


Abstract
Background/Aim: Neurofibromas, benign tumors of the nerve sheaths, are the hallmark of neurofibromatosis type 1 (NF1), an autosomal-dominant inherited tumor predisposition syndrome. Malignant tumors arising from nerve sheath cells are an important factor influencing the life expectancy of NF1 patients. Expression of growth factors and growth factor receptors play a key role in the development of tumors. Therapy of peripheral nerve sheath (PNS) tumors is predominantly surgical. The outcome in malignant entities of NF1-affected patients remains poor, despite many efforts to implement pharmacological therapy into the treatment modalities. Growth of peripheral nerve sheath tumors is finely-adjusted by growth factors and PNS tumors express growth factor receptors. However, quantification of receptor expression and comparison to the expression of other related factors are not available. The aim of the present study was to determine growth factor expression relevant for growth control in neurofibromas of NF1. Materials and Methods: Fifty-eight dermal, dermal/diffuse and plexiform neurofibromas and malignant peripheral nerve sheath tumors (MPNST) of NF1-affected patients were analyzed immunohistochemically for the expression of growth factors relevant for angiogenesis: vascular endothelial growth factor (VEGF), basic fibroblast growth factor (bFGF) and epithelial growth factor receptor (EGFR). The vessel density was also determined quantitatively by light microscopy. Results: Plexiform neurofibroma revealed a higher expression level for VEGF compared to dermal/diffuse neurofibroma. However, statistical significant differences for VEGF expression and of all other proteins investigated were found in comparison to MPNST only. EGFR expression was remarkably high in NF1 patients in their first decade of life. However, this result has to be interpreted with caution in view of the high number of young patients with MPNST in this age group. Vessel density correlated with tumor type. Vessel density increased significantly comparing benign nerve sheath tumors and MPNST (p<0.05). Discussion/Conclusion: This study revealed the presence of factors and receptors involved in angiogenesis as a prerequisite for tumor development and maintenance of PNS in NF1. These factors are highly expressed in all tumors of this study. This study reveals these relevant factors in nerve sheath tumors and also described the significant increase of vessel density in MPNST compared to benign counterparts. Anti-angiogenic drugs are presently investigated for application in NF1 tumor treatment, in particular for patients with a surgically-intractable high tumor burden. Drugs capable of blocking the EGFR receptor-mediated pathway are promising tools within the pharmacological repertoires to treat these patients.
- Epidermal growth factor receptor
- vascular endothelial growth factor
- basic fibroblastic growth factor
- neurofibromatosis type 1
- vessel density
- malignant peripheral nerve sheath tumor
Neurofibromatosis type 1 (NF1) is an autosomal dominant inherited tumor predisposition syndrome affecting about 1 in 2,500 children living at birth (1). The most prominent finding in the highly variable phenotype is benign peripheral nerve sheath (PNS) tumors, predominantly affecting the integument (2). There are 2 predominant variants of neurofibroma, the dermal and plexiform type; the latter can dedifferentiate into a malignant peripheral nerve sheath tumor (MPNST) (3). Development of MPNST is an important factor for the reduced life expectancy of NF1-affected patients (4). Neurofibromas are highly vascularized solid tumors (5). Growth factors are recognized important regulators of angiogenesis in tumors (6, 7). Inhibitors of neo-angiogenesis are under study to treat neurofibromas in NF1 patients (5). However, the presence and distribution of growth factors involved in angiogenesis in NF1-associated PNS are currently not well-recognized (8, 9). This study attempts to prove the hypothesis that in NF1-associated tumors the malignant variants will show a higher vessel density than the benign counterparts and that growth factors should be more intensely expressed in the malignant phenotype.
Materials and Methods
This study comprised of 58 formalin-fixed and paraffin-embedded PNS tumors of 29 female and 29 male patients with NF1 (Table I). All patients fulfilled diagnostic criteria of the entity according to current recommendations (10). Age of patients was 3 to 70 years, mean age of females 27.5 years and of males 29.2 years. All tumors were excised during surgical procedures in the Department of Oral and Craniomaxillofacial Surgery. All patients gave their informed consent for the investigation.
Diagnosis was established on routinely performed on 4-μm-thin slices stained with haematoxylin-eosin, van Gieson and periodic acid Schiff reaction. Furthermore, all tissues were investigated for proliferative activity by means of immunohistochemical staining for Ki67. Schwann cell origin of tumors was confirmed by S-100 protein detection in tumor cells.
The tumors were classified in 4 categories: 1=dermal (N=18), 2=dermal/diffuse (N=9), 3=plexiform (N=22), 4=MPNST (N=9). A further classification was based on gross anatomy: group 1 (extremities; N=23), group 2 (trunk; N=9) and group 3 (head and neck; N=25).
The following reagents were used for immunohistochemistry: Factor VIII-associated antigen antibody (DakoCytomation, Glostrup, Denmark; No. A0082; dilution 1:1000); Goat Serum (DAKO No. X0907, DakoCytomation), mouse monoclonal anti-human epidermal growth factor receptor antibody (Clone: H11, Code M3563; dilution 1:200, DakoCytomation); mouse monoclonal vascular endothelial growth factor antibody (C-1) (Sc7269; dilution 1:200, Santa Cruz Biotechnology, Santa Cruz, CA, USA); rabbit polyclonal basic fibroblast growth factor-2 antibody (147) (Sc79; dilution 1:50, Santa Cruz Biotechnology), Strept ABComplex/HRP Duet (mouse, rabbit), (DAKO K0492, DakoCytomation).
Expression levels were graded semi-quantitatively into 4 grades: 0=no staining, 1=poor, 2=medium and 3=strong. Further details of immunohistochemical procedures are detailed elsewhere (8, 9, 11).
The count of vessels and calculations of vessel density were performed by means of a binocular microscope (Olympus BH-2, Olympus Europe, Hamburg, Germany) analyzing an area of 1 mm2 per sample.
The statistical analysis was performed using the SPSS© software (SPSS Inc., SPSS for Windows© 15.0, Chicago, IL, USA). A non-parametric correlation analysis following Kendell-Tau b was applied for analyzing the items VEGF, bFGF, EGFR, patient age, decade of life, tumor type and tumor localization. Differences with a probability error lower than 5% (p<0.05) were regarded significant. Furthermore, the Mann-Whitney-U-test was applied to analyze the tumor type and VEGF data.
Results
VEGF. Immunoreactivity for VEGF was missing in 6 (33.3%), poor in 8 (44.4%), medium in 3 (16.6%) and strong in 1 (0.6%) case(s) of dermal neurofibroma (total: 18 cases/100%). In diffuse neurofibroma no staining was diagnosed in 4 cases (44.4%) and was poor in 5 (66.6%). On the other hand, plexiform neurofibroma showed no staining for VEGF in 3 cases (14.3%), poor staining in 19 (47.5%), medium in 7 (33.3%) and there was 1 case (0.5%) with strong staining pattern (total: 21 cases/100%). MPNST showed the following staining pattern: no staining in 2 tumors (22.2%), poor staining in 3 (33.3%) and medium staining in 4 (44.4%), (Figures 1 and 2, Tables I and II).
VEGF expression was significantly higher in PNF and MPNST compared to dermal and diffuse neurofibroma (r=0.300, p=0.009, N=58). The Mann Whitney-U-test confirmed this differential expression pattern for the comparison of dermal/diffuse and plexiform neurofibroma (Figure 3).
bFGF. Two dermal tumors showed no staining for bFGF (12%), in further 12 cases the staining intensity was poor (66.7%) and medium in 4 (22.2%). In diffuse tumors, lack of staining was rare (N=1; 11.1%), 6 (66.7%) and 2 (22.2%) tumors showed a poor and medium staining intensity, respectively Staining intensities in plexiform neurofibroma (N=21) were either poor (N=12; 57.1%) or medium (N=9; 42.9%). Staining intensities in MPNST was markedly distributed over different grades: no staining (N=2; 22.2%), poor (N=5, 55.6% and medium (N=2; 22.2%). Strong staining for bFGF was absent in all entities of this study. Results are depicted in Figure 4.
Increased cytoplasmic bFGF expression was associated with increased cytoplasmic VEGF expression (r=0.289, p=0.017, N=58). Immunoreaction of bFGF antibody in these tumors is illustrated in Figure 1C.
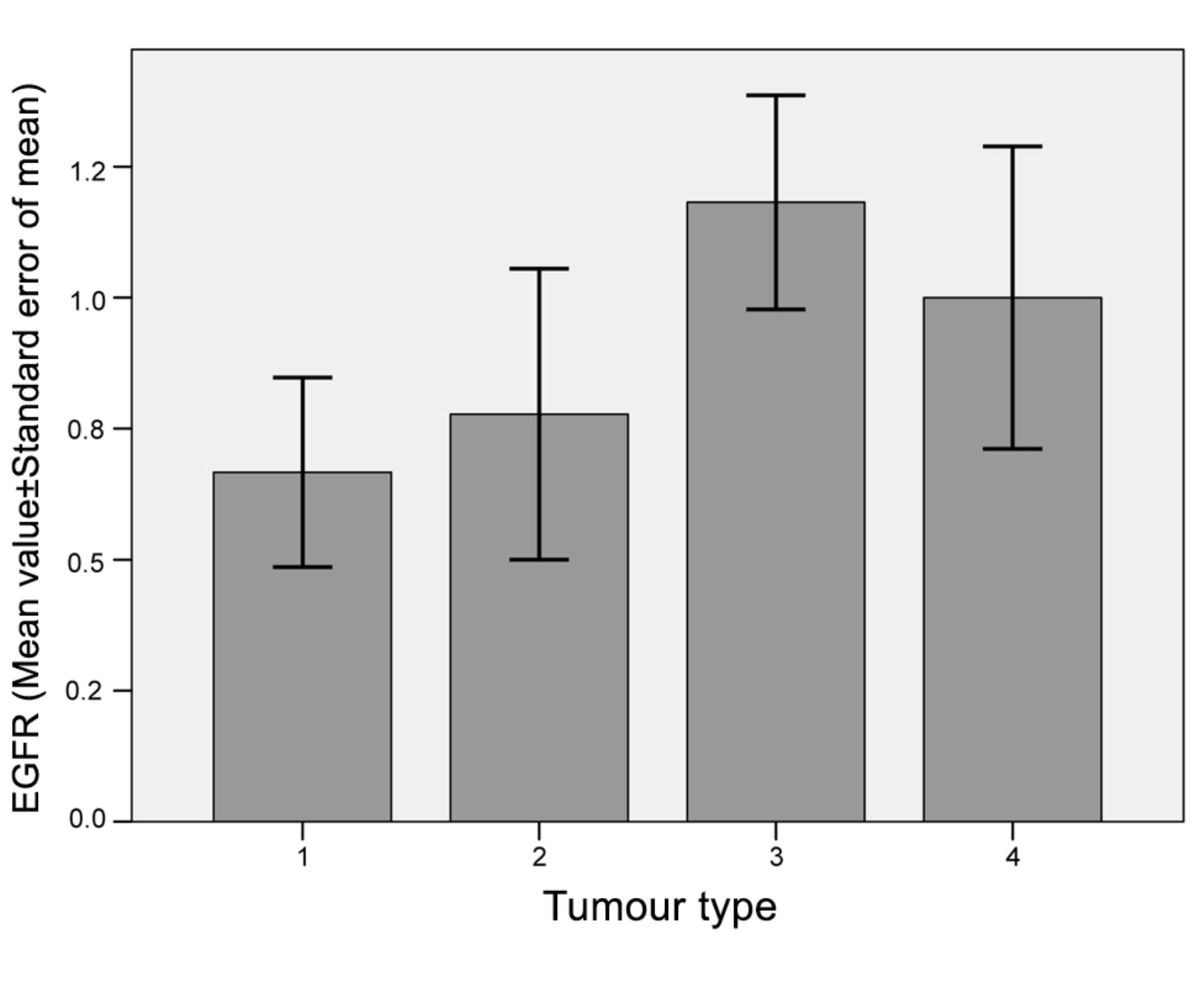
EGFR. Half of dermal neurofibromas showed no expression of EGFR (N=9) and staining intensity was poor in further 6 cases (33.3%). Medium staining intensity was restricted to 3 cases (16.7%). A similar distribution of staining patterns was observed in diffuse neurofibroma (no staining: 4 (44.4%), poor staining: 3 (33.3%), medium staining: 2 (22.2%)). The staining intensities for EGFR in plexiform neurofibroma differed from the dermal types (no staining: 5 (23.8%), poor staining: 8 (38.1%), medium staining: 6 (28.6%) and strong staining: 2 (9.5%)) (Figure 1D). MPNST expressed EGFR in different intensities (no staining: 3 (33.3%), poor staining: 3 (33.3%) and medium staining: 3 (33.3%)). Results are summarized in Tables I and II and Figure 5.
Expression of EGFR and tumor type showed no correlation. Furthermore, EGFR expression did not correlate to other antigens investigated in the present study. However, staining intensity increased for all growth factors comparing tumor group 2 and 3 (Figure 5).

(A) Staining for VEGF in dermal/diffuse neurofibroma and (B) plexiform neurofibroma. (C) Staining of bFGF in dermal neurofibroma and (D) staining of EGFR in a plexiform neurofibroma of a 13-year old patient. For scale see Figure 2A.
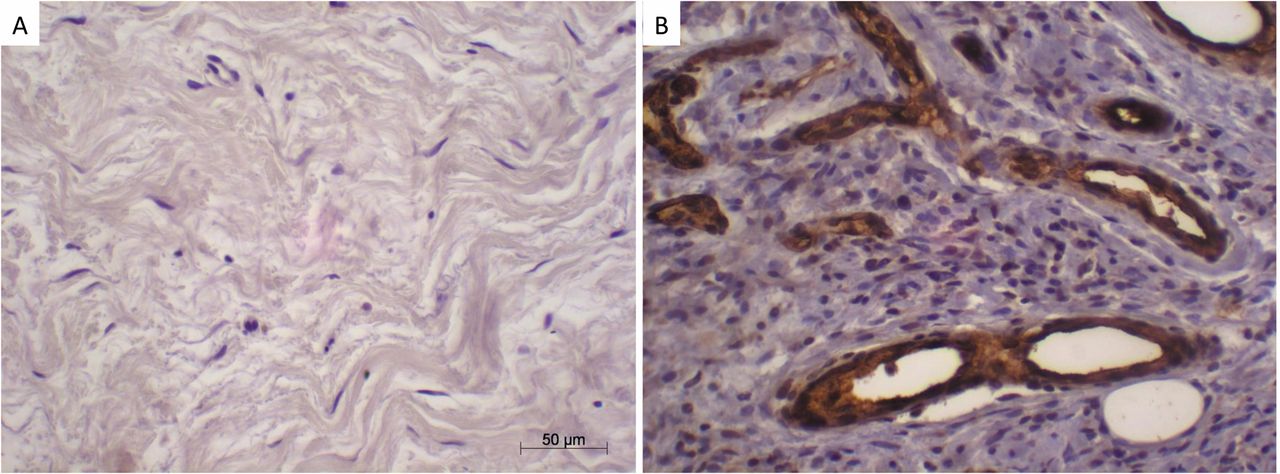
(A) Staining of EGFR in a plexiform neurofibroma of a 70-year old patient. (B) Staining of factor VIII in MPNST. Scale in A applies to all histophotographs.
Staining pattern according to grading of nerve sheath tumors in NF1 for vascular endothelial growth factor (VEGF), basic fibroblastic growth factor (bFGF) and epidermal growth factor receptor (EGFR).
Mean values of staining reactions of growth factors/receptors and vessel density vs. tumor type.
EGFR expression was markedly increased in younger patients (r=-0.238, p=0.032, N=58). The difference is likely to be attributed to the higher number of MPNST in young patients (Table III and Figure 6).
Vessel densities. The density of vessels inside a peripheral nerve sheath tumor correlated to the tumor type (r=0.249, p=0.014, N=58). Vessel density increased significantly from benign neurofibroma to MPNST (Table II and Figures 2b and 7).
Tumor type and localization. Tumor type and localization correlated (r=−0.258, p=0.028, N=57). Plexiform neurofibroma was preferentially resected in large nerves and plexus, i.e. in the trunk, whereas dermal neurofibroma was disseminated all over the integument (Table IV).
Discussion
This study reveals connections between different angiogenic factors and tumor types of peripheral nerve sheath origin in NF1-affected individuals. This study shows an increased VEGF expression of plexiform neurofibroma compared to dermal and dermal/diffuse neurofibroma but no increased vessel density.
An explanation for increased VEGF expression could be the morphological composition of this tumor type. Plexiform (nodular) neurofibroma is surrounded by a capsule in contrast to dermal tumors that show poorly-defined borders. A transmural diffusion of VEGF to the tissue outside the capsule may be hampered by this condition.
Increased vessel densities were found in MPNST. This finding is in accordance with an earlier report by Angelov et al. (12) who noted a significantly increased vessel density and VEGF expression in MPNST compared to unaffected nerve tissues. Gesundheit et al. (5) reported a change in vessel quality and an additional inflammatory component (invasion of leucocytes and micro-bleeding) in the process of transition from plexiform neurofibroma to MPNST. The authors also described an increase of VEGF and vessel density in MPNST compared to plexiform neurofibroma but did not investigate dermal neurofibroma. On the other hand, others revealed an increased VEGF expression in MPNST and normal Schwann cells compared to neurofibroma (13). It is presently unknown how the increase in vascular growth is triggered in neurofibroma during the transformation to a malignant phenotype. It is likely that the expression of angiogenic and anti-angiogenic factors are balanced in plexiform neurofibroma and, therefore, these tumors usually grow very slowly. The transformation to MPNST could be explained by an increase of VEGF receptors (VGFR) rather than increase in VEGF expression.

Tumor type vs. VEGF in cytoplasm. Tumor type 1, dermal; 2, dermal/diffuse; 3, plexiform; 4, MPNST. VEGF, vascular endothelial growth factor; *p<0.05.
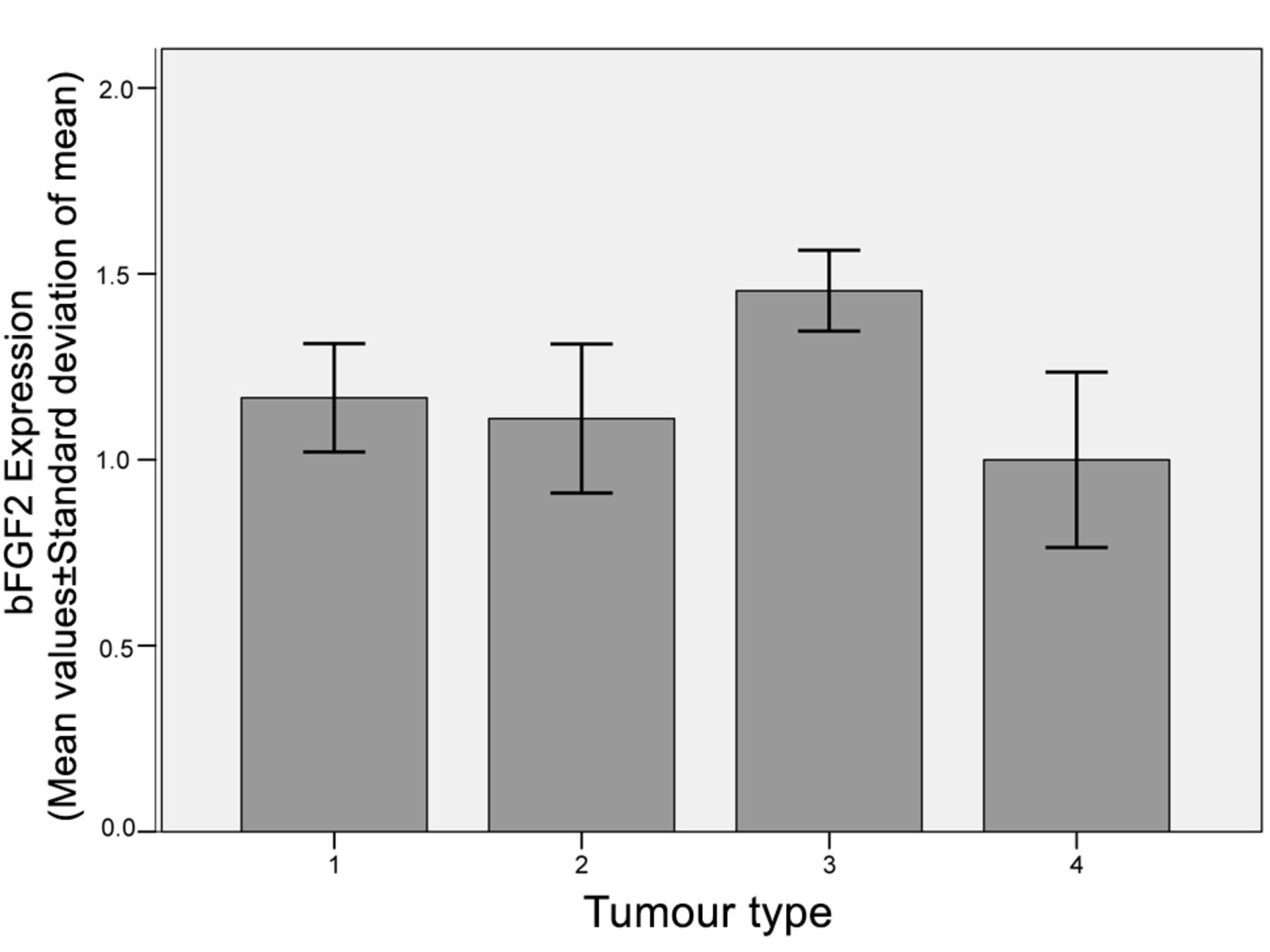
Tumor type vs. bFGF in cytoplasm. Tumor type 1, dermal; 2, dermal/diffuse; 3, plexiform; 4, MPNST; bFGF, basic fibroblast growth factor.
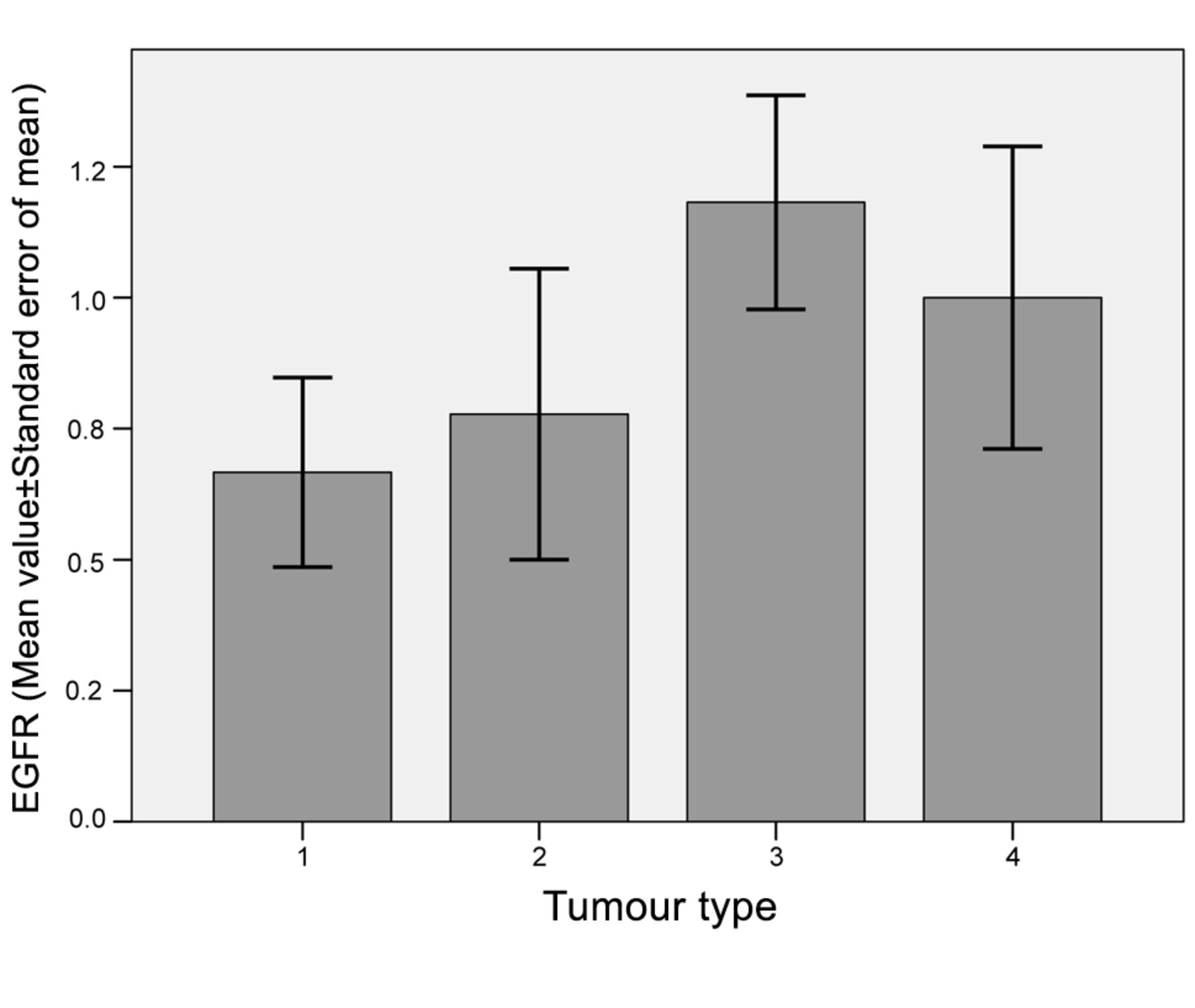
Tumor type vs. EGFR in cytoplasm. Tumor type 1, dermal; 2, dermal/diffuse; 3, plexiform; 4, MPNST; EGFR, epidermal growth factor receptor.

Age (decades) vs. EGFR in cytoplasm. *p<0.05. EGFR, epidermal growth factor receptor.
The lack of increased vessel density in PNF, despite increased VEGF, could possibly be attributed to the low expression of VEGFR. VEGFR was predominantly, but not exclusively, expressed in endothelia (5). VEGF as a ligand to this receptor is expressed by tumor cells, among other types of cells constitutive for a neurofibroma. The increased VEGF expression could, at least in part, be involved in tumor growth of neurofibroma. Zietsch et al. (14) demonstrated the expression of VEGF in peripheral nerve sheath tumors and revealed a linkage between the expression of this factor and progression of malignancy. An interrelationship between increased VEGF and VEGFR expression and transformation of plexiform neurofibroma to MPNST was confirmed by another report (5). In the latter report VEGF was not detected in the cytoplasm of tumor cells of plexiform neurofibroma but in those of MPNST (5). The present study demonstrates VEGF in the cytoplasm of plexiform neurofibroma. On the other hand, the increased VEGF expression in MPNST could not be confirmed in general. Although it was possible to reveal an increase of VEGF in MPNST, the increase was most impressive comparing diffuse to plexiform neurofibroma and did not further increase in MPNST.

Tumor type vs. vessel density. Tumor type 1, dermal; 2, dermal/diffuse; 3, plexiform; 4, MPNST, *p<0.05.
A further interesting fact concerning vessel density and growth factors in tumors is the observation of mast cells in the environment of tumor cells. Mast cells are capable to transmit inflammatory stimuli and are regarded stimulators of angiogenesis in different types of tumors. Ch'ng et al. demonstrated a correlation between the peritumoral mast cell density and microvascular vessel density on one side and the progression and prognosis in melanoma (15). Mast cells in melanoma and basal cell carcinoma contain several factors stimulating angiogenesis, e.g. bFGF and VEGF. In fact, these cells constitute the major source for these factors in these tumors (15). According to Crivellato et al. (16), the capability of mast cells to produce and secrete angiogenic cytokines (e.g. VEGF and FGF-2) is the major factor of tumor development and metastasis because these factors contribute to the angiogenic switch. As already shown by Zhu et al. (17) Nf heterozygous mast cells occur in peritumoral tissues and invade into peripheral nerves prior to the development of plexiform neurofibroma. However, recent studies revealed equal distribution of mast cells in dermal and plexiform neurofibroma of NF1 patients (11). This report is in line with the present finding that increase of vessel density occurred only in MPNST.
Tumor type vs. age.
Tumor type vs. localisation.
Increased bFGF expression was noted in neurofibroma compared to normal Schwann cells. This factor was also increasingly expressed in MPNST. However, this difference was not as obvious as in neurofibroma (13). The present study could not reveal a different expression of bFGF according to tumor type. This study confirms the correlation between cytoplasmic expression of bFGF and VEGF in neurofibroma. This correlation is understandable by reference to the known paracrine and autocrine mechanism of bFGF leading to increased VEGF expression in endothelial cells of developing capillaries, as already demonstrated by Seghezzi et al. (18). Recently, the impact of bFGF on VEGF expression was also reported by Murakami and Simons (19).
Additional growth factors that are involved in angiogenesis of neurofibroma were also investigated. Lichtenberger et al. (20) revealed synergistic effects of VEGF and EGFR signal cascades in epithelial tumors. The effect was that VEGF over-expression was caused by EGFR. Furthermore, the authors revealed cessation of further tumor growth after withdrawal of VEGF and EGFR (20). Fujiyama et al. (21) as well showed expression of VEGF via activation of the EGFR/ERK cascade. This clear relationship between VEGF and EGFR expression was not evident in the present study. Although the expression rate of both parameters increased from dermal/dermal-diffuse to plexiform neurofibroma and MPNST, these increases were statistically not significant.
In general, the present study shows a difference of all growth factor and receptor expressions for dermal neurofibroma (tumor groups 1 and 2) and plexiform neurofibroma (tumor groups 3 and 4). However, this difference was statistically significant for VEGF only. One reason for the restricted correlations of findings could be the method of investigation that allowed no quantitative measurements.
This study revealed a significant correlation between EGFR expression and age of patients. Young patients appear to express more EGFR than older ones. The expression rate declines most at the transition from the first to second decade of life and stabilizes after that period throughout the further decades. These findings are in line of other reports based on animal studies that revealed a reduction of EGFR expression in aged rat brains and rat livers (22, 23). Another study revealed an age-dependent reduced EGFR expression in olfactory epithelia. The reduction of EGFR was associated with reduced cell proliferation and atrophy of olfactory epithelia (24). These findings were confirmed in humans (25). However, the increase of EGFR expression in this study could, at least in part, be attributed to the types of tumor constituting the age groups. A considerable number of MPNST were diagnosed in this early-life period and these tumors show a higher expression of EGFR than neurofibroma (26). Other tumors show a higher EGFR expression associated with higher age of patients. This relationship could not be proven in the current study. EGFR was used as a prognostic factor for calculation of outcome in glioblastoma multiforme (27) and is over-expressed in malignancies, e.g. MPNST (28, 29). EGFR expression was higher in NF1-associated MPNST than in sporadic cases (30). In this study, no significant correlation was proven between EGFR expression and tumor type or malignant transformation.
The correlation of tumor type and topography of tumors is in line with previous reports (31, 32).
The growth factors investigated in this study are targets of potential therapies in the treatment of peripheral nerve sheath tumors. Lichtenberger et al. (20) demonstrated a significant reduction of epithelial tumors after EGFR suppression and also a negative effect of VEGF inhibition on tumor growth. Similar observations were published showing a reduced VEGF expression following EGFR antibody application (33). However, a resistance to EGFR antibodies was also noted accompanied with VEGF over-expression (33).
Blockage of EGFR and other factors mediated tumor progression is a relevant therapeutic strategy of many malignant tumors (6, 12, 20). However, patients under tyrosine kinase inhibitors can eventually develop resistance. The NF1 tumor suppressor gene is occasionally involved in this acquired resistance, e.g. in EGFR-mutated lung cancer (34): the interaction of factors and receptors allows escape mechanisms of cancer cells under chemotherapy.
Conclusion
This study showed the expression profile of several growth factors in NF1-associated peripheral nerve sheath tumors. Expression of factors and receptors varied considerably. These alterations of factor and receptor expression could be attributed to the impaired prediction for pharmacological therapies relying on the suppression of these targets.
Footnotes
-
↵* These Authors contributed equally to this study.
- Received September 3, 2014.
- Revision received October 27, 2014.
- Accepted October 30, 2014.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Peripheral Nerve Sheath Tumors in Patients With Neurofibromatosis Type 1: Morphological and Immunohistochemical Study
- Vascular Innervation in Benign Neurofibromas of Patients with Neurofibromatosis Type 1
- Vessel and Mast Cell Densities in Sporadic and Syndrome-associated Peripheral Nerve Sheath Tumors