


Abstract
Aim: To develop an instrument for estimating survival after irradiation for metastatic epidural spinal cord compression (MESCC) from head and neck cancer. Patients and Methods: In 58 patients, eleven factors were evaluated for influence on survival: age, gender, performance status, tumor site, time from cancer diagnosis until MESCC, affected vertebrae, walking ability, further osseous lesions, organ metastases, time developing motor deficits and radiation regimen. Factors with significant association with survival or a trend (multivariate analysis) were used for scoring. Results: Walking ability, visceral metastases and time to developing motor deficits were included in the score. Scoring points were calculated by dividing 6-month survival rates by 10. Patients' scores were obtained from adding the points of the three factors. Four groups were created, 7-10, 12-15, 16-18 and 21 points. Six-month survival rates were 0%, 27%, 71% and 100% (p<0.001). Conclusion: With this new instrument, one can estimate 6-month survival probabilities of patients with MESCC from head-and-neck cancer.
- Head-and-neck cancer
- metastatic epidural spinal cord compression
- irradiation
- survival
- predictive instrument
For patients with cancer of the head and neck new surgical approaches and new radiotherapy techniques are available for treating the primary tumor and locoregional lymph nodes, as well as for treating of locoregional recurrences. Therefore, patients treated today with locoregional disease live considerably longer than those treated in the past. Better local control translates to increased risk of developing distant metastases including vertebral metastases. Vertebral metastases associated with metastatic epidural spinal cord compression (MESCC) are not very common in head and neck cancer patients. In our own database of more than two thousand patients with MESCC, only 58 patients had a primary tumor that was located in the head-and-neck region (1). Therefore, the optimal treatment for such patients is quite unclear, in particular, because palliative approaches, such as MESCC, are very uncommen situations (2).The decision for a certain treatment approach, including options such as surgery, short-course irradiation, longer-course irradiation or stereotactic body radiotherapy should be based on the patient's expected survival time. The shorter the survival time, the less time consuming and less burdensome the treatment regimen should be for the patient (3-8). Therefore, predictive tools that allow estimation of a patient's survival time, as precisely as possible, are important to patient care. Since head and neck cancers show a different biology than other primary tumors with respect to recurrence and metastatic patterns, this group of patients requires a separate tool. In the present study, we created a predictive tool for estimating the survival, particularly of patients with MESCC, from head and neck cancer.
Patients and Methods
Fifty-eight patients treated with irradiation-alone for MESCC for head and neck cancer were included in this retrospective analysis. Criteria for inclusion were motor deficits of the legs due to MESCC, confirmation of MESCC with computed tomography scans or magnetic resonance imaging and no previous local treatment of the involved segments of the spine. Patients were presented to a surgeon before irradiation. The data were collected from patients, patient files and treating physicians. Patients' characteristics are presented in Table I. Irradiation was performed with a linear accelerator and the target volume included one unaffected vertebra above and below the vertebra involved by metastases.
A total of eleven factors were evaluated for survival. These factors were age (<60 years versus ≥60 years), gender, Eastern Cooperative Oncology Group performance score (ECOG-PS 1-2 versus ECOG-PS 3-4), tumor site (nasopharynx versus oropharynx versus hypopharynx versus larynx versus salivary glands versus oral cavity/floor of the mouth), time from initial diagnosis of head-an-neck cancer until MESCC (≤15 months versus >15 months), number of affected vertebrae (1-3 versus ≥4), ambulatory status prior to irradiation (no versus yes), further osseous lesions (no versus yes), organ metastases (no versus yes), time developing motor deficits prior to irradiation (1-7 days versus >7 days) and the radiotherapy regimen (5×4 Gy in 1 week versus longer-course irradiation programs, such as10×3 Gy in 2 weeks, 15×2.5 Gy in 3 weeks or 20×2 Gy in 4 weeks).
Patients' characteristics.
For the univariate analysis of survival, the Kaplan-Meier method and the log-rank test were used. Those factors that achieved significance in the univariate analysis (p<0.05) or showed a strong trend (p<0.07) were additionally evaluated in a multivariate manner (Cox regression analysis). The factors that remained significant in the multivariate analysis or showed at least a trend were included in the instrument designed for estimating the probability of surviving six months or longer following irradiation. In accordance with our preceding study (9), scoring points were calculated by dividing the survival rate at six months by 10. The prognostic score for the individual patient was calculated by adding the scoring points of the significant characteristics.
Univariate analysis of survival.
Results
On univariate analysis, four factors had a significant impact on survival: ECOG-PS (p<0.001), ambulatory status prior to irradiation (p<0.001), visceral metastases (p<0.001) and time to developing motor deficits prior to irradiation (p=0.002). The time from initial diagnosis of head and neck cancer until MESCC showed a trend (p=0.069). The data of the univariate analysis are given in Table II. On multivariate analysis, ambulatory status (risk ratio (RR): 4.31; 95%-confidence interval (CI): 1.85-10.20; p<0.001) and visceral metastases (RR: 7.20; 95%-CI: 3.17-17.58; p<0.001) were significant. Time developing motor deficits showed a trend (RR: 1.90; 95%-CI: 0.91-4.03; p=0.087). ECOG-PS (RR: 1.60; 95%-CI: 0.61-4.17; p=0.34) and time from initial diagnosis of head and neck cancer until MESCC (RR: 1.31; 95%-CI: 0.90-1.89; p=0.16) did not achieve significance in the multivariate analysis.
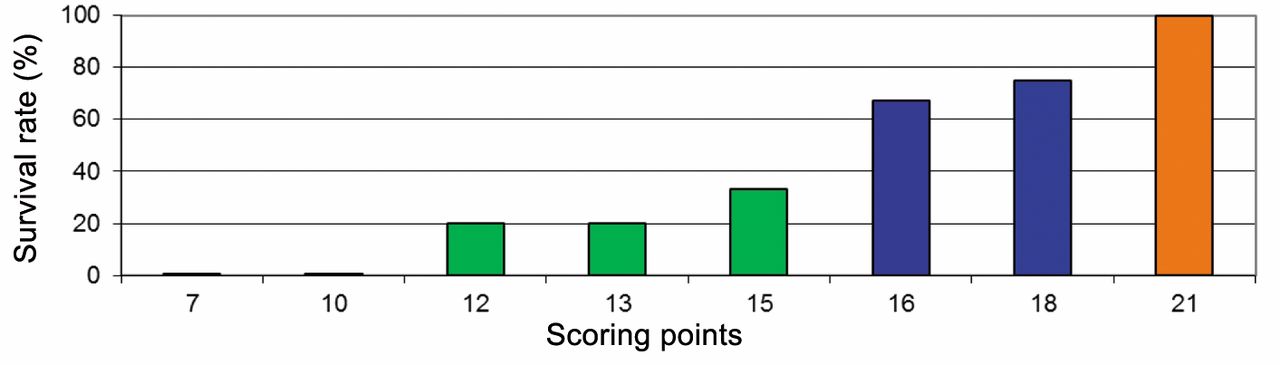
The 6-month survival rates of the different scoring points (7, 10, 12, 13, 15, 16, 18 or 21 points).
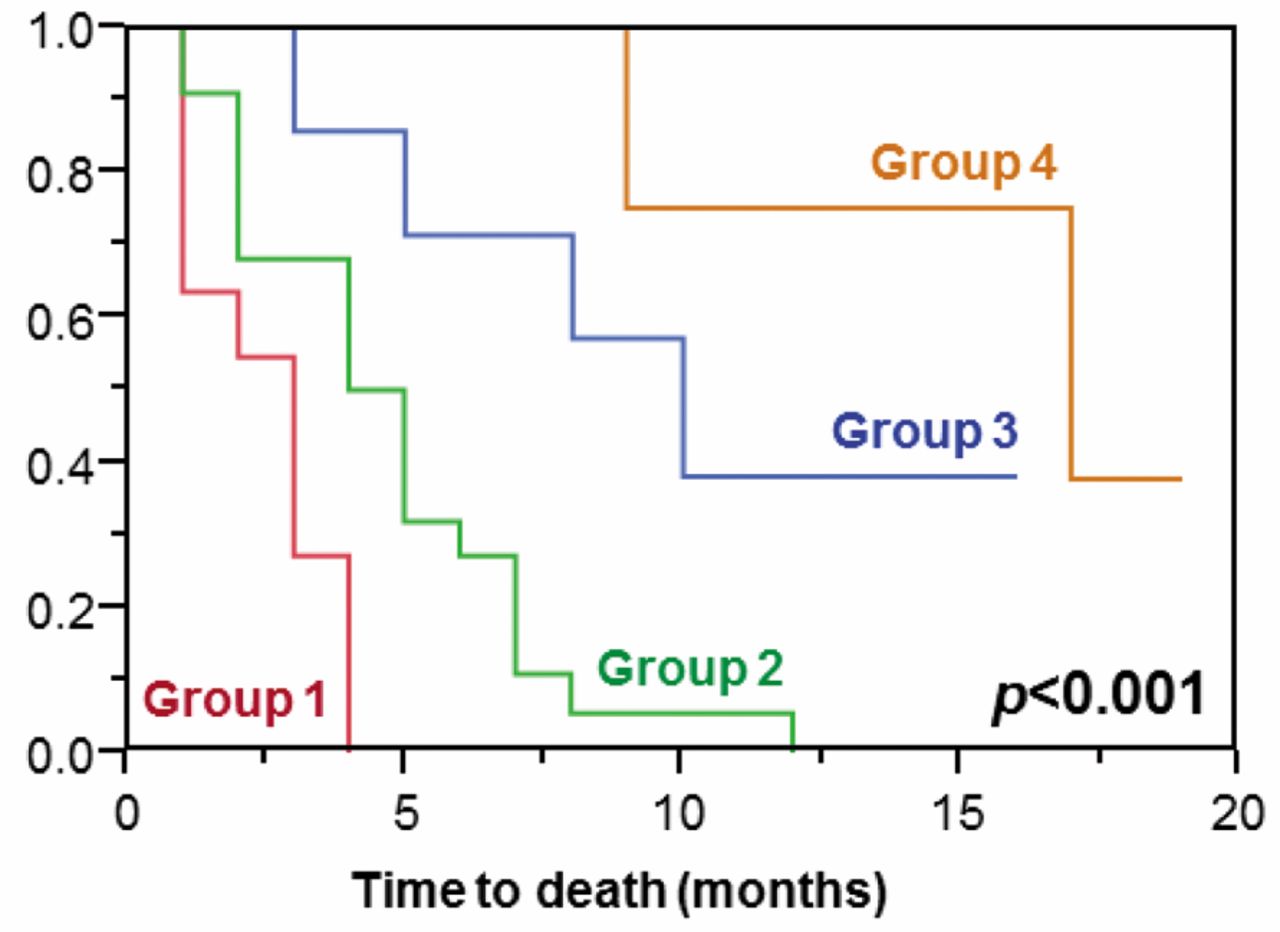
Kaplan-Meier curves of the four prognostic groups 1 to 4. The p-values were calculated with the log-rank test.
Ambulatory status prior to irradiation, visceral metastases and time to developing motor deficits prior to irradiation were included in the scoring instrument. Scoring points for each of the three factors were calculated by dividing the 6-month survival rate (in %) by 10. The prognostic score for each patient was obtained from adding the scoring points of the three factors. The additions resulted in the following scores: 7, 10, 12, 13, 15, 16, 18 or 21 points. The scores and the corresponding 6-month survival rates are presented in Figure 1. Considering the 6-month survival rates related to the scores, it appeared reasonable to design four survival groups: 7-10 points (group 1, n=11), 12-15 points (group 2, n=22), 16-18 points (group 3, n=7) and 21 points (group 4, n=18). The 6-month survival rates of these four groups were 0%, 27%, 71% and 100%, respectively (p<0.001; Figure 2). Median survival times were 3 months, 4.5 months, 10 months and 17 months, respectively.
Discussion
Spinal tumors and particularly MESCC have gained importance in oncologic research (10-12). A patient's expected survival time is one of the most important characteristics that should be considered when developing a treatment strategy for an individual patient presenting with MESCC (2). Therefore, an instrument that contributes to the prediction of the remaining life time, as precisely as possible, would be of great value. Although survival scores have already been presented for patients with MESCC, the available scores do not adequately consider the specific biology and metastatic patterns of head-and-neck cancers (9, 13). Therefore, a tool for predicting the survival prognosis, particularly for this group of patients, was created in the present study. This tool was based on three prognostic factors: pre-irradiation ambulatory status (no or yes), presence or absence of visceral metastases and the dynamic of developing motor deficits prior to irradiation (fast: 1-7 days versus slower: >7 days). The impact of the time of developing motor deficits on survival can be explained by the fact that a faster development corresponds to a more aggressive tumor (14, 15). Based on these three factors, four survival groups were designed with significantly different 6-month survival rates between 0% and 100%. No patient of group 1 survived longer than four months. Therefore, these patients should receive a short course of irradiation, such as 5×4 Gy in one week, and are generally not candidates for additional decompressive surgery (3, 4). In group 2, only 27% of patients survived at least six months. Therefore, these patients should generally be treated with irradiation alone, preferably with 5×4 Gy. Decompressive surgery may be added to highly selected patients of this prognostic group, for example in the case of sphincter dysfunction, vertebral fracture or spinal instability (2, 16). In group 3 of the present study, the majority of patients survived at least six months. These patients may be considered for decompressive surgery followed by longer-course irradiation, such as 10×3 Gy in two weeks (3). Longer-course programs result in better local control of MESCC than 5×4 Gy (7, 8). Patients of the prognostic group 3 likely live long enough to be at risk of experiencing a recurrence of MESCC in the irradiated parts of the spine. In group 4, all patients survived at least six months and their median survival time was quite long (17 months). Also, these patients should be presented to a neurosurgeon to discuss if decompressive surgery is indicated. Since a retrospective study suggested that patients with MESCC and a very favorable survival prognosis would benefit from doses greater than 10×3 Gy in terms of better local control of MESCC and better survival, patients of this prognostic group should receive irradiation with 15×2.5 Gy in three weeks or 20×2 Gy in four weeks (17). If the recommendations regarding the tolerance doses for the spinal cord and the vertebral bone are followed, also stereotactic body radiotherapy may be considered for selected patients of prognostic group 4 (18). When using this new predictive tool, one should be aware that it was designed from retrospective data, which may contain hidden biases. However, since MESCC from head-and-neck cancer is still relatively rare, a tool created from prospective data will not be available in the near future for this patient group.
In conclusion, this new predictive instrument enables the treating physician to estimate the 6-month survival probability of patients with MESCC from head and neck cancer. This knowledge will have a significant impact on the decision for a personalized treatment approach, in particular regarding the administration of decompressive surgery or stereotactic body radiotherapy, as well as regarding the selection of the most appropriate schedule of irradiation. Validation of this system will require the analysis of another dataset generated from similar patients.
Footnotes
-
Conflicts of Interest
On behalf of all Authors, the corresponding Author states that there is no conflict of interest related to this study.
- Received September 6, 2014.
- Revision received September 29, 2014.
- Accepted October 7, 2014.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A New Survival Score for Patients Scheduled for Palliative Irradiation of Locally Advanced Carcinoma of the Head-and-Neck
- The emergence of solid stress as a potent biomechanical marker of tumour progression
- A Scoring Instrument to Predict the Survival Prognoses of Patients with Metastatic Epidural Spinal Cord Compression from Gynecological Malignancies
- Prognosis of Patients with Metastatic Spinal Cord Compression from Adrenocortical Carcinoma
- A Total Radiation Dose of 70 Gy Is Required After Macroscopically Incomplete Resection of Squamous Cell Carcinoma of the Head and Neck
- Prognostic Factors After Definitive Radio(Chemo)Therapy of Locally Advanced Head and Neck Cancer
- Importance of Chemotherapy and Radiation Dose After Microscopically Incomplete Resection of Stage III/IV Head and Neck Cancer