decreased (16). However, some patients with sarcoma still undergo unplanned excisions. RHC and second-look operation should provide such patients with the opportunity to avoid such procedures.
- Received August 19, 2014.
- Revision received September 16, 2014.
- Accepted September 23, 2014.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}